
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-193
Giant RCA Aneurysm
By Raymond Cheung
Presenter
Raymond Cheung
Authors
Raymond Cheung1
Affiliation
Tuen Mun Hospital, Hong Kong, China1,
View Study Report
TCTAP C-193
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
Giant RCA Aneurysm
Raymond Cheung1
Tuen Mun Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
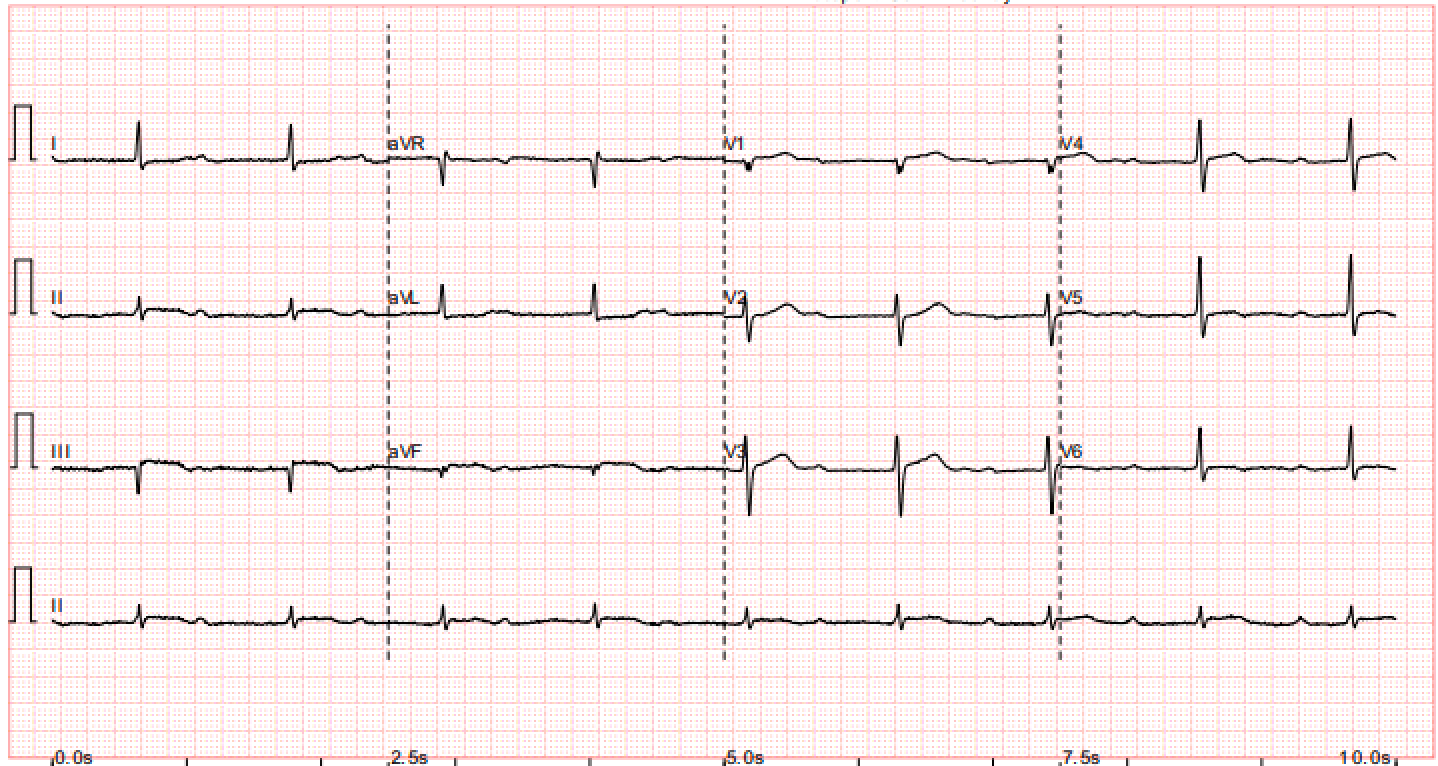
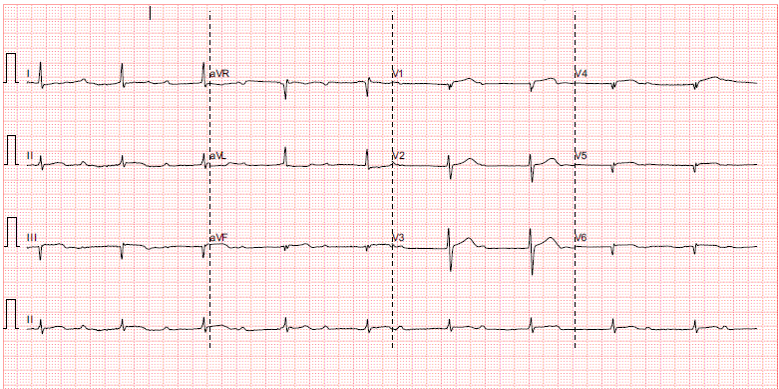
Mr A is a 45 year old construction site worker with unremarkable past health. He is active smoker with 30 pack years. He has no family history of premature CAD. He presented with sudden onset of severe chest pain at 1am. Prehospital ECG showed complete heart block, 50 beats per min, ST segment elevation at inferior leads with right side involvement.
