
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-220
A Case Report of Device Embolisation: Retrieval of Atrial Septal Occluder With Endoscopic Biopsy Forceps
By Chaiyih Tan, Kaisoon Liew, Huanyean Kang, Kenneth Khoo, Nancy Virginia, Mohd Khairi Othman, Prabahkar Subramaniam, Dharmaraj Karthikesan, Saravanan Krishinan, Abdul Rahim Wong, Kantha Rao Narasamuloo
Presenter
Chaiyih Tan
Authors
Chaiyih Tan1, Kaisoon Liew1, Huanyean Kang1, Kenneth Khoo1, Nancy Virginia1, Mohd Khairi Othman1, Prabahkar Subramaniam1, Dharmaraj Karthikesan1, Saravanan Krishinan1, Abdul Rahim Wong2, Kantha Rao Narasamuloo1
Affiliation
Hospital Sultanah Bahiyah, Malaysia1, Lincoln University College, Malaysia2,
View Study Report
TCTAP C-220
Structural - Other Structural Interventions
A Case Report of Device Embolisation: Retrieval of Atrial Septal Occluder With Endoscopic Biopsy Forceps
Chaiyih Tan1, Kaisoon Liew1, Huanyean Kang1, Kenneth Khoo1, Nancy Virginia1, Mohd Khairi Othman1, Prabahkar Subramaniam1, Dharmaraj Karthikesan1, Saravanan Krishinan1, Abdul Rahim Wong2, Kantha Rao Narasamuloo1
Hospital Sultanah Bahiyah, Malaysia1, Lincoln University College, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
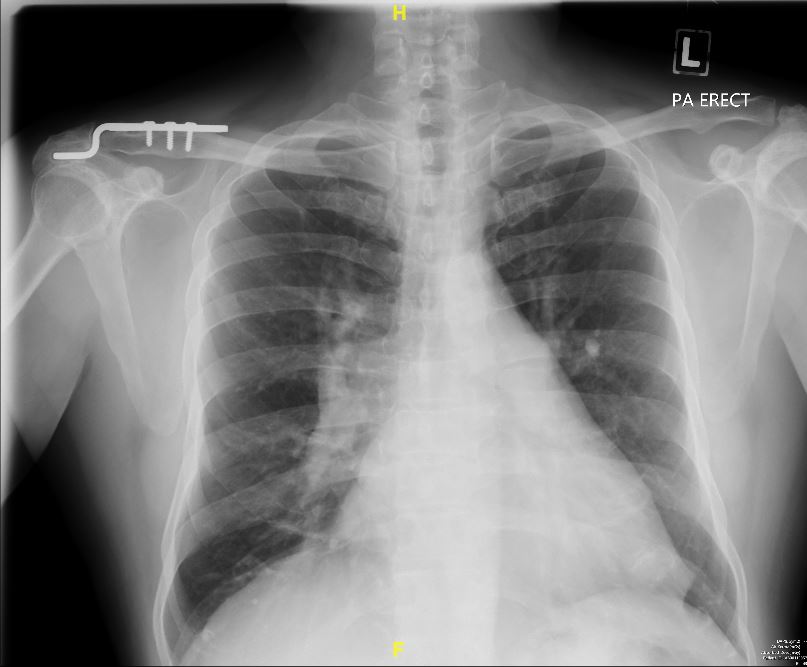
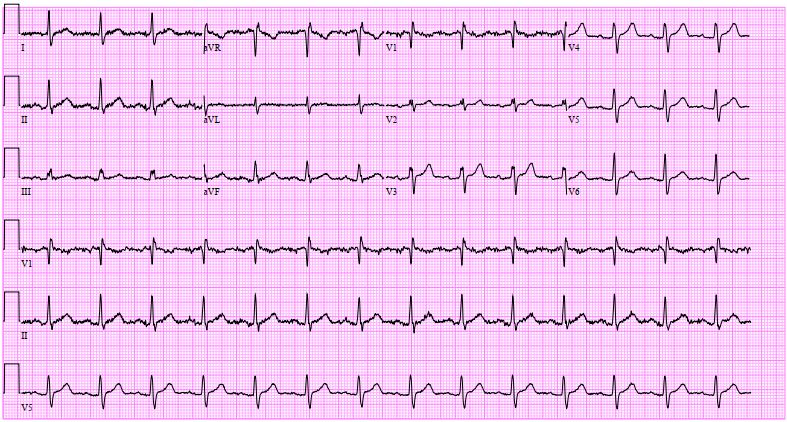
A 57-year-old asymptomatic man underwent a routine chest X-ray revealing perihilar haziness, indicative of pulmonary artery enlargement. A cardiology evaluation revealed a split second heart sound with a loud P2 & a right-sided, pansystolic murmur over the tricuspid area suggest a possible atrial septal defect (ASD) with tricuspid regurgitation. Changes of right heart dilatation like right axis deviation, P-pulmonale & right ventricle hypertrophy are absence in electrocardiography.
