
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-012
Left Main Stenting in a Patient With Difficult Access and Difficult Anatomy
By Thabish Syed
Presenter
Thabish Syed
Authors
Thabish Syed1
Affiliation
Topstars Hospitals, India1,
View Study Report
TCTAP C-012
Coronary - ACS/AMI
Left Main Stenting in a Patient With Difficult Access and Difficult Anatomy
Thabish Syed1
Topstars Hospitals, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
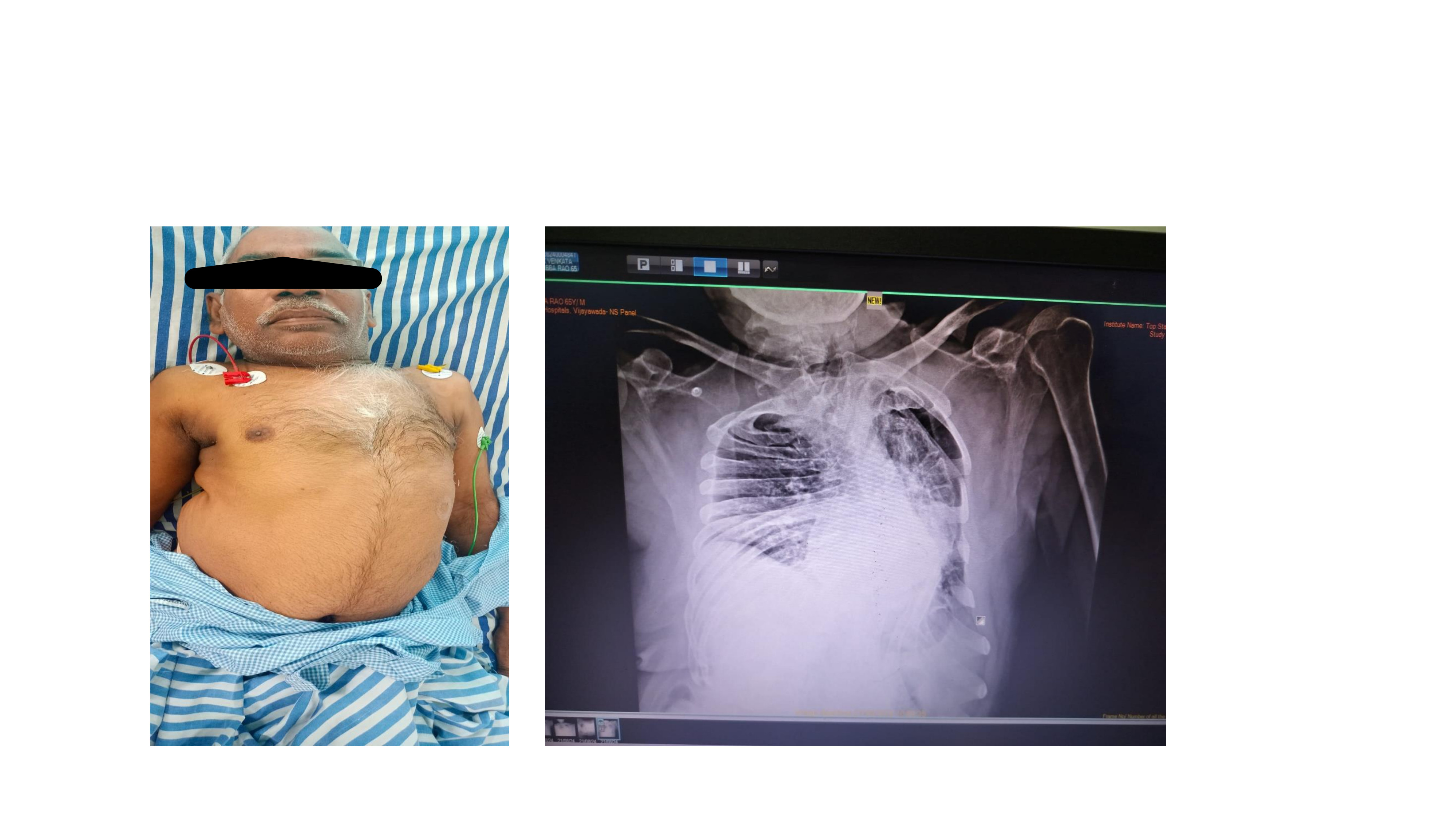
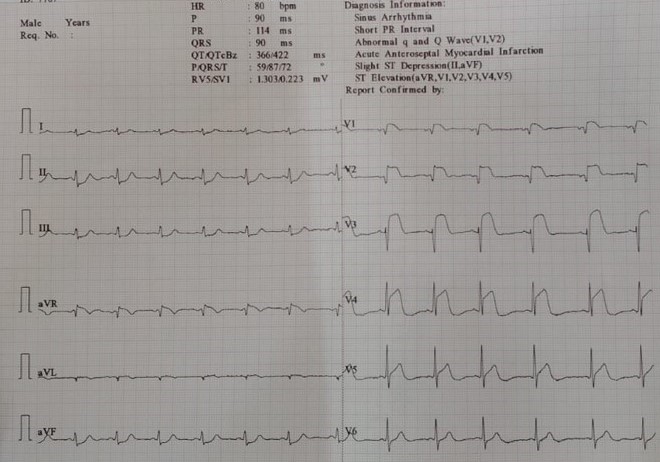
• A 65 Year old male with Kyphoscoliosis and B/L LL polio(Fig 1) presented to ER with chest pain, he was diagnosed as ACS-AWMI lysed outside. On evaluation his HR was 100 bpm, BP 90 Systolic. On examination his chest was clear and normal heart sounds heard. ECG revealed Sinus tachycardia @ 105 bpm and ST elevations in V2-V4(Fig2). 2D ECHO revealed EF of 38% with RWMA in LAD territory. In view of failed lysis, we shifted him to Cathlab for Rescue PCI.
Relevant Test Results Prior to Catheterization
His Hemoglobin was 12 gm%, Serum creatinine was 1.0 mg/dl, Trop I was Positive, NT Probnp- 2400pg/ml and Viral Markers (HIV,HBSAG,HCV) were negative. Chest Xray suggestive of Deformed chest due to kyphoscoliosis with no evidence of pulmonary edema.
Relevant Catheterization Findings
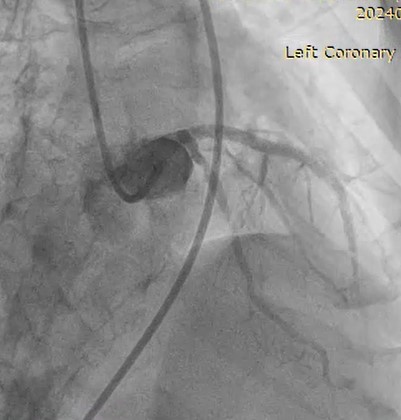
Coronary angiogram revealed- RCA- Normal, LMCA - Normal, LAD - Ostioproximal -99% stenosis followed by Mid 90% stenosis. LCX- Ostium-50% stenosis, mid -90 % Stenosis, after correlating with background spine and diaphragm with angiogram pictures and videos, due to kyphoscoliosis routine views are not validating, forced to adjust views and angles according to anatomy of patient.



Interventional Management
Procedural Step
