
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-048
Critical Intervention: Left Main Bifurcation Stenting in a Patient With Anterior Myocardial Infarction
By Wai For Siu, Ho Ling Tsoi
Presenter
Wai For Siu
Authors
Wai For Siu1, Ho Ling Tsoi1
Affiliation
North District Hospital, Hong Kong, China1,
View Study Report
TCTAP C-048
Coronary - Complex PCI - Bifurcation
Critical Intervention: Left Main Bifurcation Stenting in a Patient With Anterior Myocardial Infarction
Wai For Siu1, Ho Ling Tsoi1
North District Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Mr. Yip, a 60-year-old smoker, with a history of hyperlipidemia and cerebrovascular accident defaulted follow-up, presented to the AED department on 29th September 2024 for central chest pain 1 week ago. Vital signs were stable, with blood pressure 156/100mmHg, pulse 81 beats per minute, O2 saturation of 97% on room air. Physical examination showed clear chest, dual heart sound without murmur and no ankle edema.
Relevant Test Results Prior to Catheterization
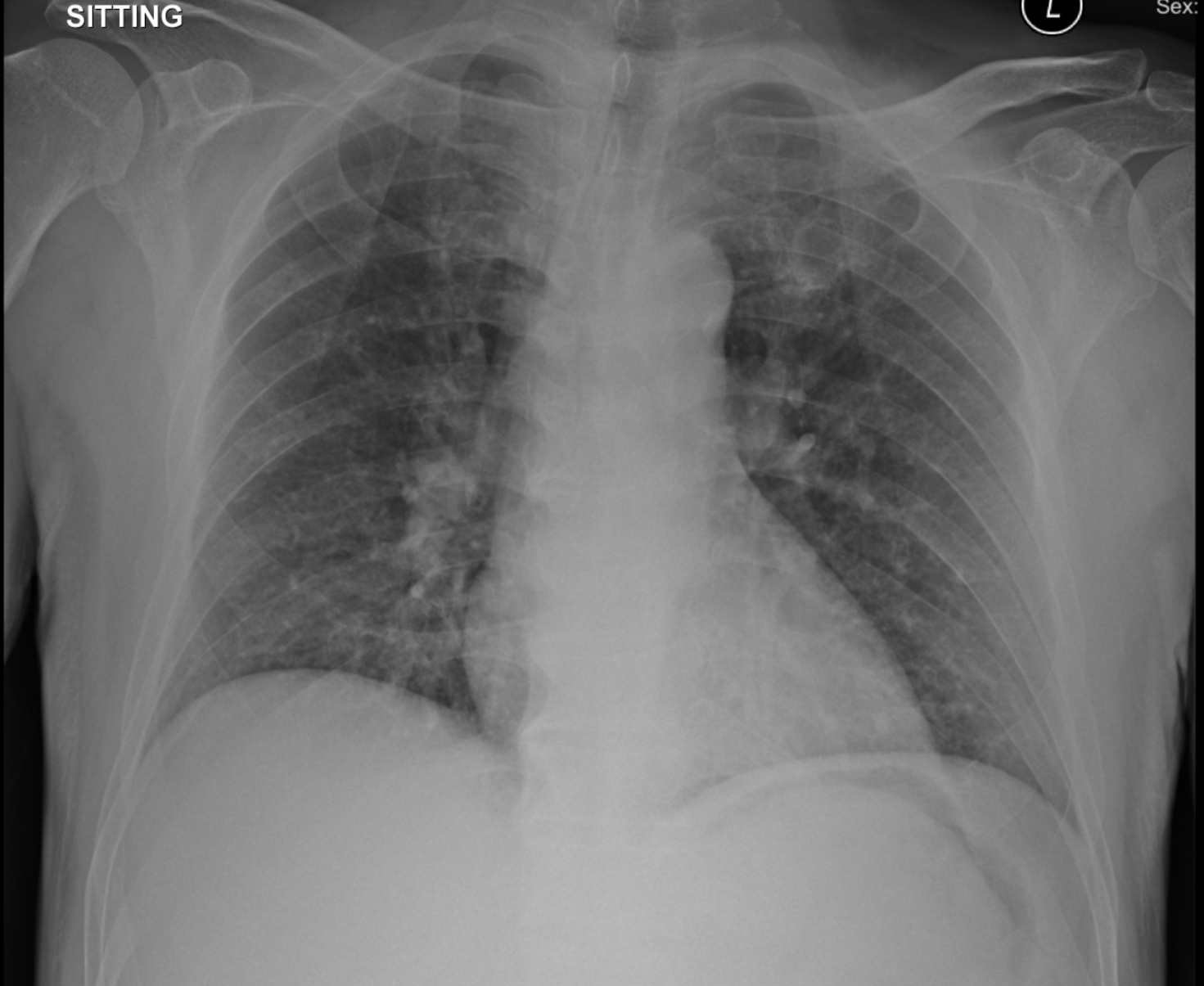
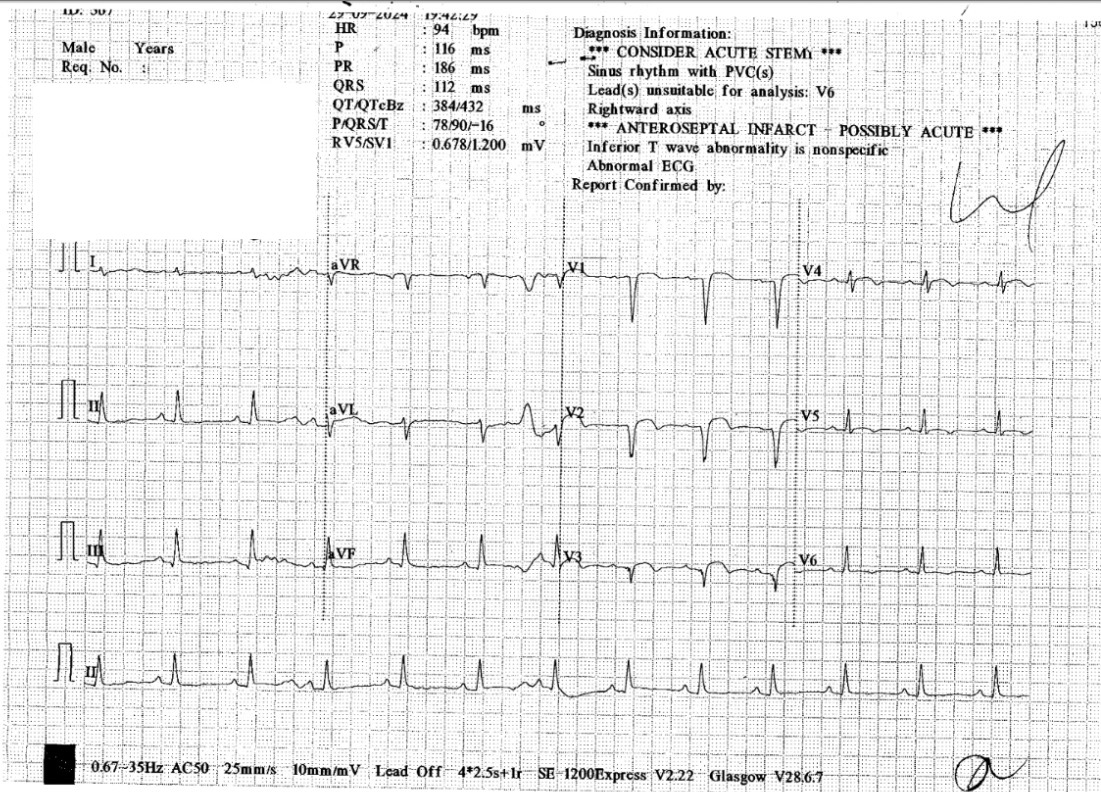
ECG showed sinus rhythm with Q wave and ST-segment elevation over lead V1-V3. Chest X-ray showed no consolidation. Highly sensitive troponin I was elevated to 5120ng/L and creatine kinase was elevated to 331U/L. LDL was 3.8mmol/L. HbA1c was 13.9%. Bedside echocardiography showed LVEF 40% with hypokinesia over LAD territory, without significant valvular lesions.
