
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-003
Importance of a Systematic Approach With Structural and Physiological Testing in the Diagnosis of Myocardial Infarction With Non-Obstructive Coronary Arteries
By Haruyuki Deguchi, Takashi Kubo, Miki Kitamura, Misato Miyamoto, Kazuya Takihara, Yuki Yamashita, Yoshikazu Takeuchi, Taiyo Tezuka, Yoichi Iwasaki, Nobuhiro Tanaka
Presenter
Haruyuki Deguchi
Authors
Haruyuki Deguchi1, Takashi Kubo1, Miki Kitamura1, Misato Miyamoto1, Kazuya Takihara1, Yuki Yamashita1, Yoshikazu Takeuchi1, Taiyo Tezuka1, Yoichi Iwasaki1, Nobuhiro Tanaka1
Affiliation
Tokyo Medical University Hachioji Medical Care Center, Japan1,
View Study Report
TCTAP C-003
Coronary - ACS/AMI
Importance of a Systematic Approach With Structural and Physiological Testing in the Diagnosis of Myocardial Infarction With Non-Obstructive Coronary Arteries
Haruyuki Deguchi1, Takashi Kubo1, Miki Kitamura1, Misato Miyamoto1, Kazuya Takihara1, Yuki Yamashita1, Yoshikazu Takeuchi1, Taiyo Tezuka1, Yoichi Iwasaki1, Nobuhiro Tanaka1
