
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-121
Complex Long Diffuse Coronary Lesions: Hybrid Revascularization in Action
By Mohd Tawfeq Mohd Noor, Hafidz Abd Hadi
Presenter
Mohd Tawfeq Mohd Noor
Authors
Mohd Tawfeq Mohd Noor1, Hafidz Abd Hadi1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-121
Coronary - Complex PCI - Long Lesion
Complex Long Diffuse Coronary Lesions: Hybrid Revascularization in Action
Mohd Tawfeq Mohd Noor1, Hafidz Abd Hadi1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
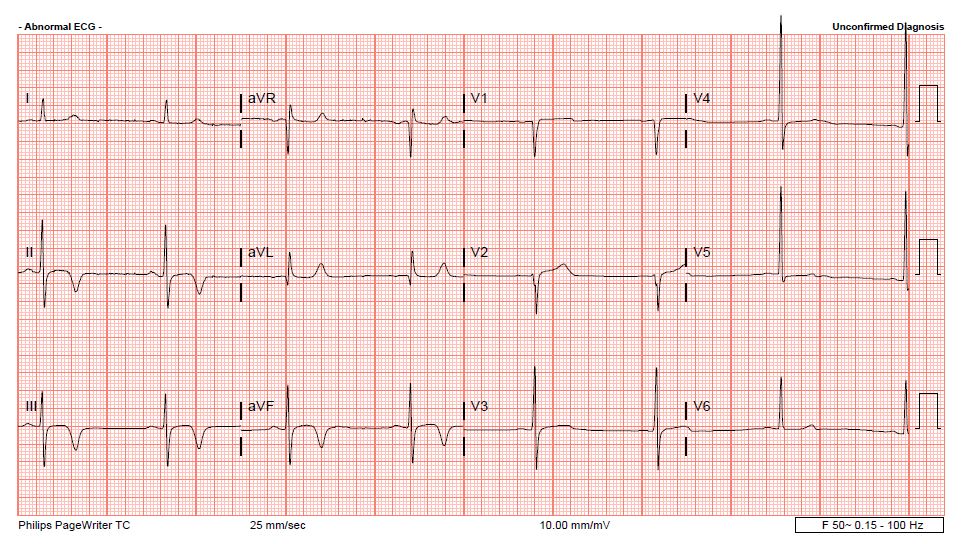
A 65-year-old man with diabetes mellitus, hypertension and dyslipidemia was admitted for non-ST-elevation acute coronary syndrome. He presented with central chest pain for 1 day prior to admission. His vital signs were stable with blood pressure of 130/75 mmHg and heart rate was 50 beats per minute. No significant finding from physical examination. Electrocardiogram showed T waves inversion over the inferior leads.
Relevant Test Results Prior to Catheterization
Troponin T was elevated at 763 pg/ml (normal level less than 14). Echocardiography revealed ejection fraction of 45%. He was then scheduled for coronary angiogram.
