
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-231
Aneurysmal Dilatation of Common Femoral Artery After Directional Atherectomy
By Timothy Ho Him Kam, Guangming Tan, Bryan Ping Yen Yan
Presenter
Timothy Ho Him Kam
Authors
Timothy Ho Him Kam1, Guangming Tan2, Bryan Ping Yen Yan2
Affiliation
Prince of Wales Hospital, Hong Kong, China1, The Chinese University of Hong Kong, Hong Kong, China2,
View Study Report
TCTAP C-231
Endovascular - Iliac / SFA Intervention
Aneurysmal Dilatation of Common Femoral Artery After Directional Atherectomy
Timothy Ho Him Kam1, Guangming Tan2, Bryan Ping Yen Yan2
Prince of Wales Hospital, Hong Kong, China1, The Chinese University of Hong Kong, Hong Kong, China2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 70 year-old gentleman presented with 2-month history of claudication on a background of obesity, diabetes mellitus, ischemic heart disease and history of lobectomy for lung cancer. He complained of left claudication upon walking for 200 metres (Rutherford class III) despite guideline directed medical therapy. Upon examination, his left pedal pulses were absent and right pedal pulses were present. There were no ulcers or tissue losses.
Relevant Test Results Prior to Catheterization
Ankle brachial index was 0.91 and 0.73 on the right and left side respectively. The segmental pressure drop on the left side was across the knee. CT angiogram showed severely calcified vessels with multiple moderate to severe short segment stenosis involving bilateral external iliac, superficial femoral and popliteal arteries.
Relevant Catheterization Findings
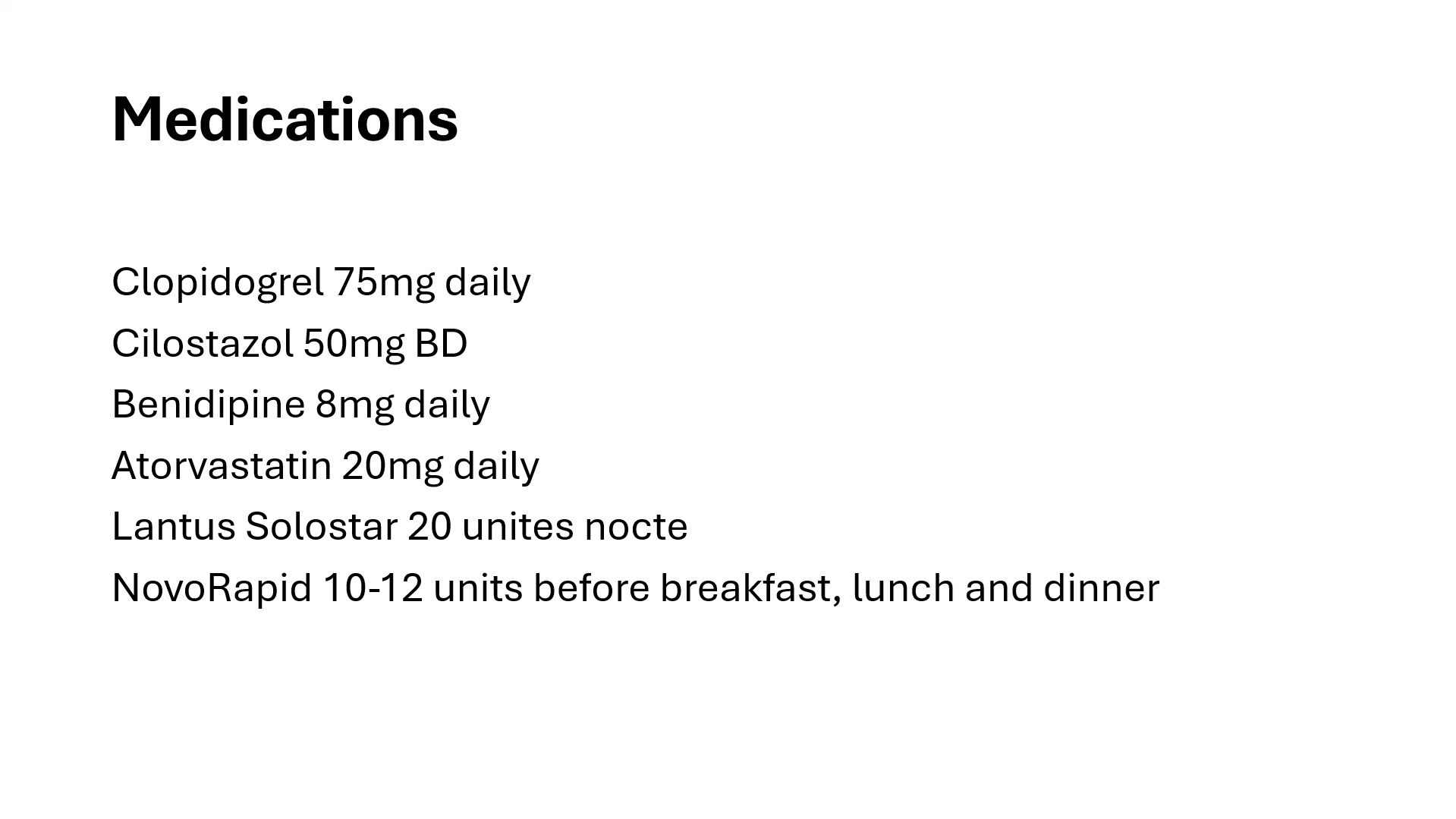
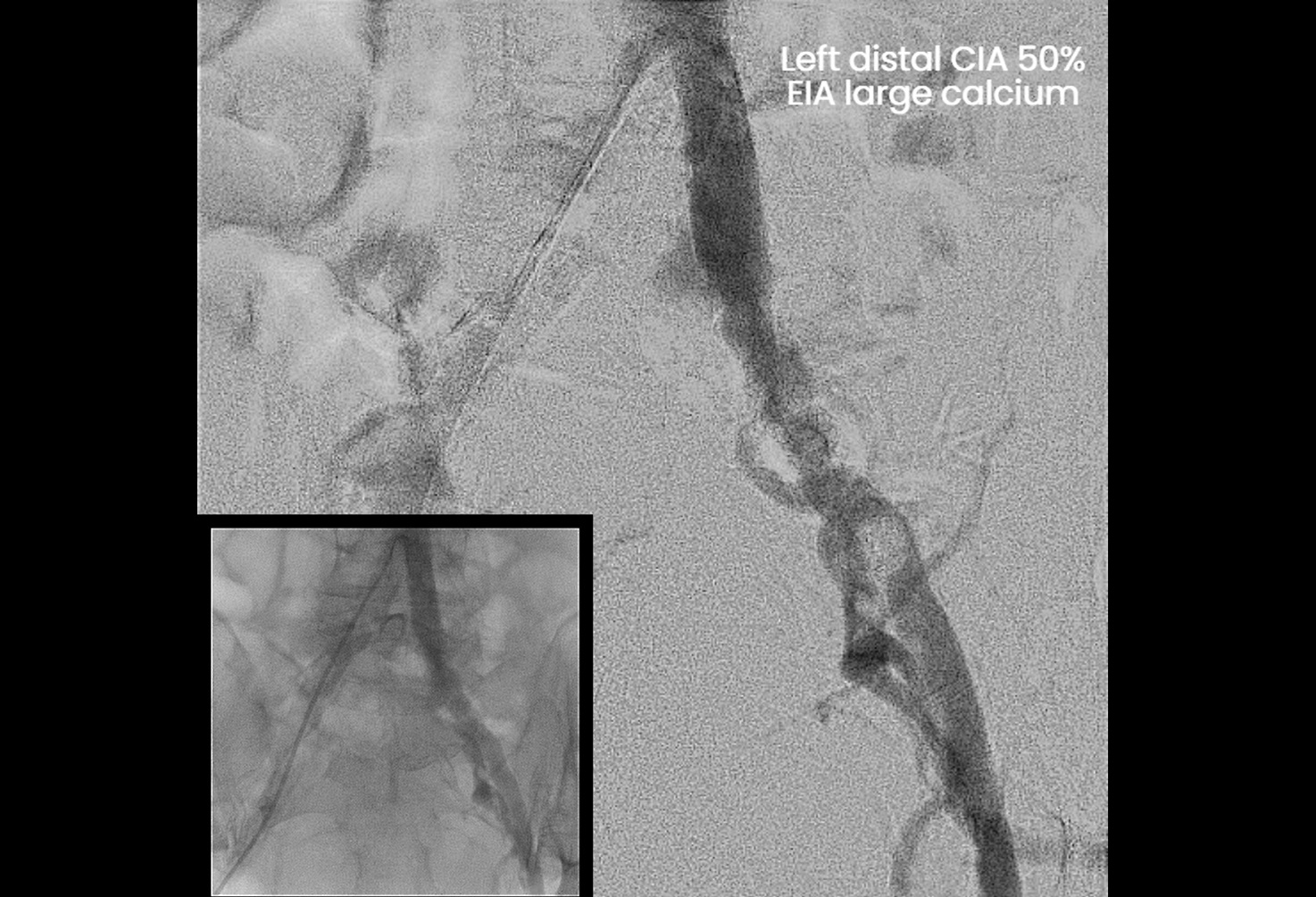
7Fr retrograde right femoral artery access was obtained and diagnostic angiograms showed left distal common iliac artery (CIA) 50% stenosis, external iliac artery (EIA) eccentric calcium 80% stenosis, common femoral artery (CFA) eccentric calcium 90% stenosis and distal superficial femoral artery (SFA) 90% stenosis.