Tokyo Medical University Hachioji Medical Care Center, Japan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
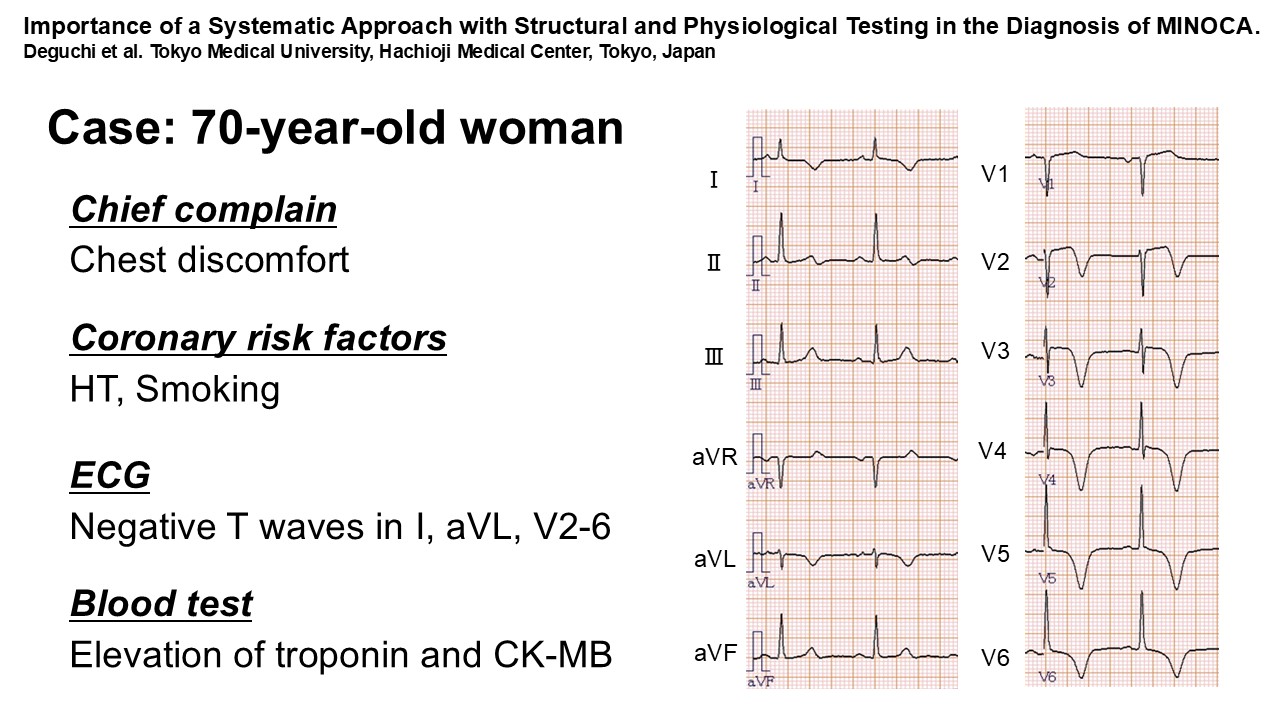
A 70-year-old woman had persistent chest discomfort after exertion. Electrocardiography (ECG) showed giant negative T waves in precordial leads. Blood tests showed elevated serum troponin and CK-MB levels.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
Interventional Management
Procedural Step
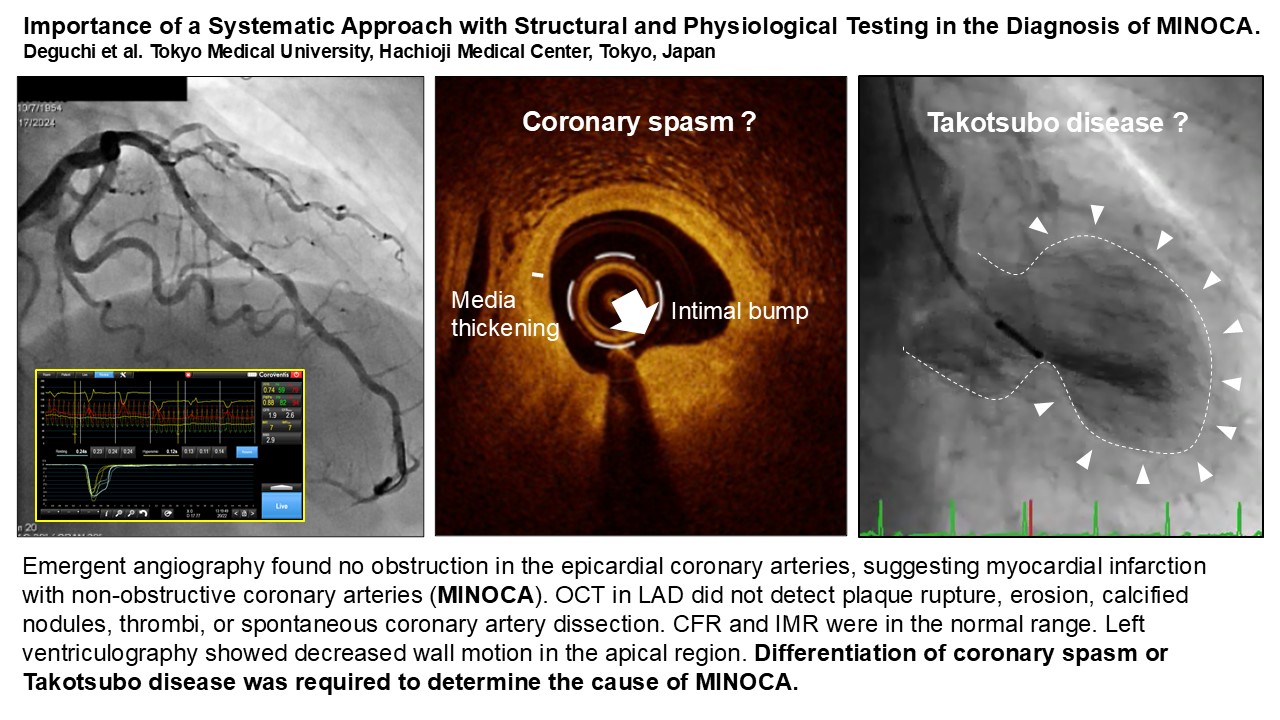
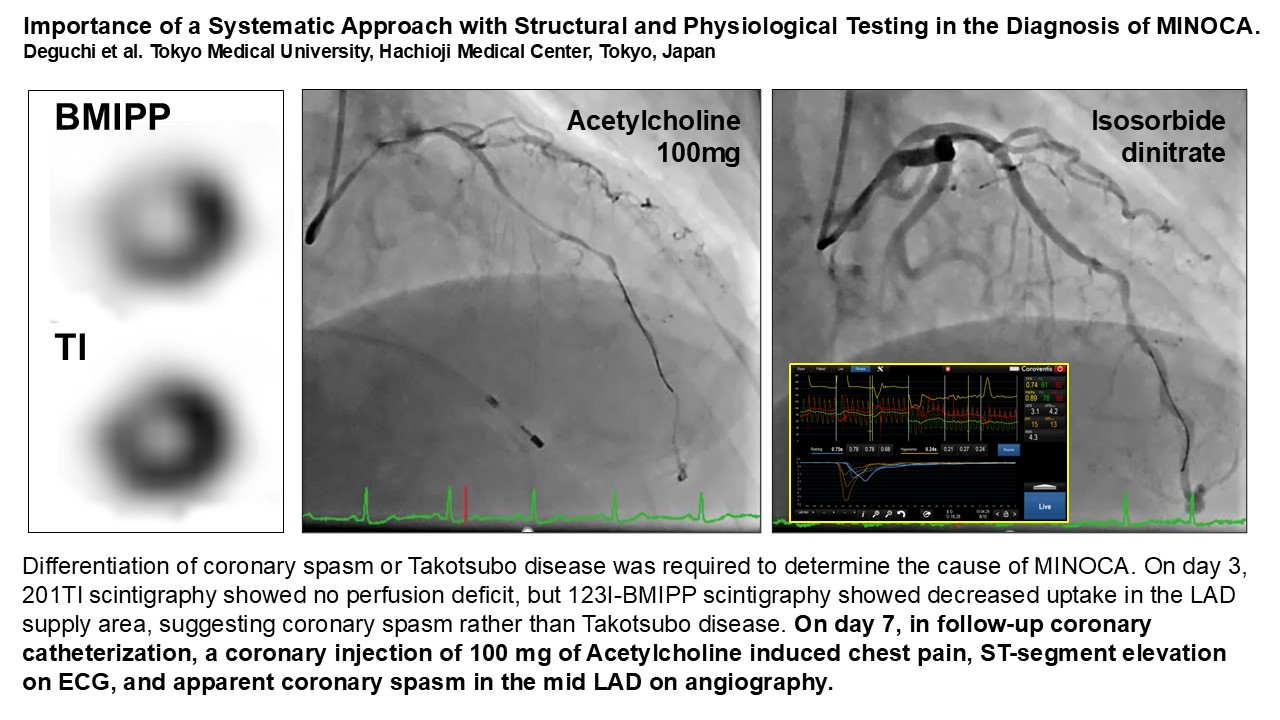
Emergency coronary angiography found no obstruction in the epicardial coronary artery and identified only mild stenosis in mid portion of the large left anterior descending artery (LAD). This case was considered myocardial infarction with non-obstructive coronary arteries (MINOCA). We performed further tests to elucidate the cause of MINOCA. Optical coherence tomography (OCT) in LAD did not detect plaque disruption, erosions, calcified nodules, thrombi, or spontaneous coronary artery dissection. Coronary flow reserve (CFR) and index of microvascular resistance (IMR) were in the normal range. Left ventriculography showed decreased wall motion in the apical region. Differentiation of coronary spasm or takotsubo disease was required to determine the cause of MINOCA. On day 3, 201Tl scintigraphy showed no perfusion deficit, but 123I-beta-methyl-P-iodophenyl-pentadecanoic acid (BMIPP) scintigraphy showed decreased uptake in the LAD supply area, suggesting coronary spasm rather than Takotsubo disease. On day 7, in coronary catheterization, a coronary injection of Acetylcholine 100mg induced chest pain, ST-segment elevation on ECG, and apparent coronary spasm in the mid LAD on angiography.
Case Summary
We conclude that the cause of MINOCA in this case was coronary spasm. This case has been treated with Ca antagonists and has so far had no recurrent cardiovascular events. Through this case, we report the importance of a systematic approach with structural and physiologic testing to identify the cause of MINOCA.