Relevant Test Results Prior to Catheterization
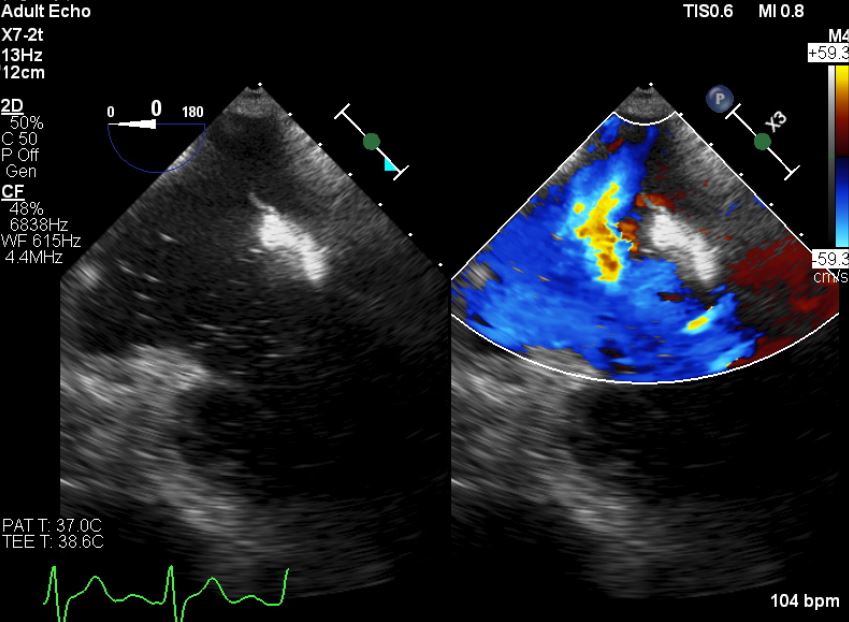
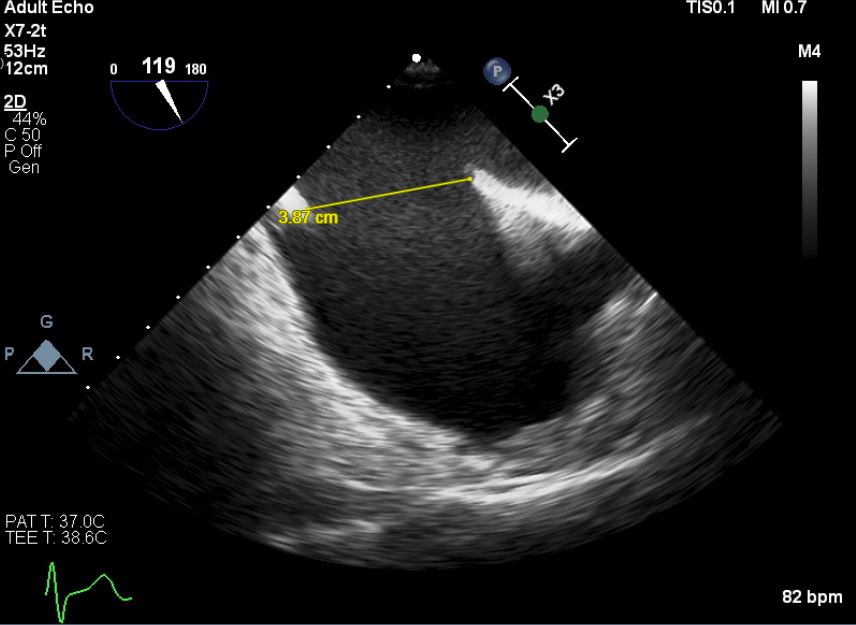
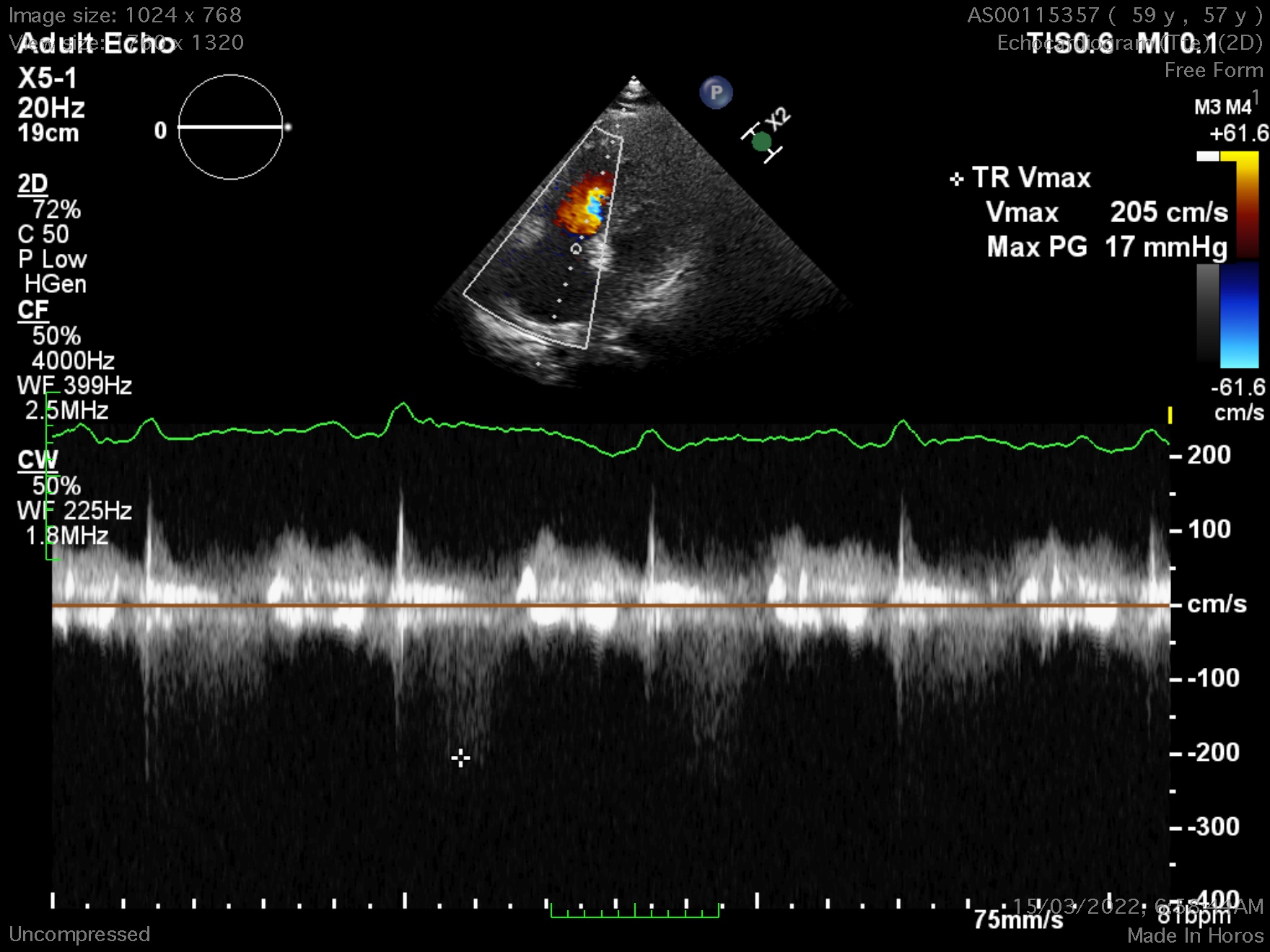
First, a trans-thoracic echocardiography(TTE) was done, there is a defect over the intra-atrial septum (IAS) with a dilated right heart. The doppler study exhibited a left to right shunting. A trans-oesophageal echocardiography (TOE) was done to assess the IAS & he has a secundum atrial septal defect(ASD), with anterior wall deficits but preserved inferoposterior wall length, largest diameter measuring 38.7mm. Estimated pulmonary arterial systolic pressure was 17 + 3 mmHG.