Relevant Test Results Prior to Catheterization
His vitals are stable: BP 160/116 P53 SpO2 98% RA Hstix 15
Bloods tests are grossly unremarkable. Troponin 218 (<= 34.2) CK 412
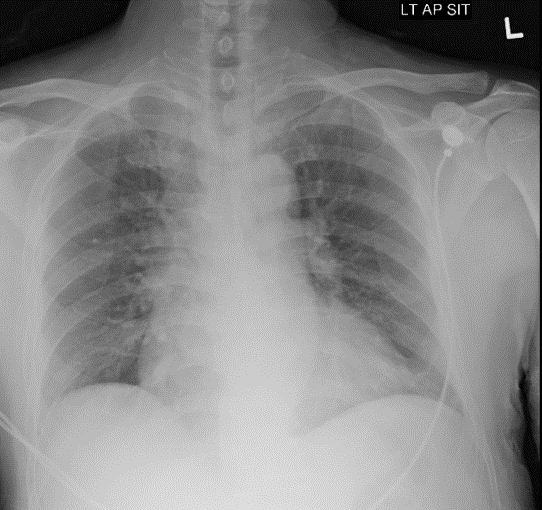
CXR is clear
Echo shows impaired LV systolic function, EF ~ 45%, inferior wall hypokinesia. Dilated RV Mild MR. no AR. mod TR. No pericardial effusion.PPCI is activated. He is sent to catherization lab immediately.
Relevant Catheterization Findings
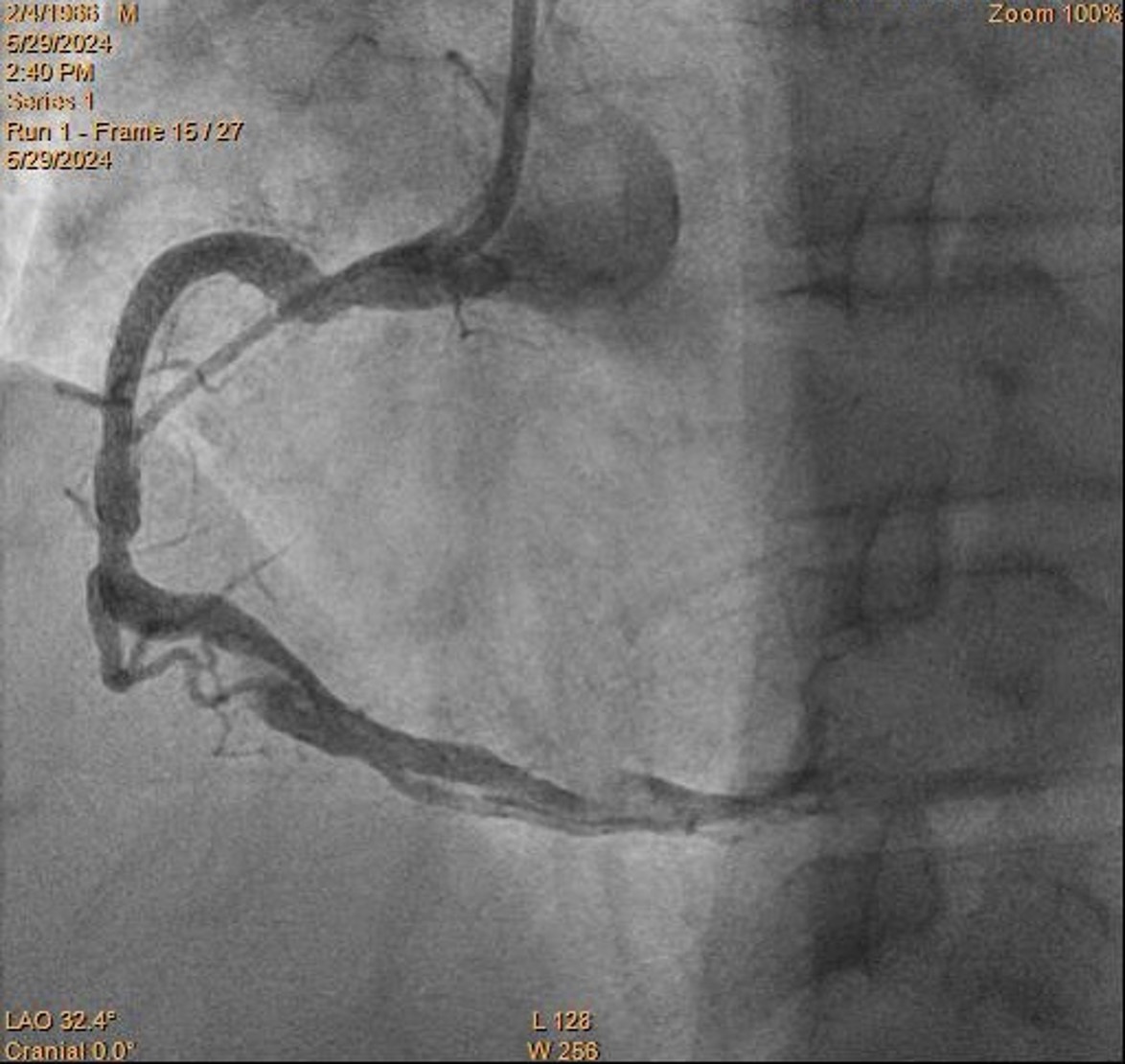
Coronary angiogram: LMS: normalLAD: diffuse disease up to 40% stenosis over p-mLADLCX: minor diseaseRCA: pRCA total occlusion with ? flapIRA = RCAPlan: PPCI to RCA
Interventional Management
Procedural Step
RCA is engaged with JR4.
