
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-006
Left Main ST-Segment Elevation Myocardial Infarction in Takayasu Arteritis With Aorto-Ostial Coronary Involvement: A Complex and Rare Case Report
By Archan Jaspattananon, Tharinee Sirithanasart
Presenter
Archan Jaspattananon
Authors
Archan Jaspattananon1, Tharinee Sirithanasart2
Affiliation
Vachira Phuket Hospital, Thailand1, Bangkok Phuket Hospital, Thailand2,
View Study Report
TCTAP C-006
Coronary - ACS/AMI
Left Main ST-Segment Elevation Myocardial Infarction in Takayasu Arteritis With Aorto-Ostial Coronary Involvement: A Complex and Rare Case Report
Archan Jaspattananon1, Tharinee Sirithanasart2
Vachira Phuket Hospital, Thailand1, Bangkok Phuket Hospital, Thailand2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 41-year-old female with a history of migraine presented to the emergency department with 3-day history of intermittent chest pain radiating to the jaw and left arm. The pain became severe and persistent 2 hours prior to presentation. The physical examination was unremarkable.
Relevant Test Results Prior to Catheterization
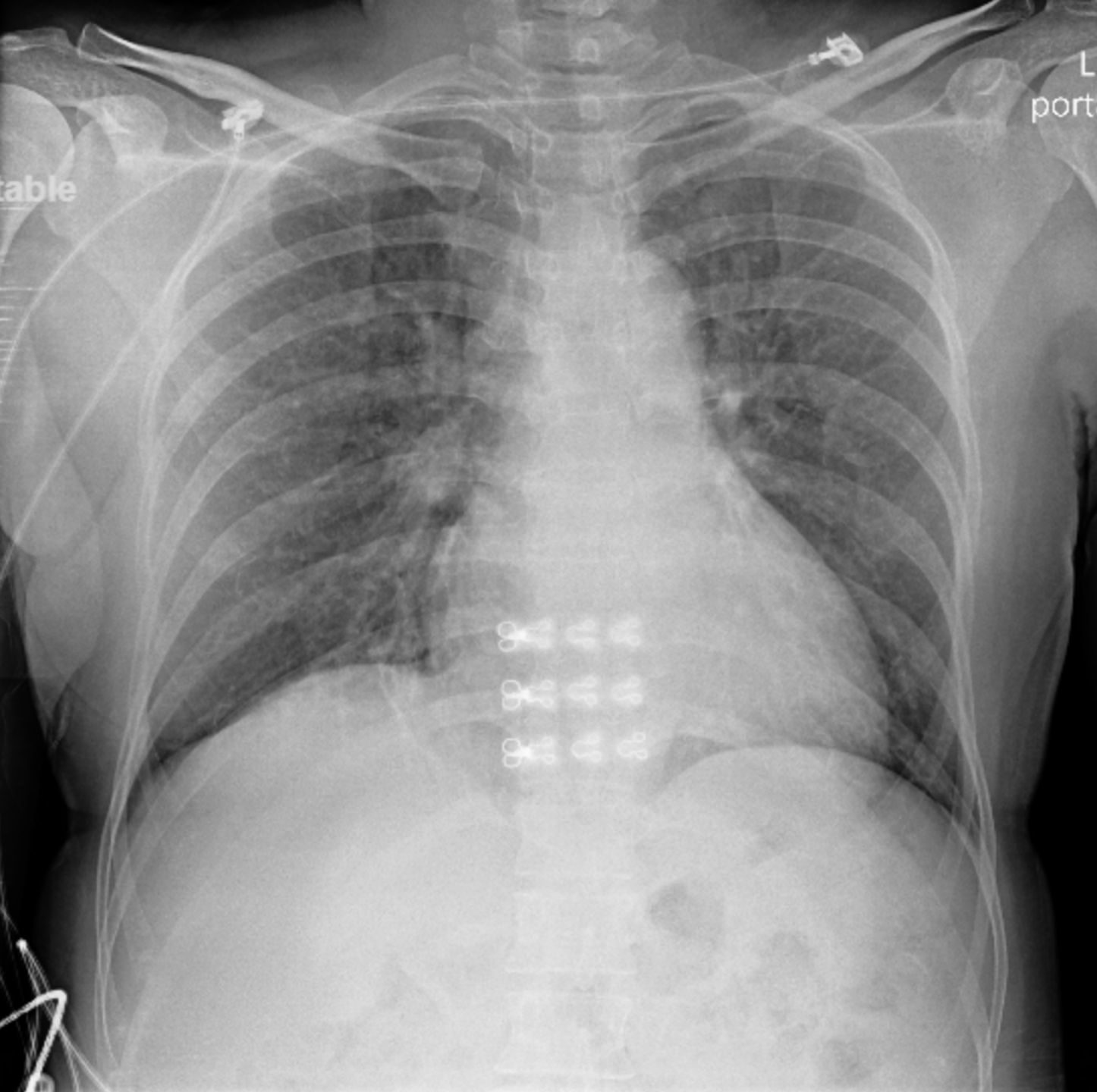
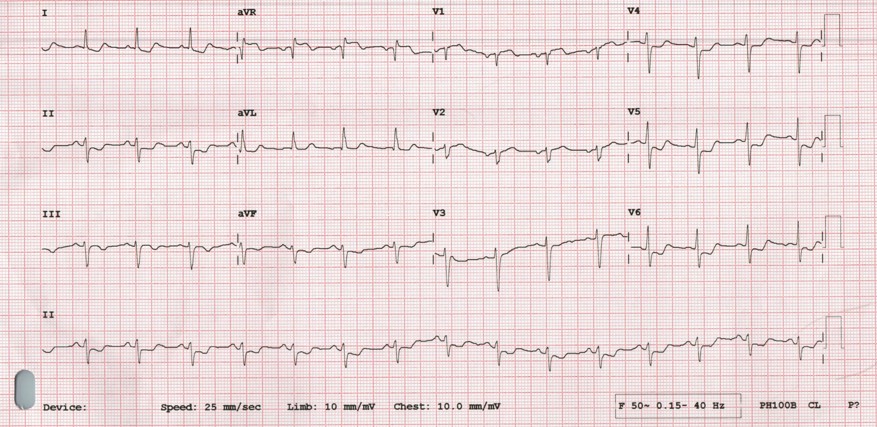
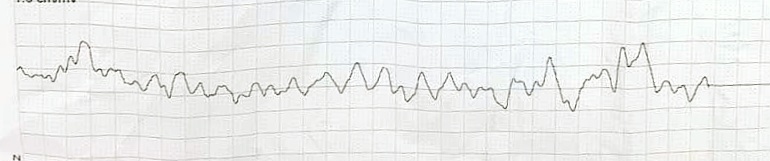
Initial electrocardiogram demonstrated diffuse ST-segment depression with ST-elevation in leads aVR and V1. The patient subsequently developed ventricular fibrillation requiring immediate cardiopulmonary resuscitation and defibrillation. During emergency transfer to the cardiac catheterization laboratory, she experienced recurrent ventricular fibrillation and profound cardiogenic shock.