Relevant Catheterization Findings
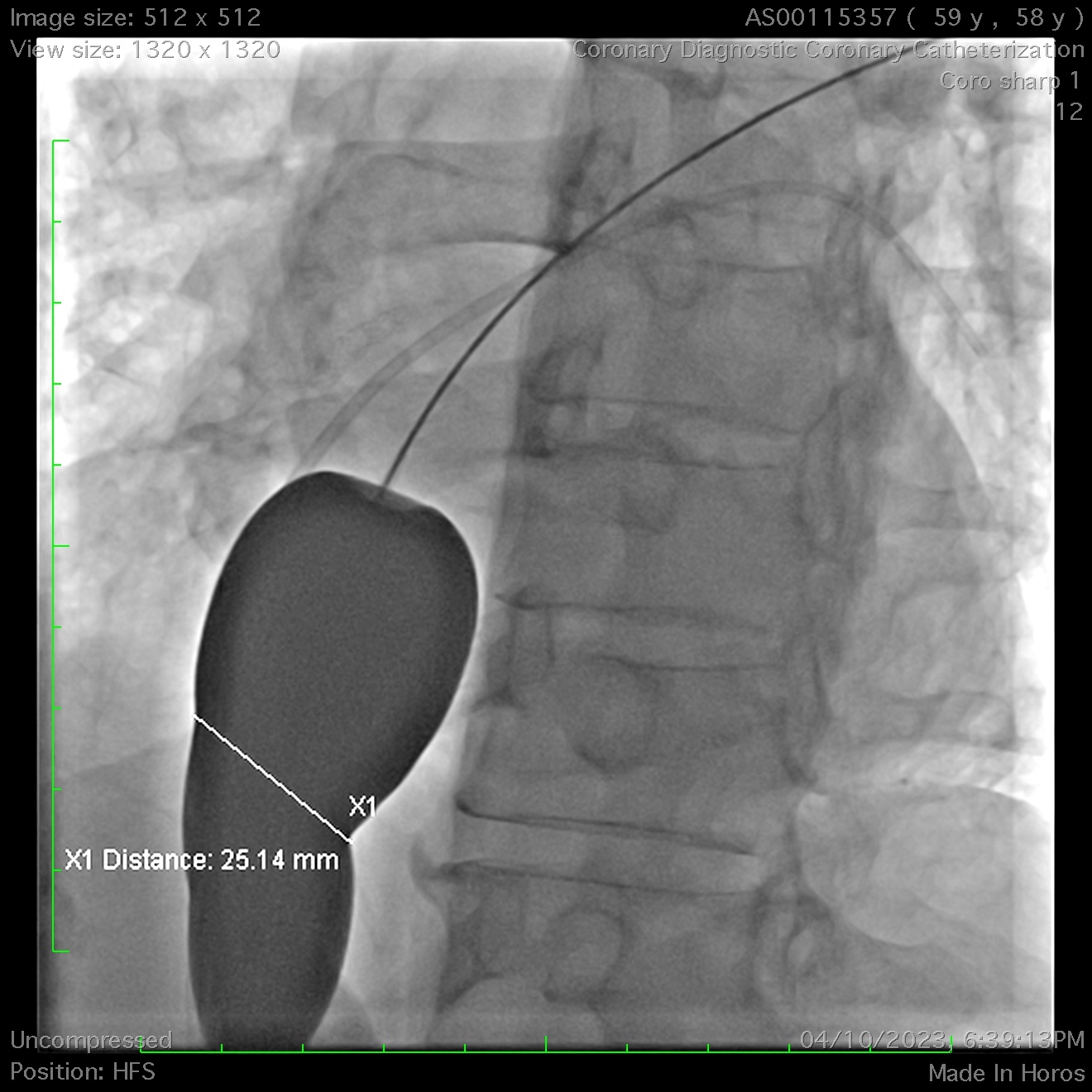
A right heart catheterisation was done, With Fick’s method revealing the pulmonary vascular resistance 2.83 wood unit indicating the need for ASD’s closure. A significant discrepancy arose in determining the true diameter of the ASD. In contrary to previous echocardiography, a repeated peri-procedural TTE measured it at 32mm with balloon inflation to occlude the defect. A decision was made to use a size 36mm occluder.
Interventional Management
Procedural Step