Relevant Catheterization Findings
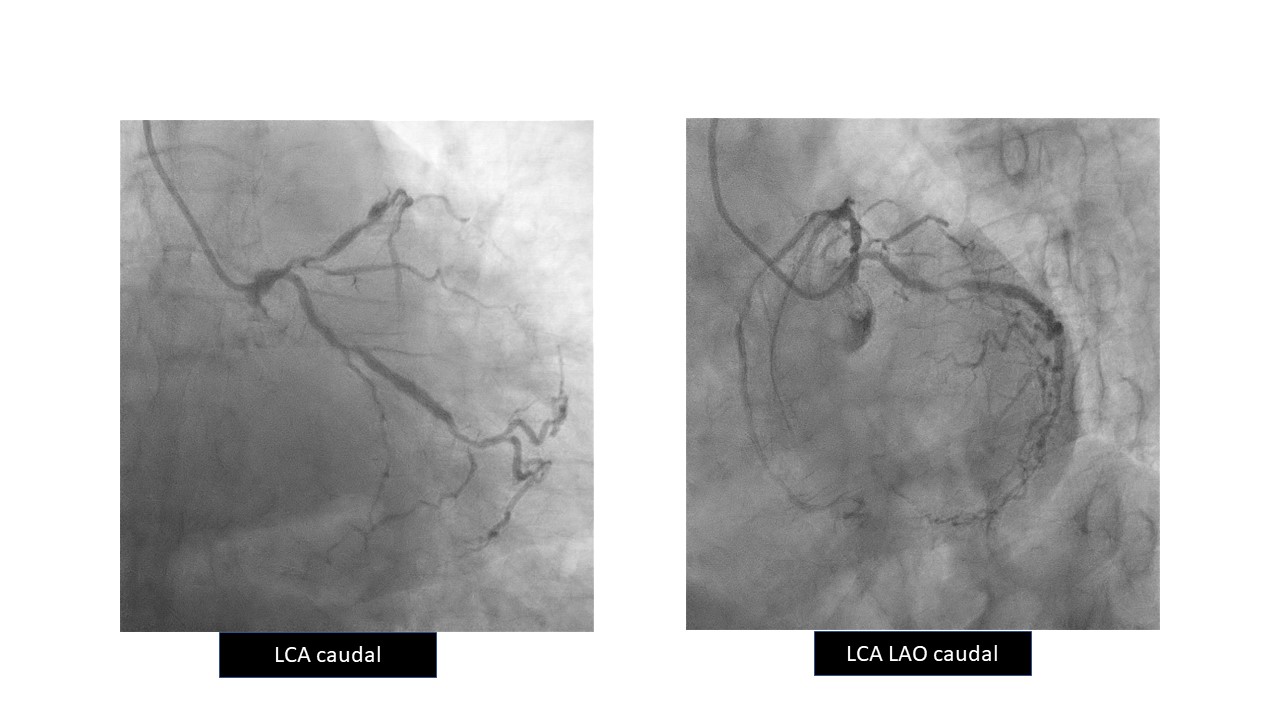
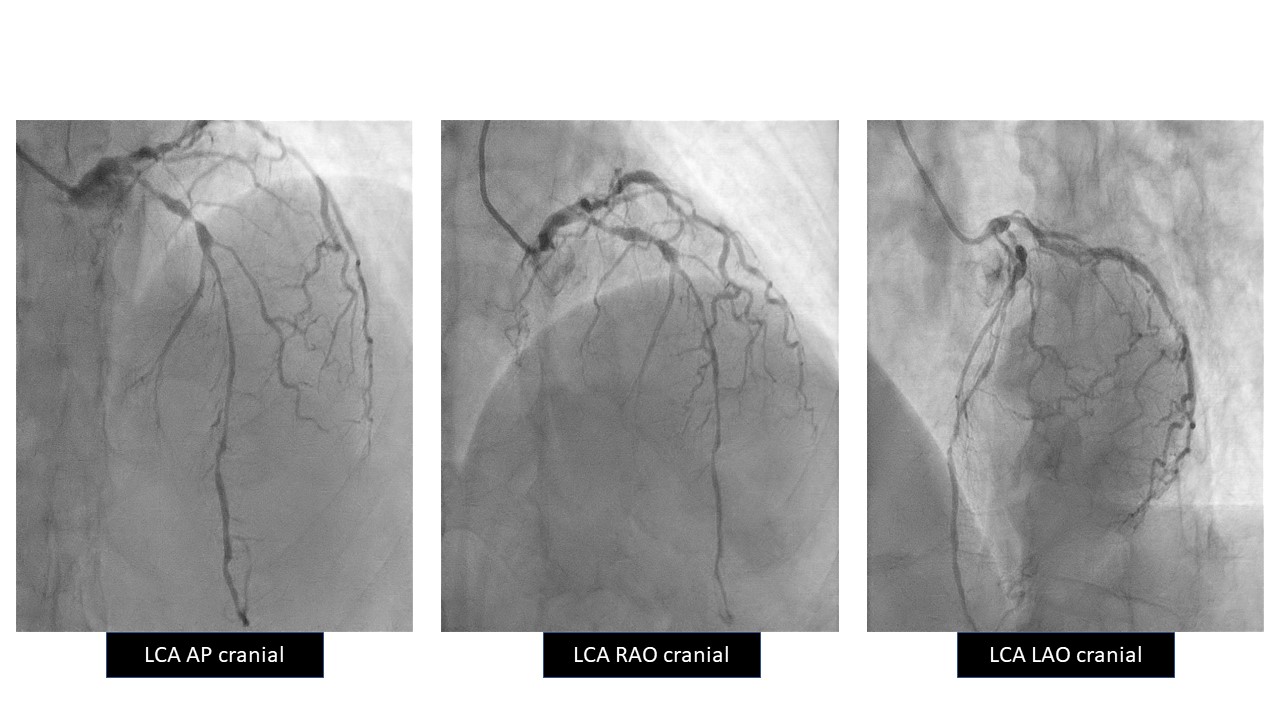
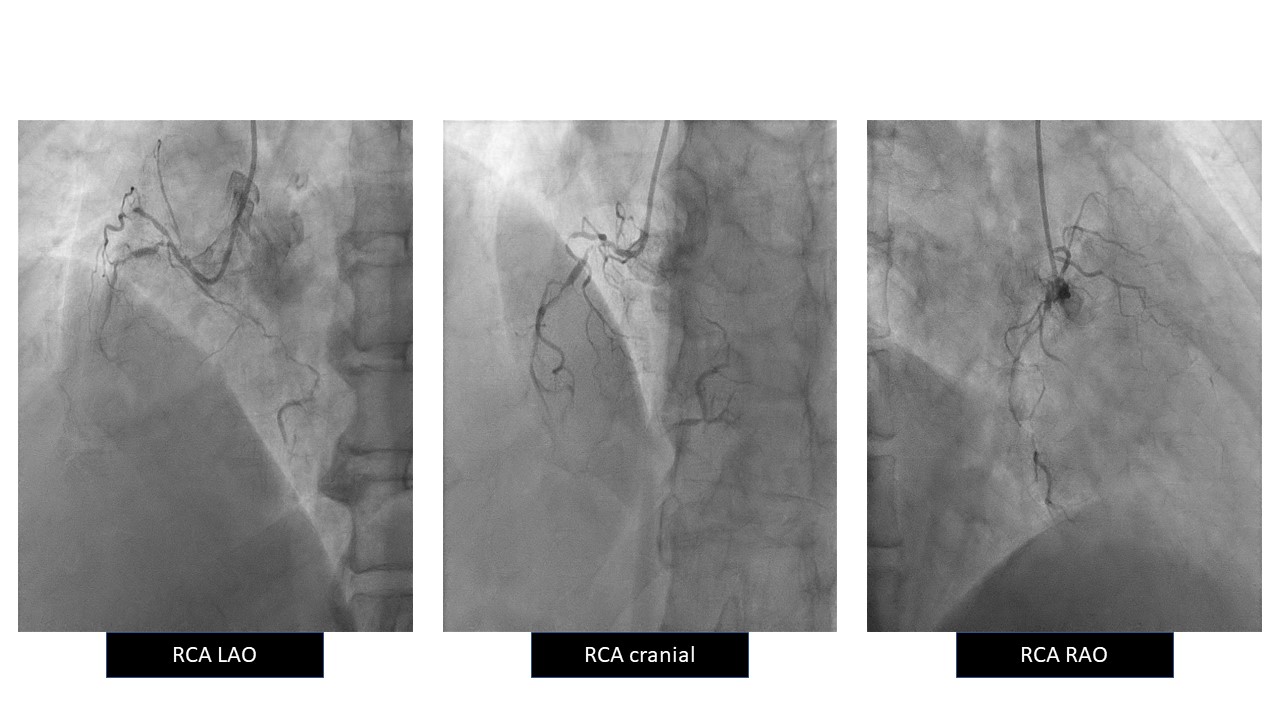
Coronary angiogram revealed severe distal left main (LM) disease with severe, long diffused lesions extending from ostial to distal segments of both left anterior descending artery (LAD) and left circumflex artery (LCX). There was also severe long diffused disease of right coronary artery (RCA) with subtotal occlusion of the proximal segment. Patient was referred for coronary artery bypass surgery, but he refused for surgery. Multi-vessel coronary angioplasty was staged for all 3 vessels.