Interventional Management
Procedural Step
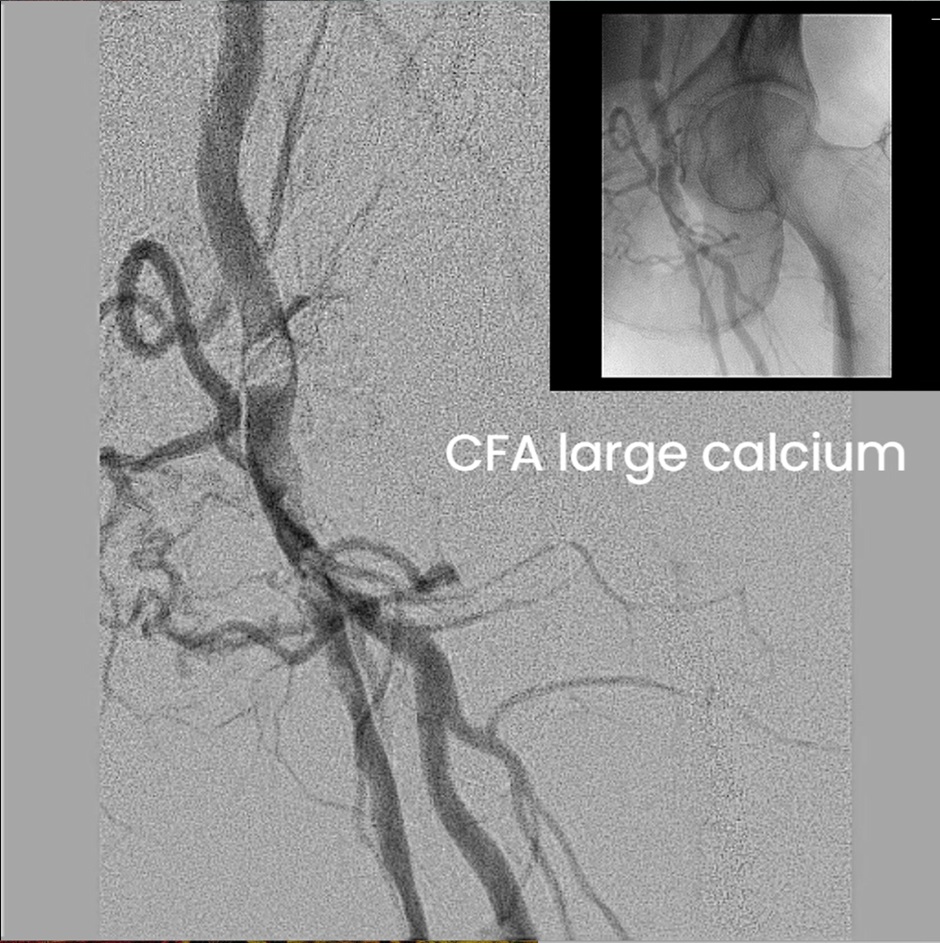
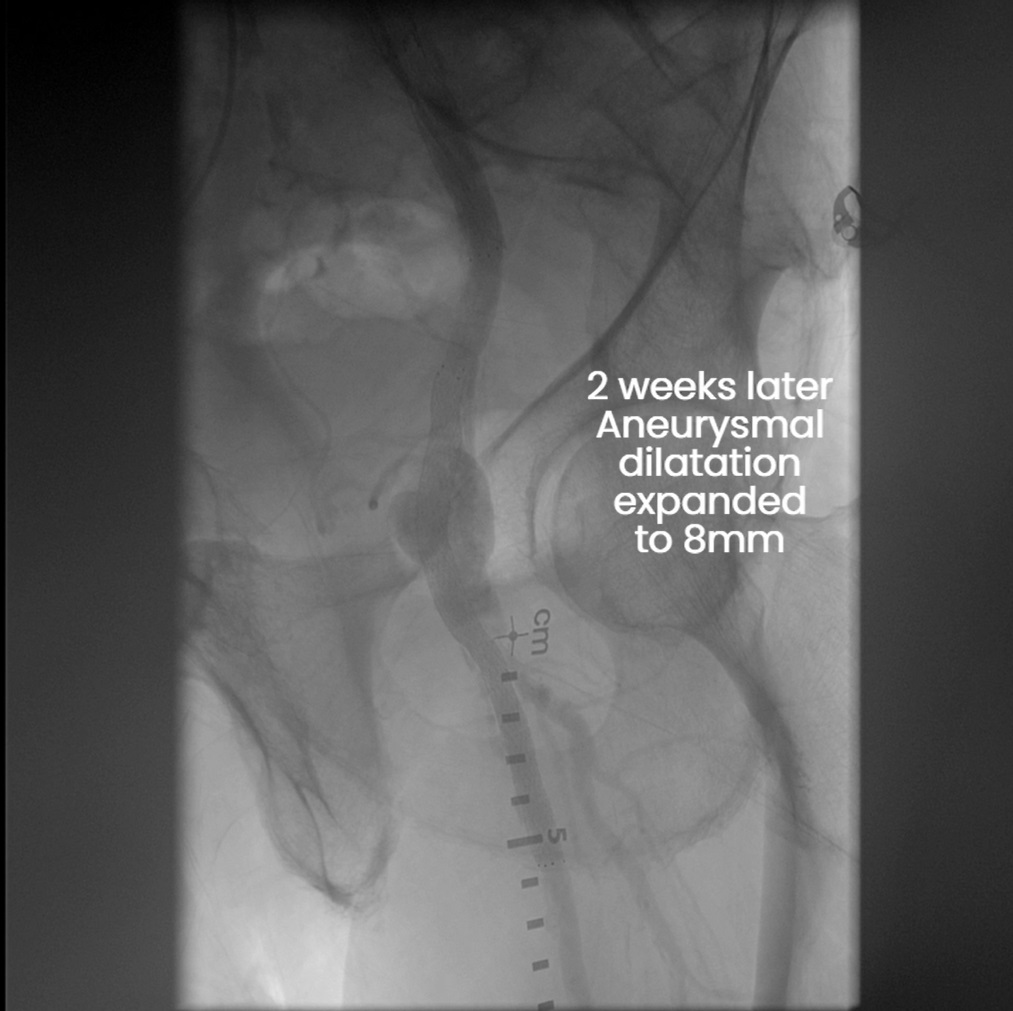
7Fr Destination guiding sheath (Terumo) was inserted and the left EIA lesion was treated first to allow passage of the sheath. Left EIA was predilated with 8.0 non-compliant (NC) balloon followed by Protégé self expanding stent (Medtronic) 10 x 40 mm and 9 x 80mm from CIA to EIA. The SFA lesion was predilated with 2.0 then 3.0 NC balloon to facilitate passage of devices, followed by the placement of SpiderFX filter (Medtronic) at the distal SFA. Then, HawkOne directional atherectomy (Medtronic) delivered multiple runs to CFA to remove plaques. The filter was then removed with no emboli found. The atherectomy site showed aneurysmal dilatational changes due to arterial wall injury, and it was decided to stent the CFA with a bare metal stent to reinforce its vessel wall. The aneurysmal site was predilated with 6.0 NC balloon, followed by a Everflex (Medtronic) 7 x 120mm stent. The SFA was treated with two 6.0x 150mm drug coated balloon with a good final angiogram result. 2 weeks after the patient complained of persistent groin pain and swelling and a bedside ultrasound showed left CFA aneurysm continued to grow. A repeated angiogram confirmed the left CFA aneurysm expanded to 8mm and the aneurysm was sealed off with the deployment of two Covera stent grafts (BD) 8 x40mm at the CFA. A repeated ultrasound 4 days after the procedure showed patent CFA with a thrombosed aneurysm. The patient underwent uneventful recovery with improvements in claudication and groin swelling

Case Summary
This case illustrates a complication of CFA aneurysmal dilatation most likely due to the unintentional atherectomy of tunica intima which weakened the vessel wall. Directional atherectomy was chosen to tackle the calcified CFA due to the eccentricity of the calcium. The decision to treat with the aneurysm with a bare metal stent rather than a cover stent upfront was because of side branches preservation. In the end, the symptomatic aneurysm expanded in size and was treated with cover stents. After the deployment of the first cover stent, residual leakage via the proximal stent entry was recognised and was treated with another cover stent, resulting in complete sealing of the aneurysmal sac.