
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-078
A Challenging Case Report: Chronic Total Occlusion With Blunt Stump Calcification
By Yu Jui Hsieh, Chi-Jen Chang
Presenter
Yu Jui Hsieh
Authors
Yu Jui Hsieh1, Chi-Jen Chang1
Affiliation
Chang Gung Memorial Hospital, Taiwan1,
View Study Report
TCTAP C-078
Coronary - Complex PCI - CTO
A Challenging Case Report: Chronic Total Occlusion With Blunt Stump Calcification
Yu Jui Hsieh1, Chi-Jen Chang1
Chang Gung Memorial Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
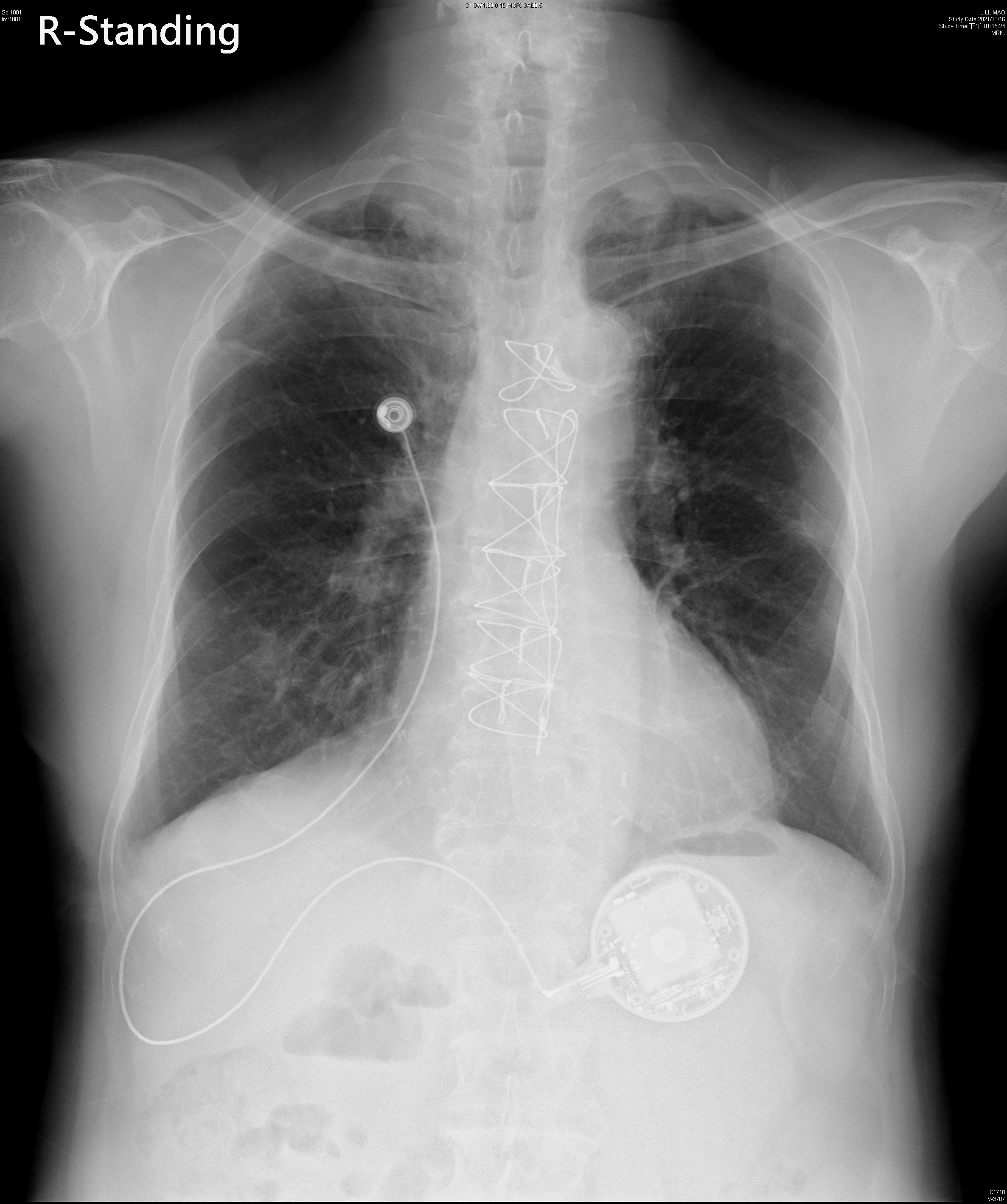
An 81-year-old man had a medical history of CAD status post CABG, with LIMA to LAD and SVG to PDA and OM. He had comorbidities of dyslipidemia and COPD, presenting with chronic dyspnoea on exertion. Recently, his exertional dyspnea worsened, accompanied by mild chest discomfort. There was no orthopnea or other associated symptoms. Physical examinations were grossly normal, which is not typical for AECOPD. With positive findings by myocardial perfusion scan, coronary angiography was arranged.