Initially coronary dissection is suspected as pathology due to unusual angio appearance.
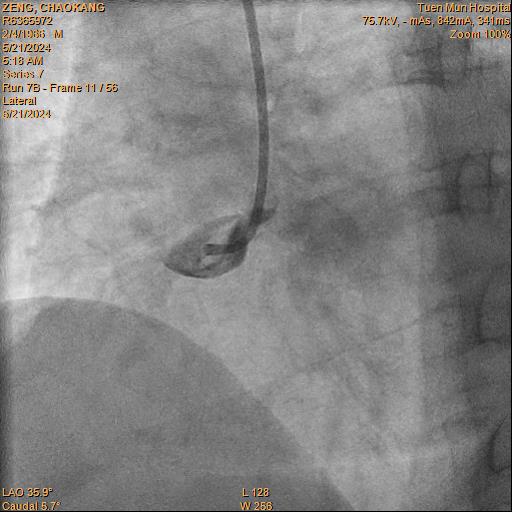
Difficult wiring is noted partly due to uncertain pathology. Eventually RCA is successful wired with Sion Black to distal. IVUS then confirmed giant pRCA coronary aneurysm with a large thrombus.
Size of aneurysm exceeded the US scan limits for measurement and angiographically > 10 mm. Multiple dilatation is attempted with 2.0 and 3.0 balloons, followed by clot aspiration with CAT Rx. . Despite of that, RCA remains in totally occluded with TIMI 0 flow.
Patient reported ongoing pain. Decided to proceed with stenting with the acknowledgement of likely malapposed proximal stent. Onyx Frontier 5.0/30 is deployed over proximal-mid RCA.. IVUS showed no stent edge dissection and malapposed proximal stent edge as expected.
The stent is dilated with 6.0 balloon. Integrellin infusion is given. TIMI III flow is restored.
Patient is discharged later with no more chest pain.
Restudy coro is performed 3 months later. Very difficult RCA wiring is noted. RCA is wired with NS Runthrough, but failed to deliver IVUS. Second Runthrough wire crossed with crusade. IVUS showed stent landed on distal edge of aneurysm. Size of aneursym too big to be measured by IVUS and stented. Thrombus inside aneruysms is noted.
Reviewed is team discussion, it is decided for lifelong anticoagulation and not for further stenting proximally
Case Summary
This presentation shows a case of inferior STEMI with very big RCA aneurysm and thrombus formation inside.
Despite balloon dilatation and thrombectomy, flow is yet to be restored. Flow is restored after stenting. IVUS shows the aneurysm is so big beyond the limit of the machine, with thrombus inside. Stent landed on distal edge of aneurysm. Restudy coro showed TIMI III flow. Difficult rewiring requires use of crusade and 2nd wire. IVUS shows stent malapposed. No available coronary stent is big enough to cover the aneurysm. Reviewed in team meeting, it is decided for lifelong anticoagulation.
Despite balloon dilatation and thrombectomy, flow is yet to be restored. Flow is restored after stenting. IVUS shows the aneurysm is so big beyond the limit of the machine, with thrombus inside. Stent landed on distal edge of aneurysm. Restudy coro showed TIMI III flow. Difficult rewiring requires use of crusade and 2nd wire. IVUS shows stent malapposed. No available coronary stent is big enough to cover the aneurysm. Reviewed in team meeting, it is decided for lifelong anticoagulation.