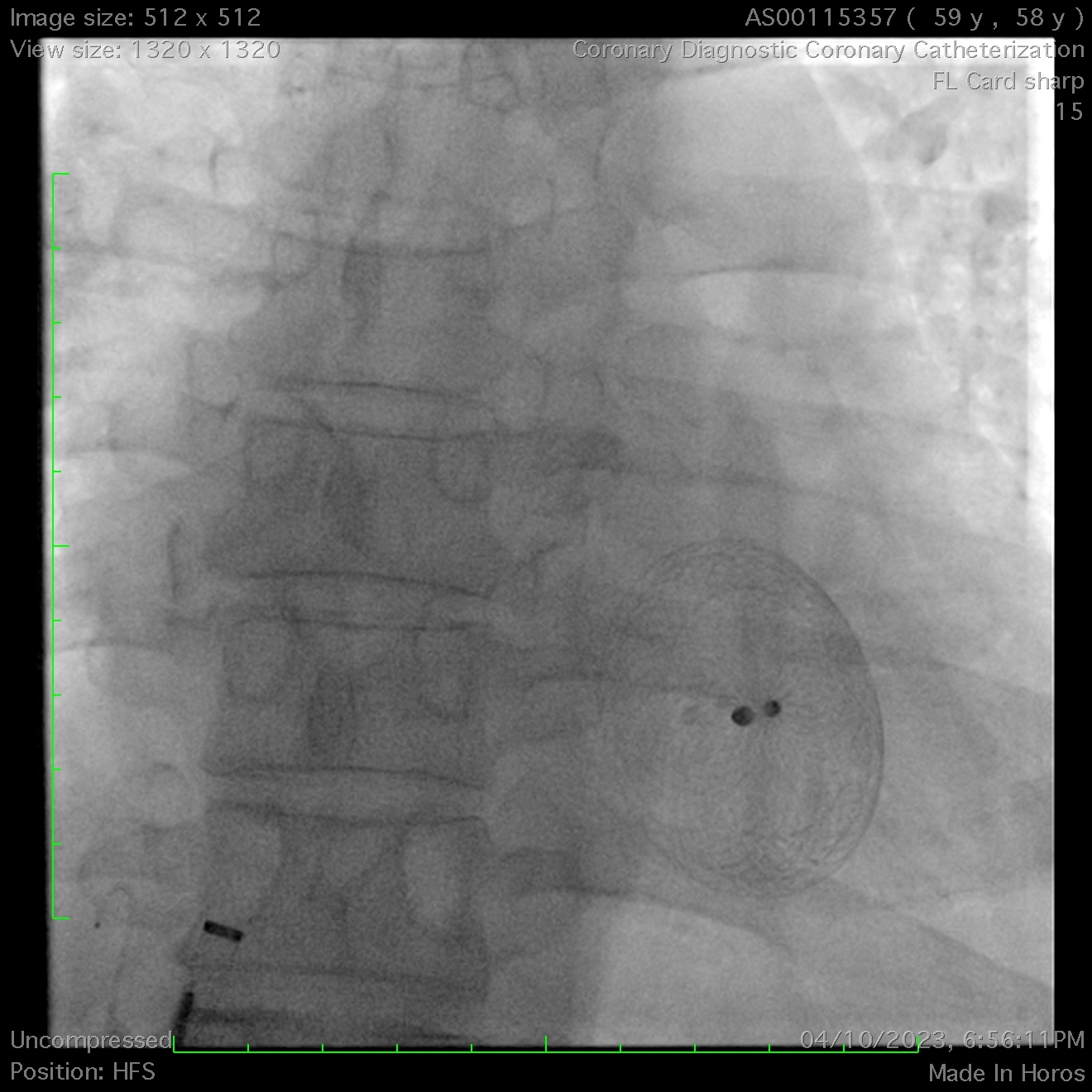
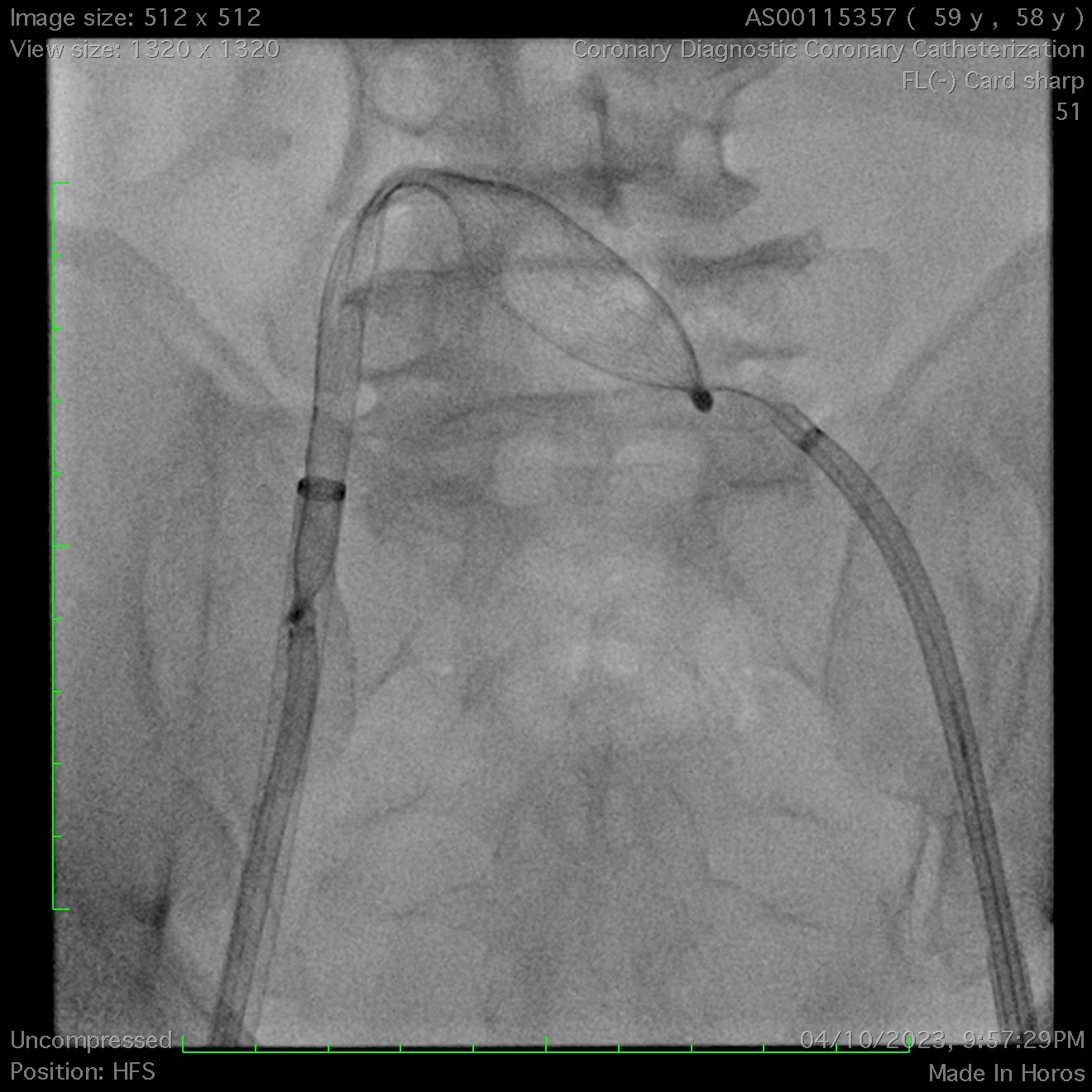
A 36mm ASD occluder was successfully deployed after confirming optimal position & stability. Unfortunately, post-release, the device embolized into the right ventricle. Agilis steerable catheters were inserted to bilateral femoral veins. Initial attempts to snare the occluder's hub with a single-loop snare proved challenging due to its high mobility within the right ventricle, even when stabilized with a steerable mapping catheter. A modified snare with a larger loop, made from a guiding catheter, coronary wire, and balloon, was employed but failed to capture the hub after multiple attempts.
