
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-013
A Rare Case Report of Acute Myocardial Infarction Originating From Superdominant Left Anterior Descending Artery Occlusion
By Leet Ming Khor, Su Min Lim, Poi Keong Kong
Presenter
Su Min Lim
Authors
Leet Ming Khor1, Su Min Lim1, Poi Keong Kong1
Affiliation
Hospital Pulau Pinang, Malaysia1,
View Study Report
TCTAP C-013
Coronary - ACS/AMI
A Rare Case Report of Acute Myocardial Infarction Originating From Superdominant Left Anterior Descending Artery Occlusion
Leet Ming Khor1, Su Min Lim1, Poi Keong Kong1
Hospital Pulau Pinang, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
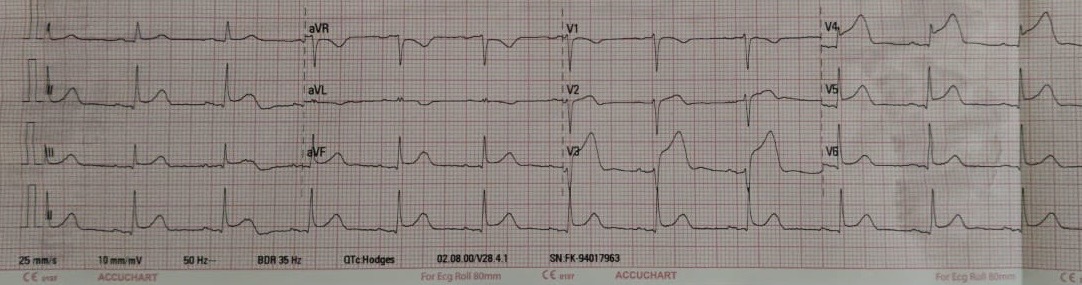
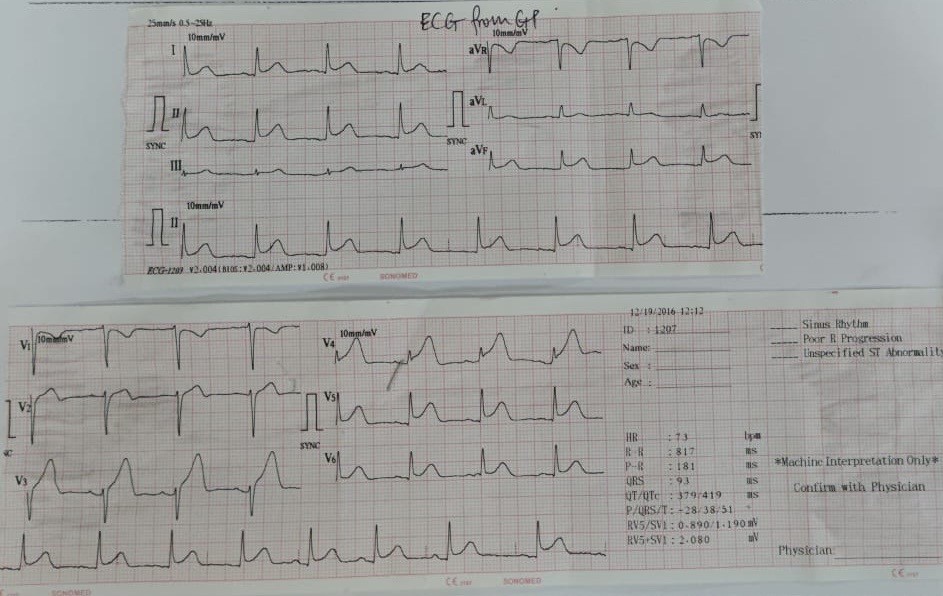
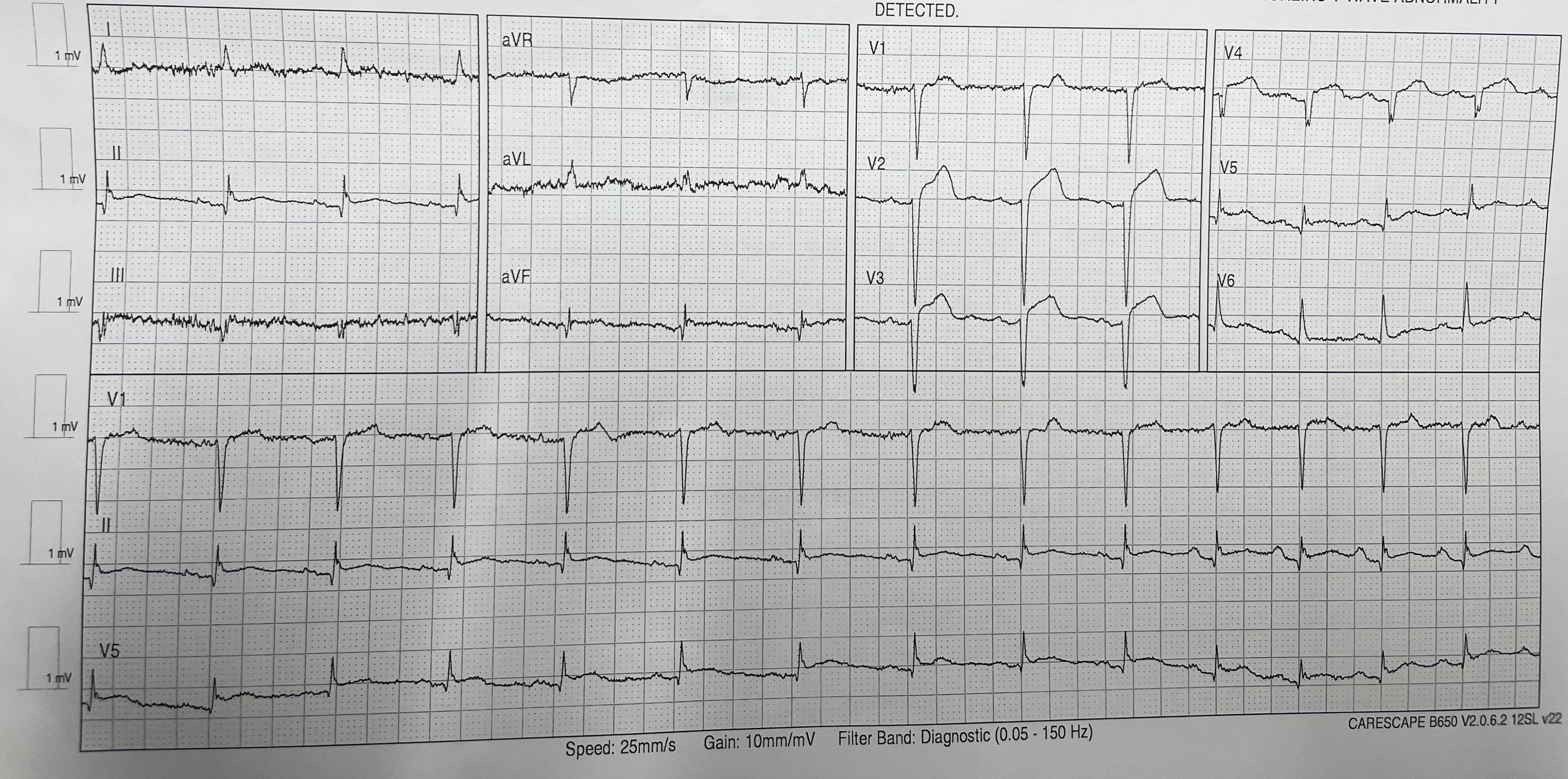
53 year old Chinese male, no known medical illness and non-smoker, presented to local clinic with sudden onset central chest pain of one hour duration with profuse sweating. Urgent ECG at the clinic showed ST elevation changes. He was immediately referred to the nearest hospital for acute myocardial infarction. He was hemodynamically stable at presentation. The repeated ECG at the hospital showed evolving MI changes and hence he was referred to our cardiac center for primary PCI.
