
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-086
Brace the Storm
By Ting Yuen Beh, Chan Ho Thum, Wei Liang Lee, Ji Ken Ow, Azhari Rosman
Presenter
Ting Yuen Beh
Authors
Ting Yuen Beh1, Chan Ho Thum1, Wei Liang Lee1, Ji Ken Ow1, Azhari Rosman1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-086
Coronary - Complex PCI - CTO
Brace the Storm
Ting Yuen Beh1, Chan Ho Thum1, Wei Liang Lee1, Ji Ken Ow1, Azhari Rosman1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 59 year old gentleman with hypertension, dyslipidaemia, coronary artery disease and obesity. He had history of PCI to LAD and RCA in 2004 and 2010. He presented with recurrent unstable angina. Therefore, coronary angiogram was performed.

Relevant Test Results Prior to Catheterization
ECG: T inversion anterior leads
Troponin T: normal
Troponin T: normal
Relevant Catheterization Findings
Left Main Stem : Normal
Interventional Management
Procedural Step
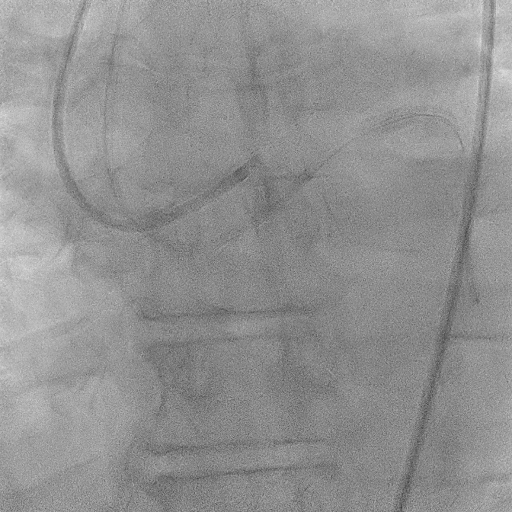
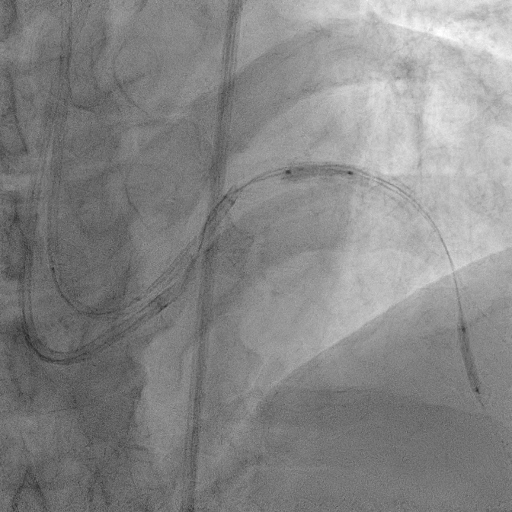
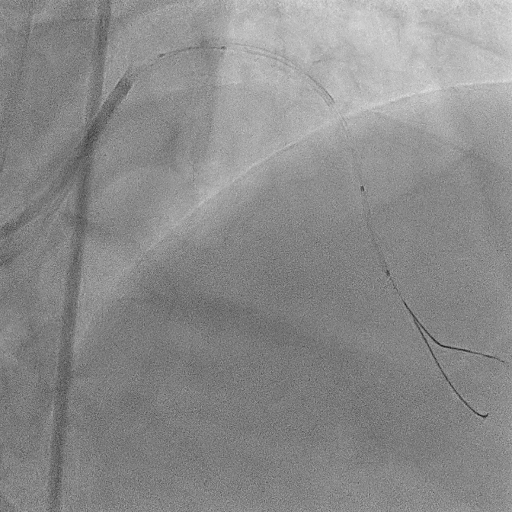
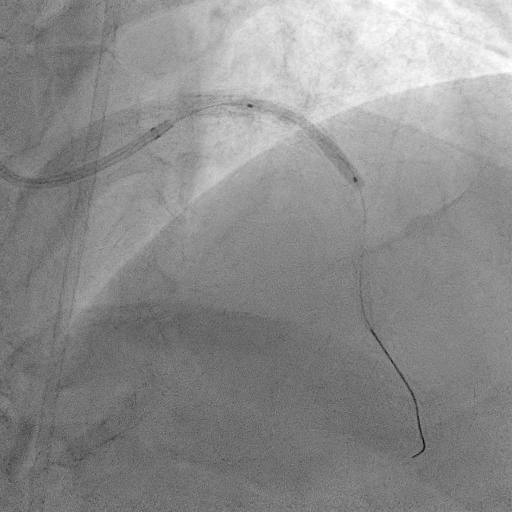
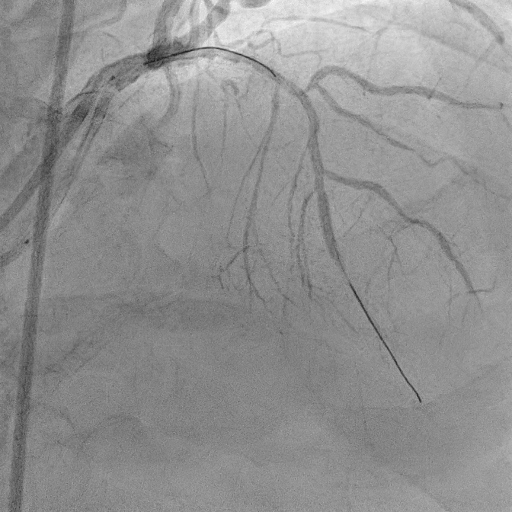
The procedure commenced with EBU 3.5/6F catheter and CTO wire with microcatheter. Managed to cross the lesion and changed to workhorse wire. Proximal LAD ISR predilated with SC balloon 2.0/15mm. CTO at mid segment predilated with same balloon. However, noted perforation at mid LAD after predilatation. We used the same balloon to tamponade the perforation and attempted to wire down distal LAD with another wire but failed. Right femoral puncture was performed and another EBU3.5/6F was used. The ping pong technique was used in which another workhorse wire to distal LAD when tamponade balloon was deflated. However, the covered stent was unable to cross the proximal LAD. Proximal segment was then predilated with NC 2.5/15mm, yet still unable to advance the covered stent. Subsequently, guide extension GuidePlus II was used and managed to advance covered stent 2.5/20mm. Tamponade balloon was then removed and covered stent deployed at perforation site. We proceeded with drug coated balloon angioplasty to proximal-mid LAD using DCB 3.5/20mm. Patient was stable and bedside echo revealed minimal pericardial effusion only
Case Summary
Coronary artery perforation is rare but potentially lethal complication. Early recognition and immediate balloon occlusion are crucial in preventing cardiac tamponade and haemodynamic compromise. Double catheter guide technique (ping pong) allowed controlled delivery of covered stents to perforation site. It ensures uninterrupted balloon occlusion of perforated site and smooth delivery of bulky covered stents.