Interventional Management
Procedural Step
PCI RCA was done using JR 3.5-6 French. Subsequently decided to change to SAL 1.0-6 French for better support due to difficulty in wiring and delivering balloons.
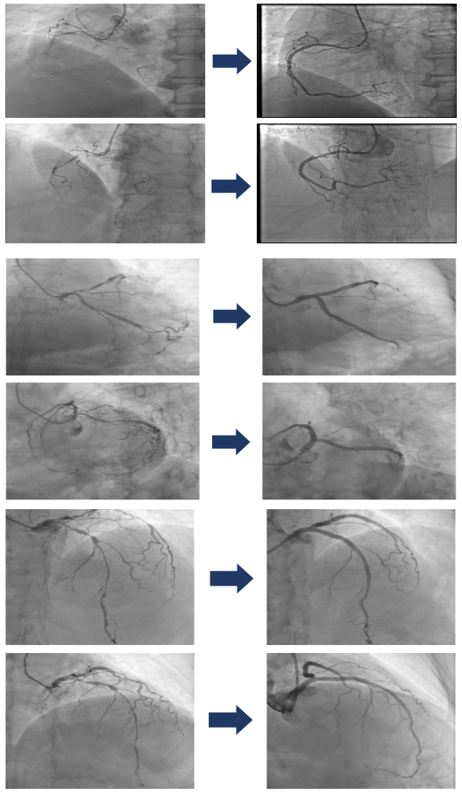
Managed to cross the lesion using Fielder XT. Lesions were prepared with sequential ballooning using 1.5, 2.0 and 2.5 mm balloons.
IVUS done revealed heavy plaque burden from ostial to distal RCA.
Distal RCA was treated with drug coated balloon (DCB) 2.0/30 and 2.5/30.
Stent mid to ostial RCA with drug eluting stent (DES) 2.75/36 and 3.0/36.
Post dilated with high pressure 3.0 and 3.5 non-compliant balloons.
IVUS done showed stent well apposed, no edge dissection.
Decided for upfront 2-stent strategy using double-kissing culotte (DK culotte) technique, IVUS guided with EBU 3.5-7 French.
Prepared distal to proximal LCX lesions with scoring 3.0/15, high pressure proximally.
Initial plan for DCB at distal LCX changed to DES due to dissection at distal segment.
DES 2.75/29 and 3.5/33 deployed at LCX.
After adequate preparation at LM - LAD, DCB distal with 2.5/30, DES at mid with 3.0/38.
LCX to LM stent with 4.0/23, optimized proximally with 4.5/10. LAD rewired and first kiss done with 4.0/15 balloons sub nominal pressure at both LAD and LCX.
Ostial LM to LAD stent with 3.5/38 and optimized proximally. LCX rewired. Stents were post dilated and second kiss done.
Final proximal optimization done with 4.5/10.
IVUS done showed stent well apposed, no edge dissection. TIMI III flow.
Case Summary
The hybrid revascularization strategy using DES and DCB is well-suited for managing long diffuse coronary lesions in complex PCI. By deploying DES in focal segments that require structural support and DCB in diffuse areas to reduce metal load, this approach not only minimizes restenosis risk but also preserves vessel integrity. Importantly, the reduced metal burden maintains surgical options for future coronary artery bypass graft if needed, providing flexibility in the patient’s long-term treatment plan. This strategy enhances immediate revascularization outcomes while keeping future treatment pathways open.