Relevant Test Results Prior to Catheterization
ECG showed ST elevation over V3-V6, I, II, III, AVF suggestive of anteroinferolateral STEMI.Formal Echocardiogram showed reduced LVEF 38%, normal valves, no pericardial effusion and no left ventricular thrombus.Hemoglobin 17.7, random blood sugar 7.6
Relevant Catheterization Findings
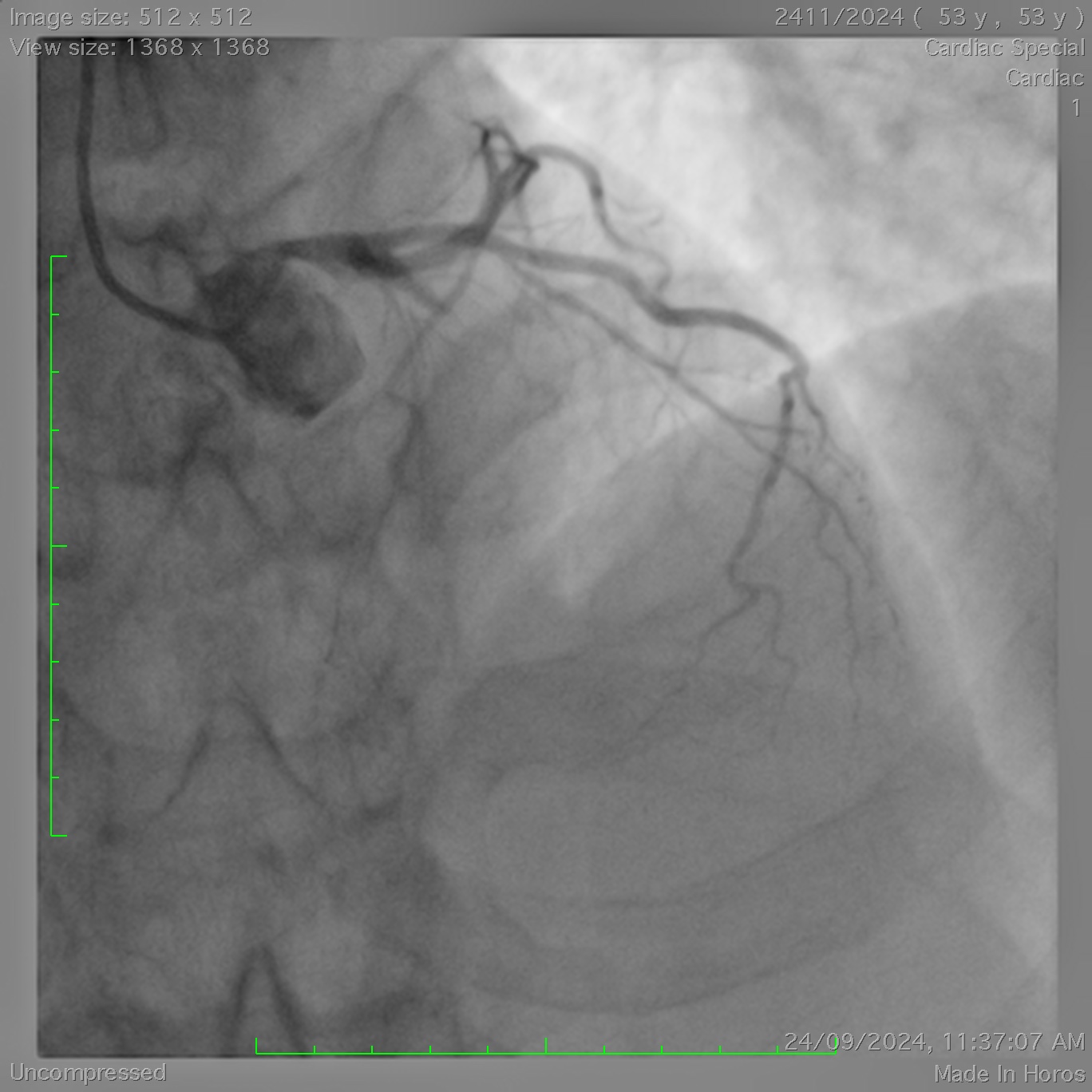
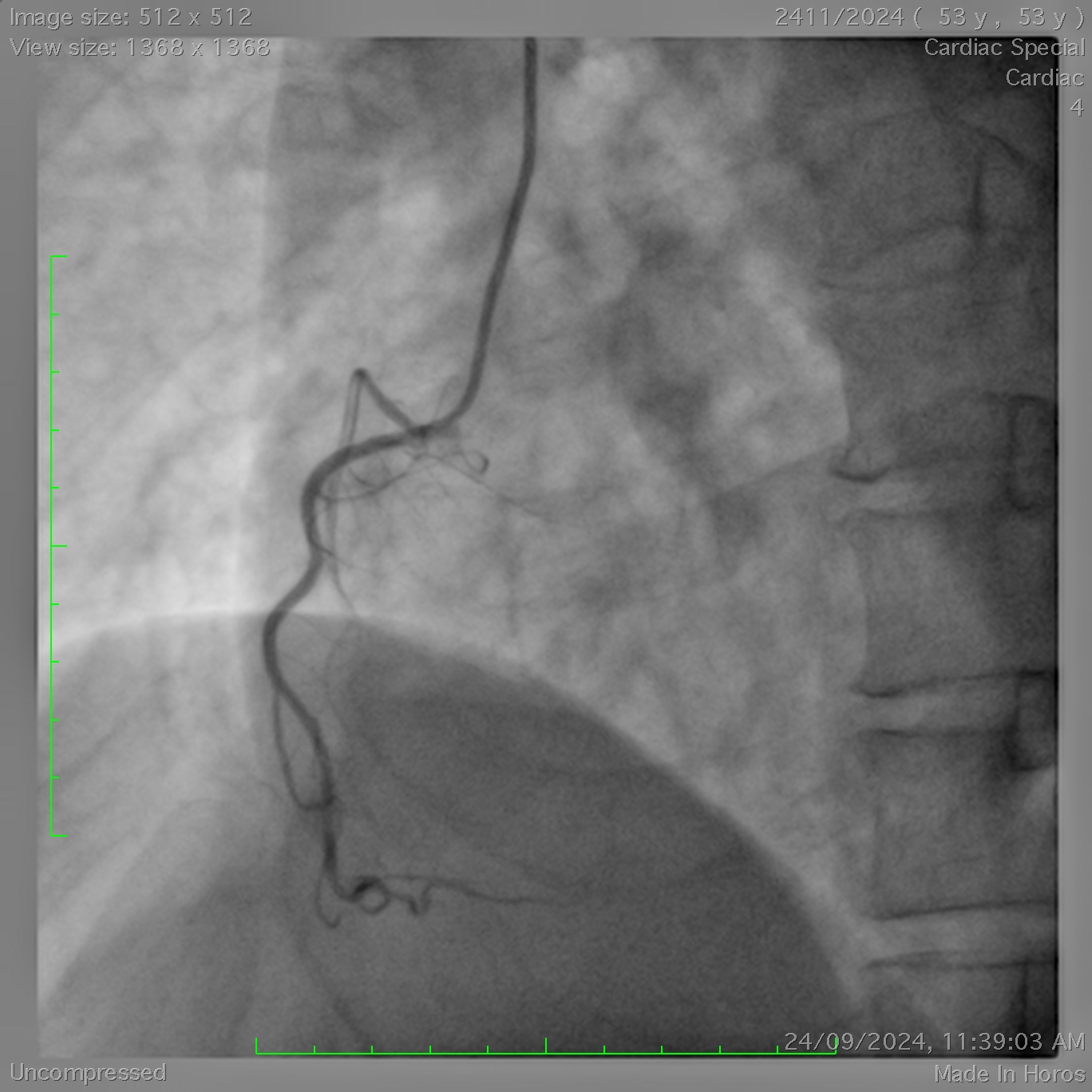
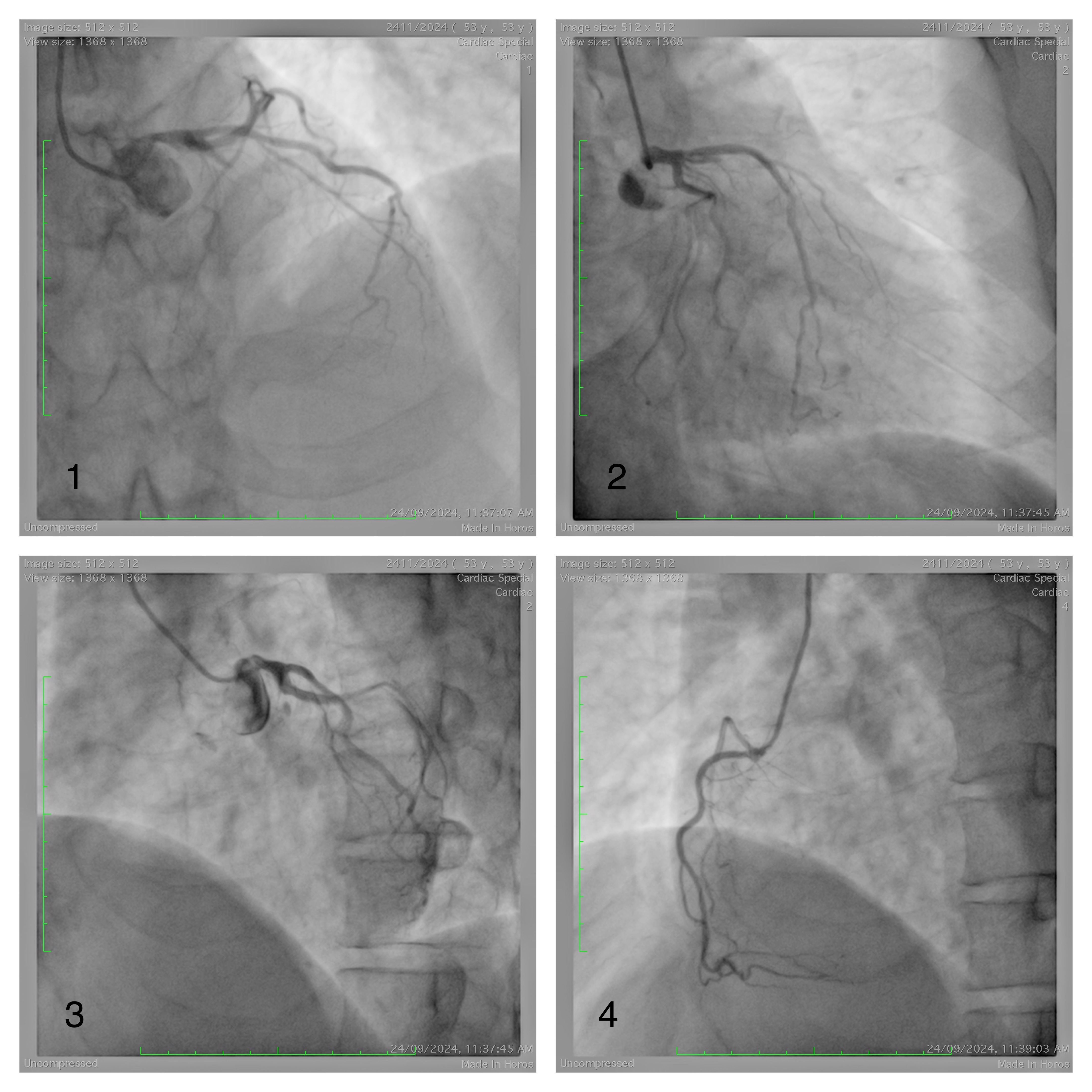
Coronary angiogram showed acute total occlusion of proximal LAD with smooth, non-dominant