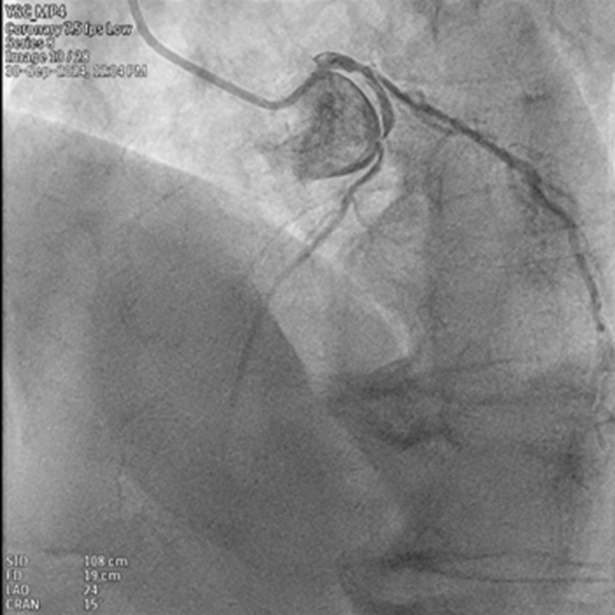
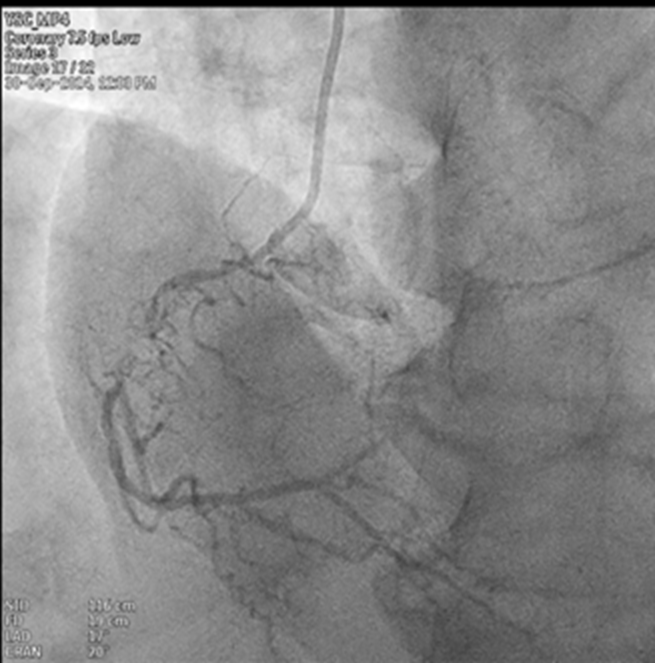
Relevant Catheterization Findings
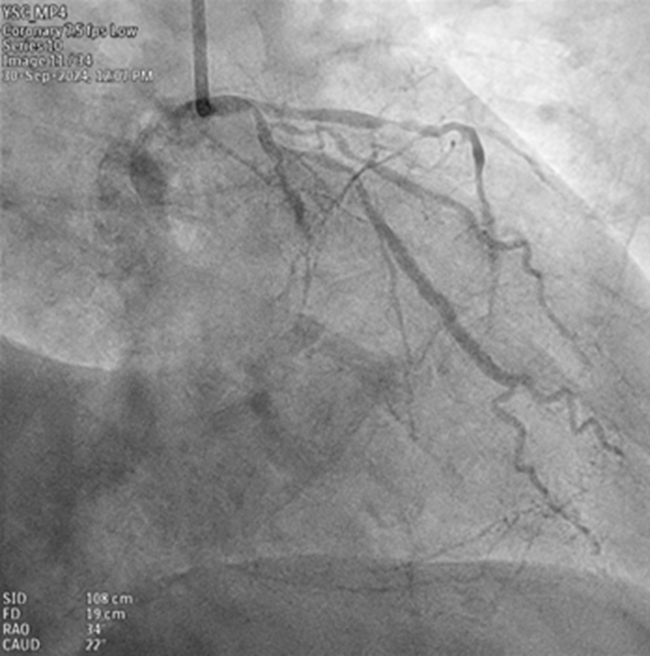
Coronary angiogram was done using 6Fr TIGII catheter. It revealed a chronic total occlusion of the proximal-to-mid RCA. The left system revealed a left main bifurcation lesion, with a Medina type 1,1,1. There was a 60% stenosis over distal LM. LAD was diffusely diseased, with ostial-proximal LAD 80% stenosis, mid LAD 99% stenosis, followed by distal LAD 70% stenosis. LCx revealed ostial LCx 80% stenosis with a chronic total occlusion at very distal LCx. OM branch was big, with 80% stenosis.