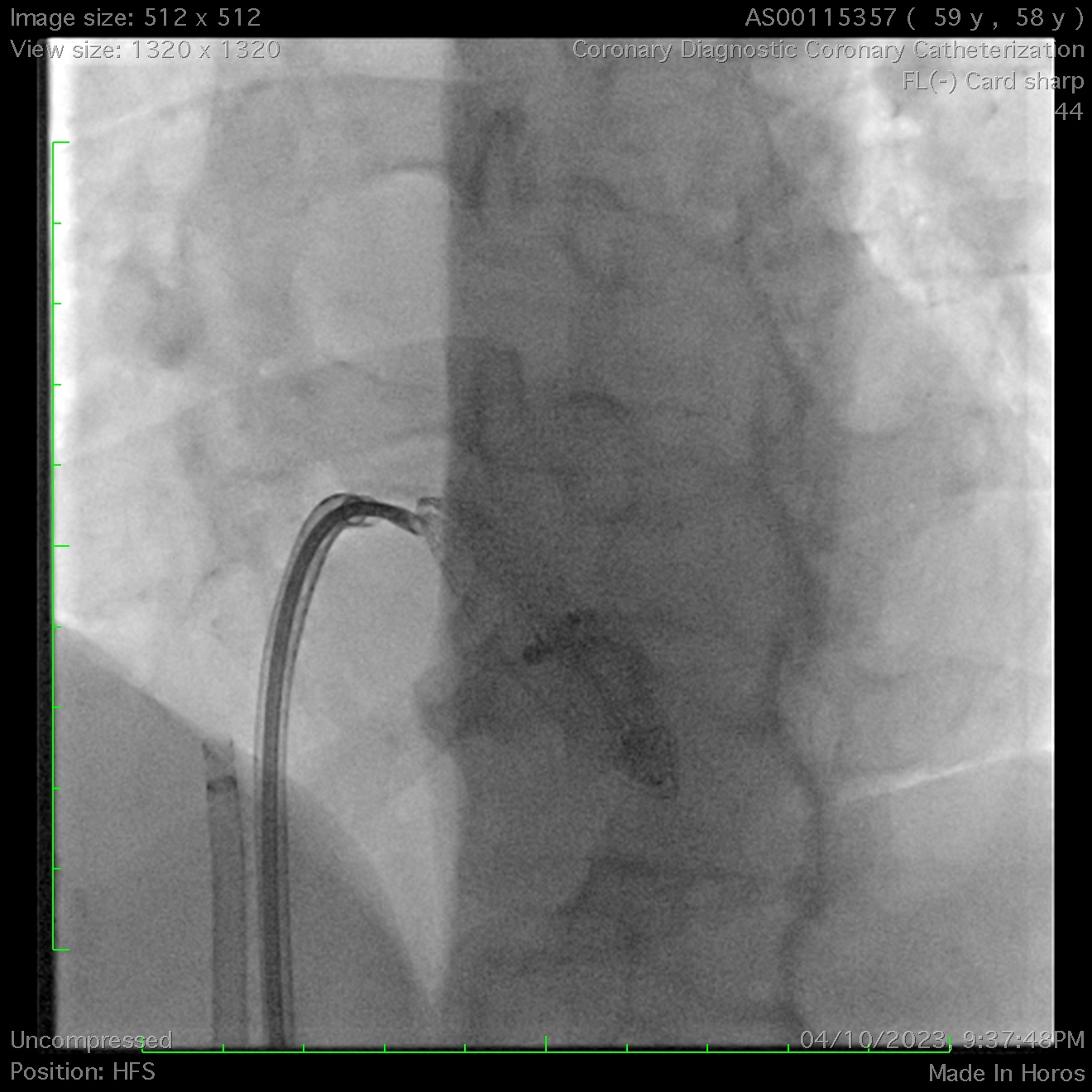
Ultimately, a biopsy forceps was used to grasp the atrial disc and pull it into the inferior vena cava. This stabilized the occluder, enabling successful snaring of the left atrial disc’s hub into the left femoral sheath. Subsequently, a second snare was deployed from the right femoral sheath to capture the right atrial disc’s hub, allowing its sheathing & subsequent removal.
A 42mm occluder was subsequently re-implanted using a balloon-assisted technique. Due to the