LCx and smooth, non-dominant RCA.Primary PCI done to LAD with DES Biofreedom Ultra 3.0X33mm. Noted post-PCI angiogram showed the PDA arising directly as continuation of distal to apical LAD meaning the wrap around LAD is supplying the posterior wall apart from the usual anterior and part of inferior territory.1,2,3 Acute total occlusion of proximal LAD with smooth non-dominant LCx4 Small, non-dominant RCA
Interventional Management
Procedural Step
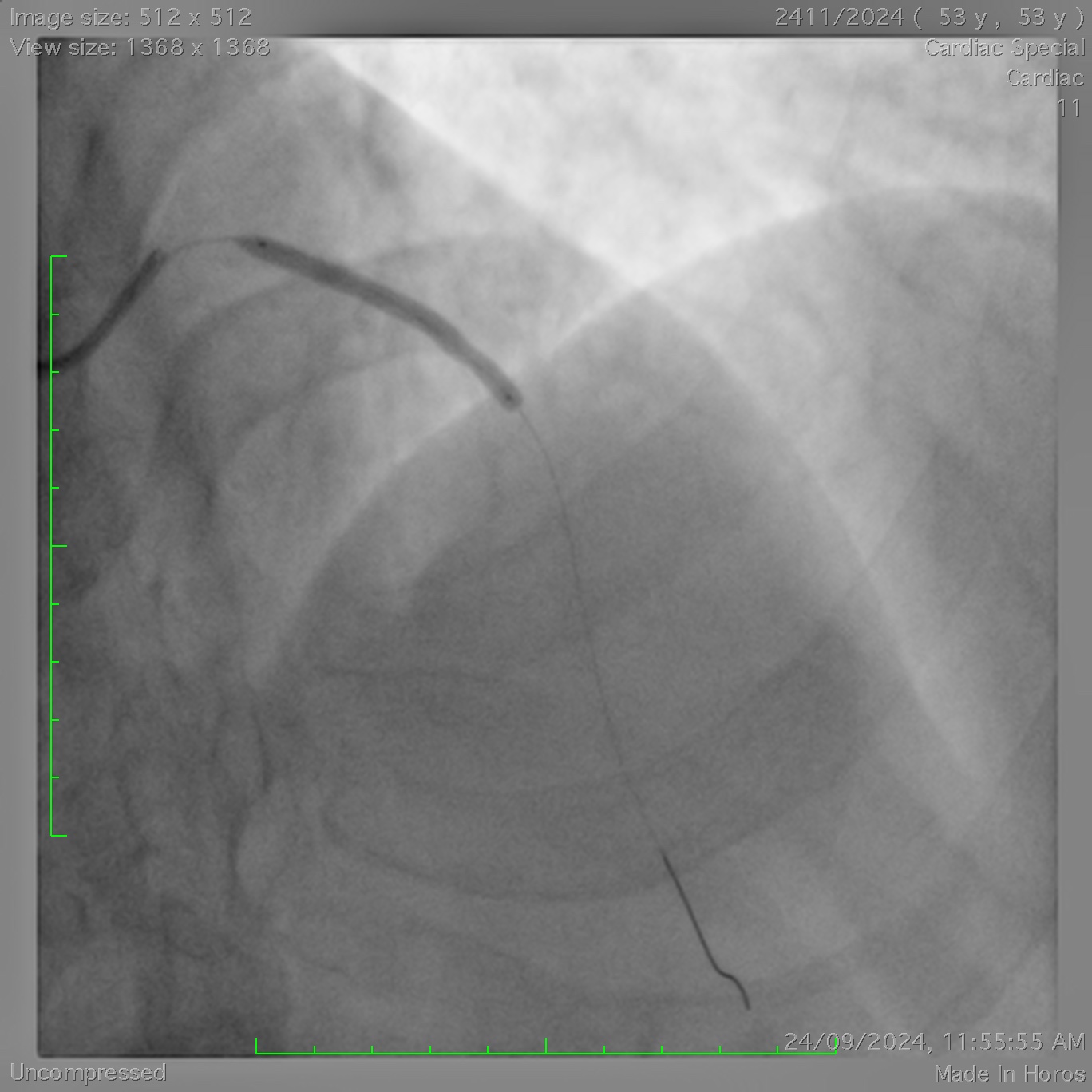
Right radial access with 6 French sheath and 6 French XBLAD3.5 guide engaged to LM-LAD followed by intracoronary heparin 6000 units. Runthrough floppy wire crossed the occluded proximal LAD segment to the distal LAD. Minimal flow seen across proximal LAD after wiring so no thromboaspiration was done but the occluded segment was predilated with semi compliant balloon 2.5X15mm at 12atm. After predilatation, TIMI 3 flow was restored to the distal LAD with very minimal thrombus. Proximal to mid LAD was stented with DES Biofreedom Ultra 3.0X33mm at nominal pressure 8atm. Postdilated LAD stent with non-compliant balloon 3.25X15mm up till 26atm (maximal expansion of more than 3.5mm). Post-angioplasty, noted large wrap around LAD with PDA coming directly as continuation from the distal LAD after wrapping around the apex supplying posterior LV wall apart from anterior, lateral and partly inferior surface. The RCA and Lcx are non-dominant. Final angioplasty result is good with TIMI 3 flow restored in the highly dominant LAD with no evidence of dissection and perforation and first diagonal branch flow still preserved.