Interventional Management
Procedural Step
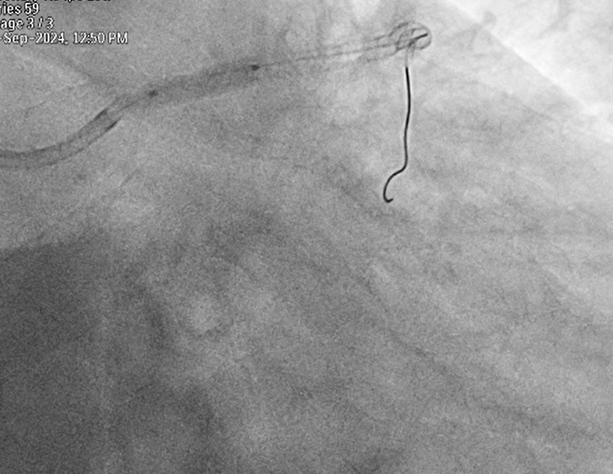
PCI was performed using 6Fr JL4 guide catheter. A guide wire was used to cross LAD lesion. OCT was performed. Proximal to distal LAD was pre-dilated with 2.0 x 15mm compliant balloon, followed by 2.25 x 15mm NC balloon. A drug-eluted stent 2.25 x 38mm was deployed to mid to distal LAD, and another drug-eluted stent 3.0 x 38mm was deployed to proximal to mid LAD. Distal LAD stent was post-dilated with 2.5 x 15mm NC balloon, and proximal to mid LAD stent was post-dilated with 3.0 x 15mm NC balloon.
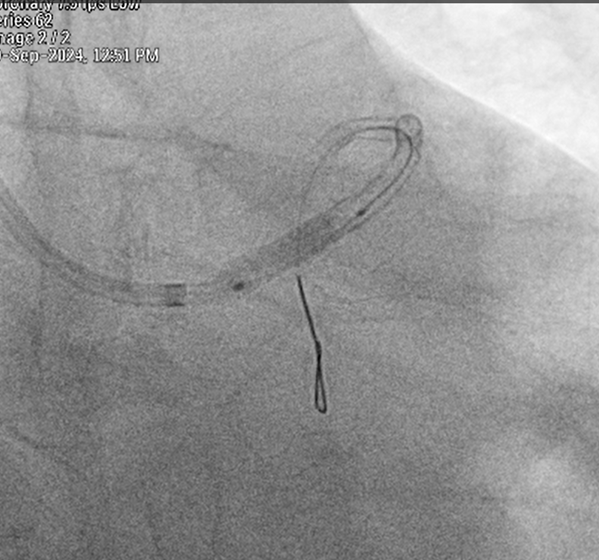
Another guidewire was used to cross OM lesion. OCT was performed. Stenting to LM-LAD/LCx was planned to be done by mini-crush technique. Ostial LCx and OM were pre-dilated with 2.25 x 20mm compliant balloon and 2.5 x 12mm NC balloon. A drug-eluted stent 2.25 x 38mm was deployed to distal left main to OM, followed by post-dilatation with 2.5 x 8mm NC balloon. A 3.5 x 12mm NC balloon was delivered to LAD and inflated to crush ostial LCx stent. Another 3.5 x 18mm drug-eluted stent was deployed to LM-pLAD. POT to LMS was performed with a 4.0 x 8mm NC balloon. OM branch was recrossed by guide wire. POBA to ostial LCx was done by a 1.5 x 15mm NC balloon. Kissing inflation to LMS/LAD and LMS/LCX was performed by 3.5 x 12mm NC balloon and 2.5 x 12mm NC balloon respectively. Good angiographic and OCT results were obtained.

Another guidewire was used to cross OM lesion. OCT was performed. Stenting to LM-LAD/LCx was planned to be done by mini-crush technique. Ostial LCx and OM were pre-dilated with 2.25 x 20mm compliant balloon and 2.5 x 12mm NC balloon. A drug-eluted stent 2.25 x 38mm was deployed to distal left main to OM, followed by post-dilatation with 2.5 x 8mm NC balloon. A 3.5 x 12mm NC balloon was delivered to LAD and inflated to crush ostial LCx stent. Another 3.5 x 18mm drug-eluted stent was deployed to LM-pLAD. POT to LMS was performed with a 4.0 x 8mm NC balloon. OM branch was recrossed by guide wire. POBA to ostial LCx was done by a 1.5 x 15mm NC balloon. Kissing inflation to LMS/LAD and LMS/LCX was performed by 3.5 x 12mm NC balloon and 2.5 x 12mm NC balloon respectively. Good angiographic and OCT results were obtained.
Case Summary
This case demonstrated successful bifurcation stenting via Mini-crush technique to LM/LAD/LCx in a patient with anterior myocardial infarction under OCT guidance. This approach minimizes stent protrusion into the left main artery, reducing the risk of complications such as in-stent restenosis at LCx ostium.