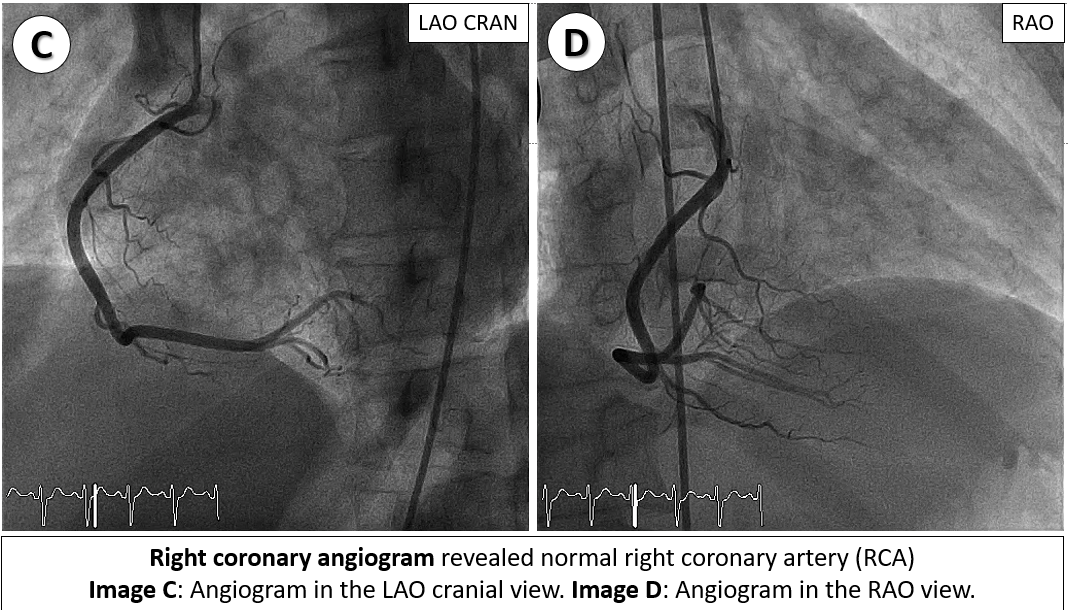
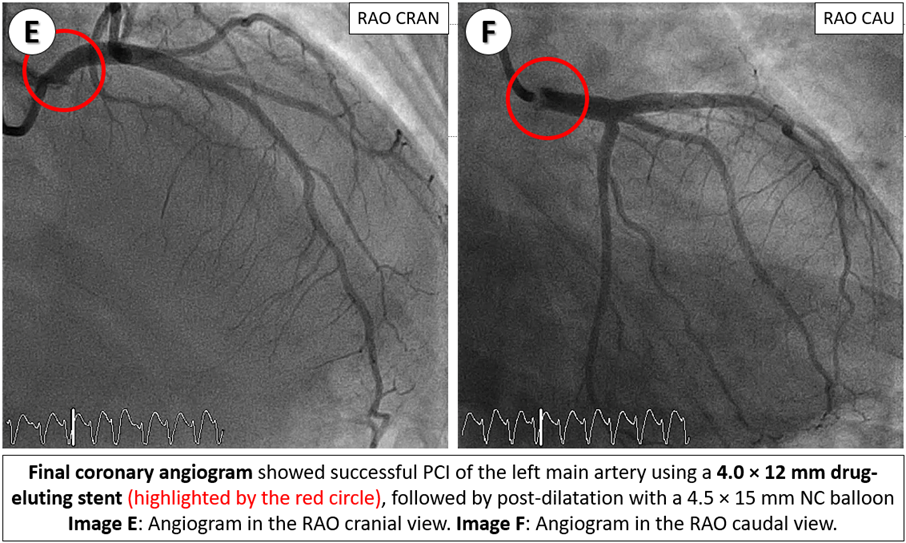
Relevant Catheterization Findings
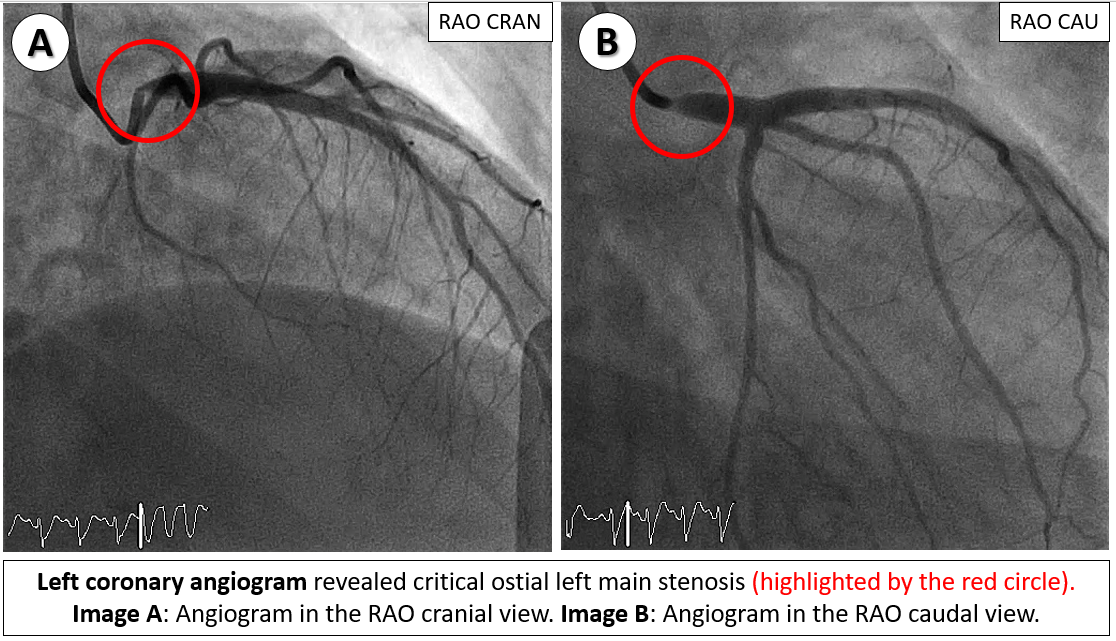
Emergency coronary angiography revealed a critical ostial left main stenosis with TIMI 2 flow and a normal right coronary artery. Following engagement with 6-Fr JL 4.0 side-hole catheter, sequential pre-dilatation was performed using 3.5x15 mm and 4.5x15 mm non-compliance (NC) balloons. A 4.0x12 mm drug-eluting stent was deployed in the left main artery, followed by post-dilatation with a 4.5x15 mm NC balloon. Subsequently, an intra-aortic balloon pump was inserted for hemodynamic support.
Interventional Management
Procedural Step
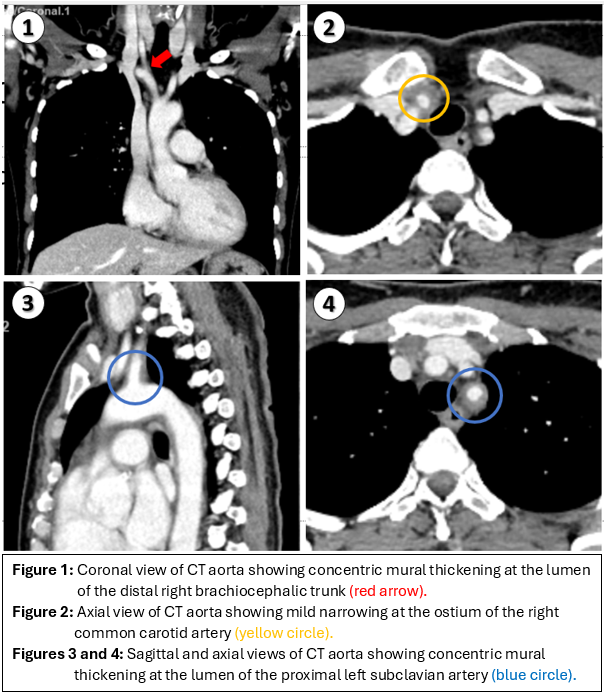
Initial investigations showed favorable lipid profile (LDL51 mg/dl) and HbA1C level of 4.9%. Considering the presence of isolated aorto-ostial disease leading to acute left main STEMI, further investigations were conducted to assess for aortitis, including ankle-brachial index and serology for antinuclear antibody (ANA), antineutrophil cytoplasmic antibody (ANCA), rheumatoid factor, syphilis, and HIV, all of which were negative. However, the patient demonstrated elevated levels of erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), indicative of systemic inflammation. A computed tomography angiography (CTA) of the whole aorta revealed concentric mural thickening in the lumen of the distal right brachiocephalic trunk, proximal right common carotid artery, proximal right subclavian artery, and proximal left subclavian artery with mild narrowing at the ostium of the right common carotid artery. These findings were suggestive of Takayasu arteritis type I.
Case Summary
This case highlights a rare presentation of Takayasu arteritis manifesting as left main ST-elevation myocardial infarction (STEMI). It is important to recognize the underlying inflammatory arteritis in patients presenting with STEMI in the absence of atherosclerotic risk factors.