prolonged procedure, the patient developed hemorrhagic pericarditis on the second postoperative day and required temporary pericardial drainage. The patient was discharged home three days post-procedure. Serial TTE performed on days 1, 1 month, and 6 months confirmed the occluder's in-situ position and the absence of peri-device leaks.
Ultimately, a biopsy forceps was used to grasp the atrial disc and pull it into the inferior vena cava. This stabilized the occluder, enabling successful snaring of the left atrial disc’s hub into the left femoral sheath. Subsequently, a second snare was deployed from the right femoral sheath to capture the right atrial disc’s hub, allowing its sheathing & subsequent removal.
A 42mm occluder was subsequently re-implanted using a balloon-assisted technique. Due to the prolonged procedure, the patient developed hemorrhagic pericarditis on the second postoperative day and required temporary pericardial drainage. The patient was discharged home three days post-procedure. Serial TTE performed on days 1, 1 month, and 6 months confirmed the occluder's in-situ position and the absence of peri-device leaks.
Case Summary
Precise sizing of atrial septal defect (ASD) occluders, incorporating multiple imaging modalities including TTE, TOE, fluoroscopy, cardiac magnetic resonance imaging (MRI), and computed tomography (CT), is essential to mitigate the risk of device embolisation. While standard retrieval techniques, such as snare and endomyocardial biopsy catheter methods, are well-established, endoscopic tools, including pleural and gastrointestinal biopsy forceps, offer safe and effective alternatives. Additionally, balloon-assisted techniques are highly recommended for large ASD closures to optimize device positioning and stability.