After seeing angiogram we decided to do cross over stenting from Left Main to LAD, Wiring done to both LAD & lCX, However first difficulty we faced was during passing balloon due to bend near clavicle, Hence both wires removed, shifted to femoral route immediately. Femoral puncture has become very difficult due to bilateral polio of legs, high access taken, again there was acute bend just above iliac bifurcation in addition to huge aortic arch, which made things more difficult as guide support was not good. As patient complaining of persistent chest pain we did not enhance our sheath and proceeded with intervention. LAD ostium predilated with 2.5x 12 mm NC balloon @ 16 atm pressure for 10 seconds followed by Provisional stenting from LM to LAD done with 3.5x 32 mm DES @ 10 atm pressure. POT done with 4.5 x 8mm balloon @ 16 atm pressure for 10 seconds. Distal 3x28 mm another DES overlapping with proximal DES done @12 atm pressure. Post dilatation of LAD done with 3.5 x 15 mm NC balloon @ 20 atm pressure for 10 seconds. Final shot revealed TIMI 3 flow in LAD and LCX, LCX ostium does not look tight enough for intervention , hence no rewiring done as patient is in cardiogenic shock.

Case Summary
This is very interesting case of abnormal anatomy (kyphoscoliosis) and both legs polio presented with Acute MI and Cardiogenic shock. PCI is the only option here. Provisional stenting is best in case of acute MI instead of 2 stent strategy. Imaging not possible here as patient is crashing, have to finish procedure as quick as possible, in addition to difficult anatomy, bends, lack of guide support made hardware passage very difficult. May be such patients can be taken for check angiogram after 48 to 72 hours of stabilization and proper approximation of stent can be done under imaging. 3 months follow up patient doing well with EF of 48%.