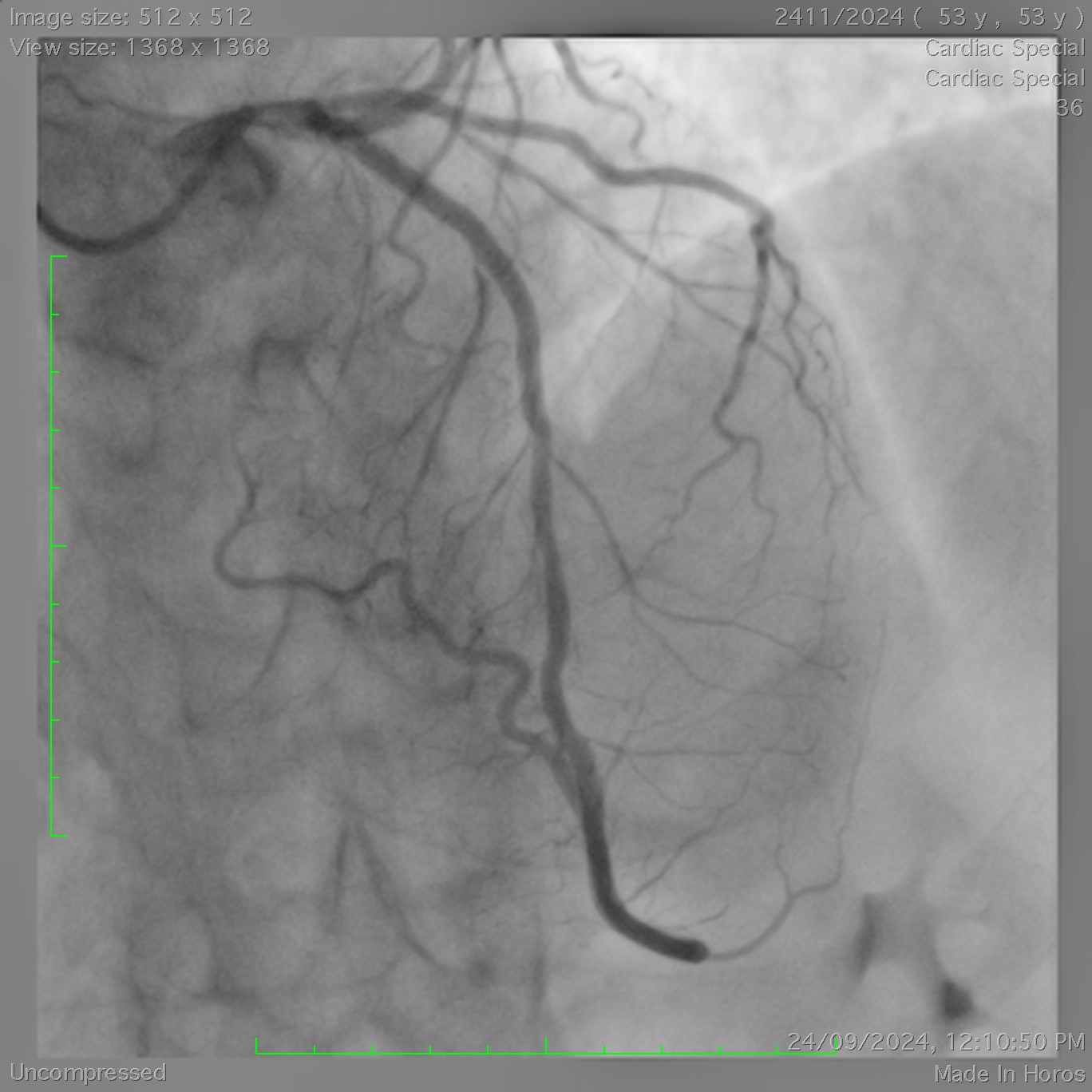
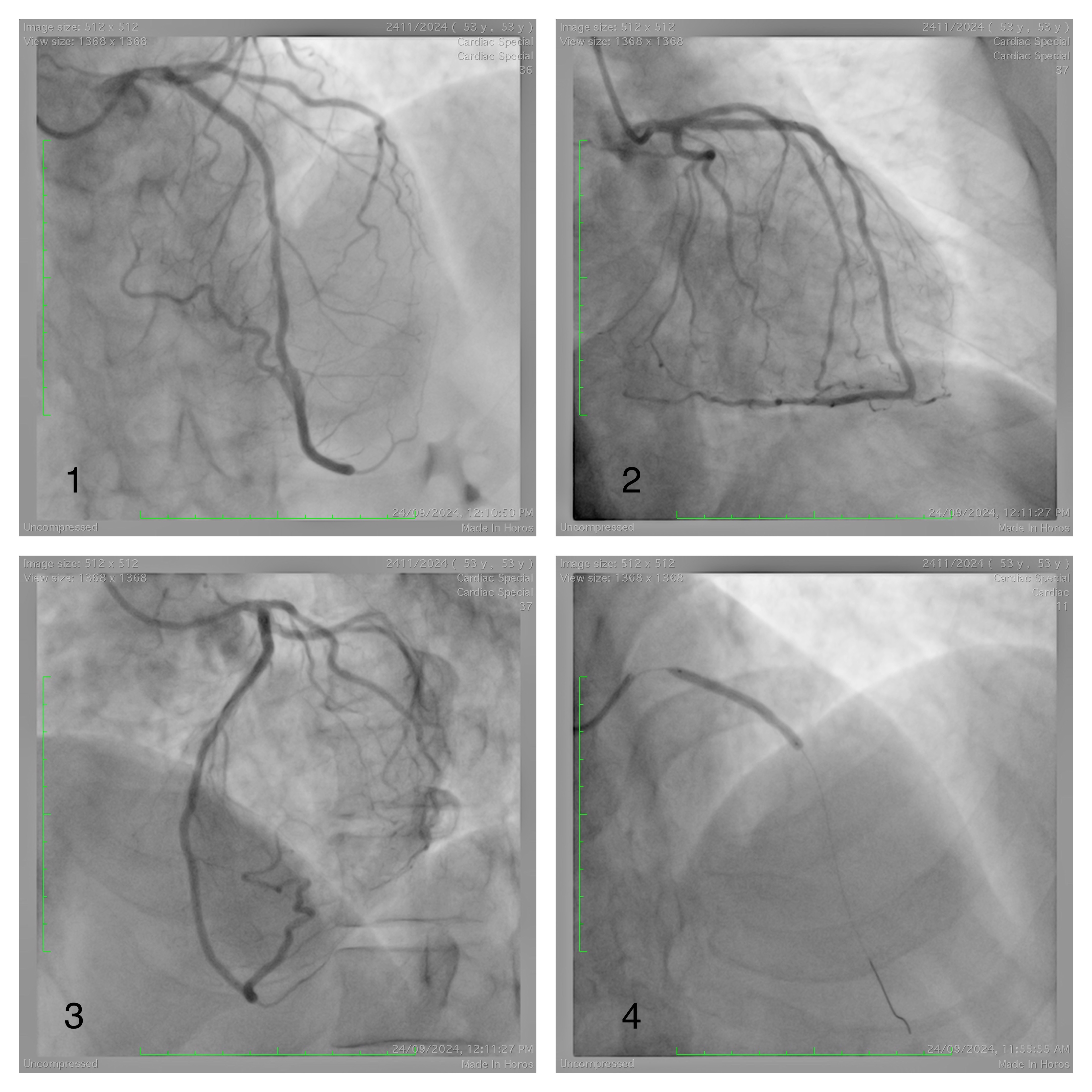
1,2,3 Post-PCI angiogram showing large "wrap around" "superdominant" LAD with PDA from LAD at different views
4 Stenting of proximal to mid LAD during primary PCI
Case Summary
This ia a rare variant of left dominant system with the "wrap around" LAD being very dominant supplying posterior wall of the left ventricle which is usually supplied by PDA branch arising from RCA in most patients apart from a portion of the inferior wall and the usual anterior territory. This type of LAD is often referred to as the "super dominant" LAD. The occlusion of this dominant LAD in proximal segment resulted in extensive anterior, inferior and lateral STEMI. This type of coronary anomaly cause no signs and symptoms and is usually found as incidental findings in the time of catheterization or other radiological investigations.