Relevant Test Results Prior to Catheterization
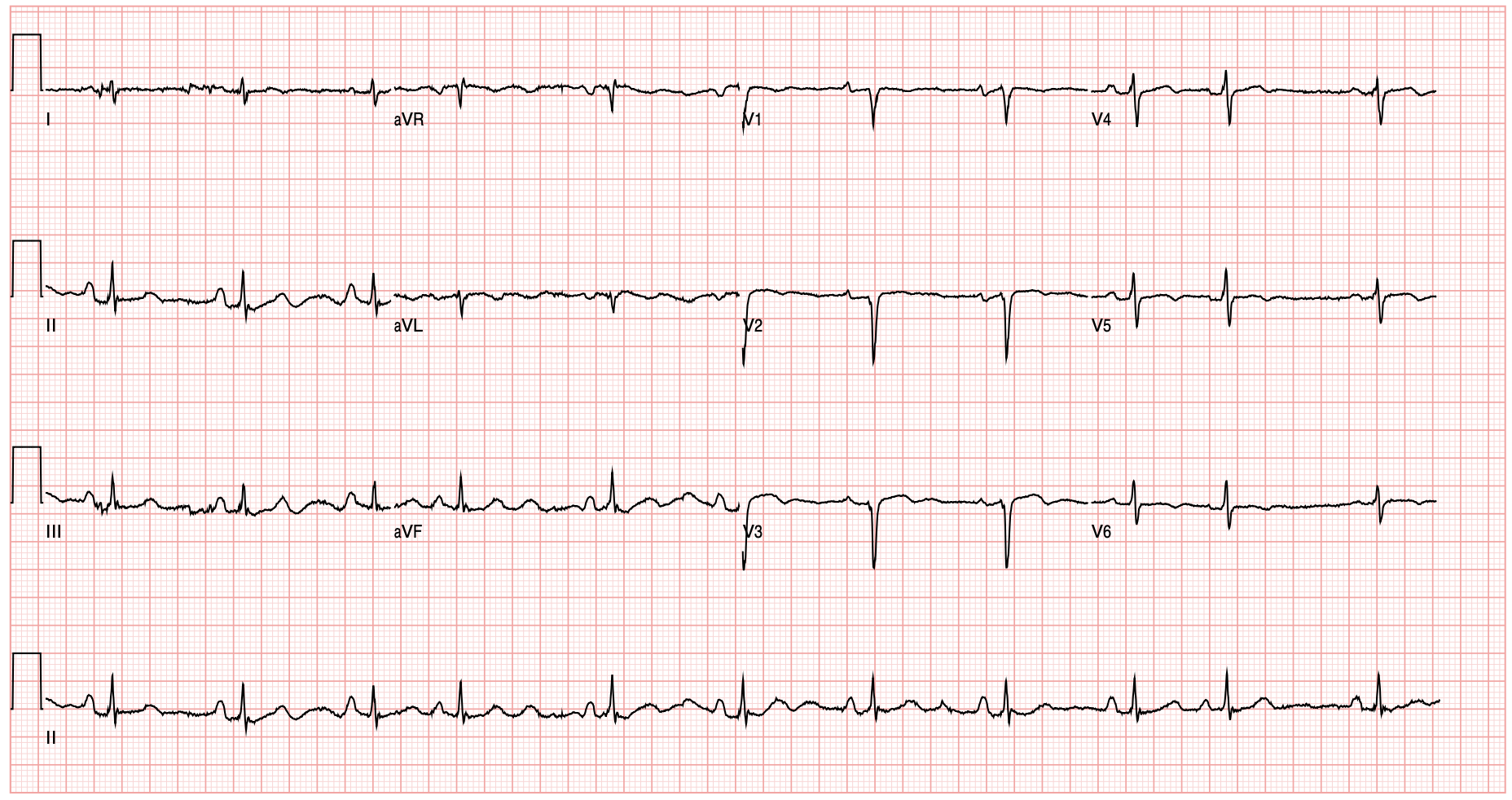
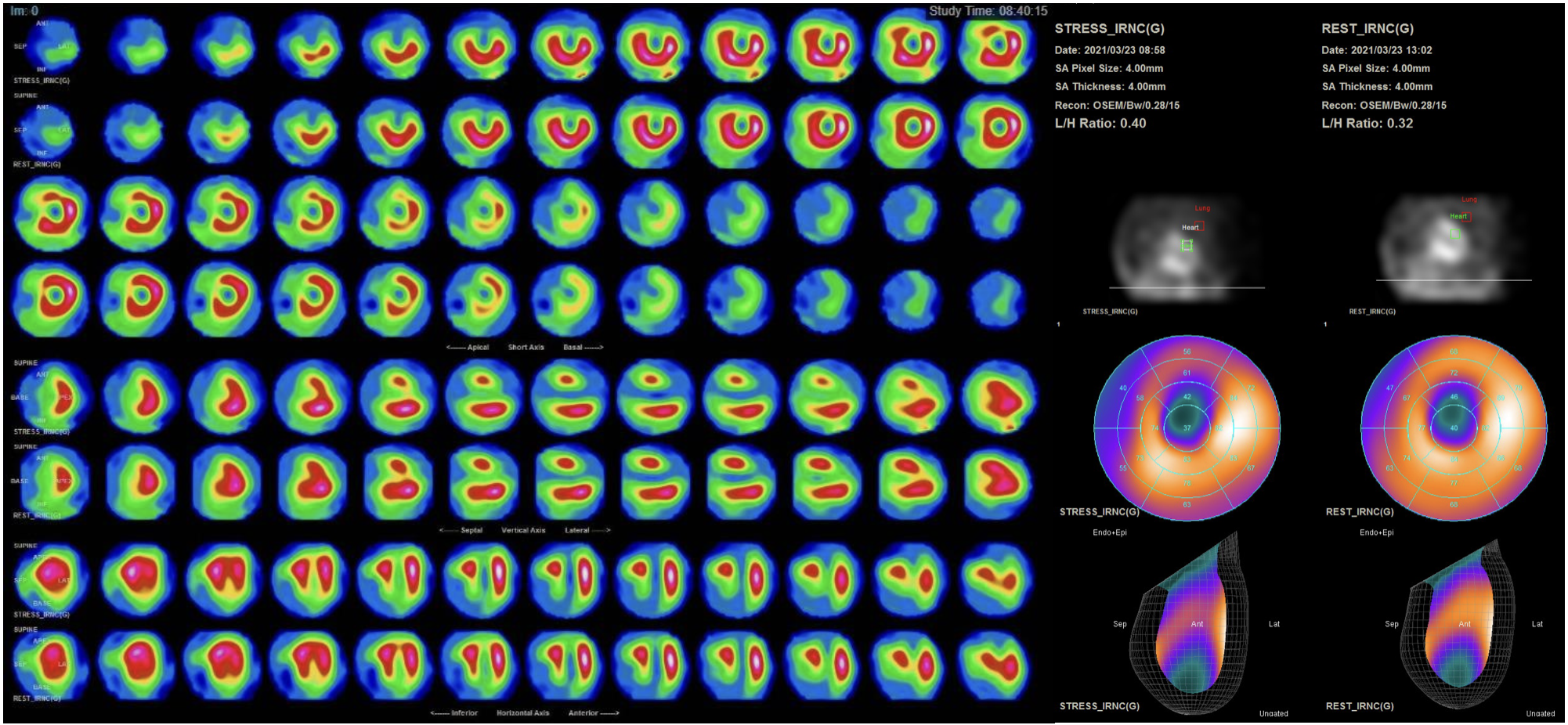
An annual echocardiogram revealed adequate left ventricular systolic function but hypokinesia in the anteroseptal segment. The electrocardiogram demonstrated sinus rhythm with premature atrial complexes. Additionally, an anteroseptal infarct pattern was recorded. A myocardial perfusion scan was performed. The images revealed mixed ischemia and infarction in the anterior and basal septal segments of the left ventricle. Cardiac catheterisation was scheduled based on the positive image results.
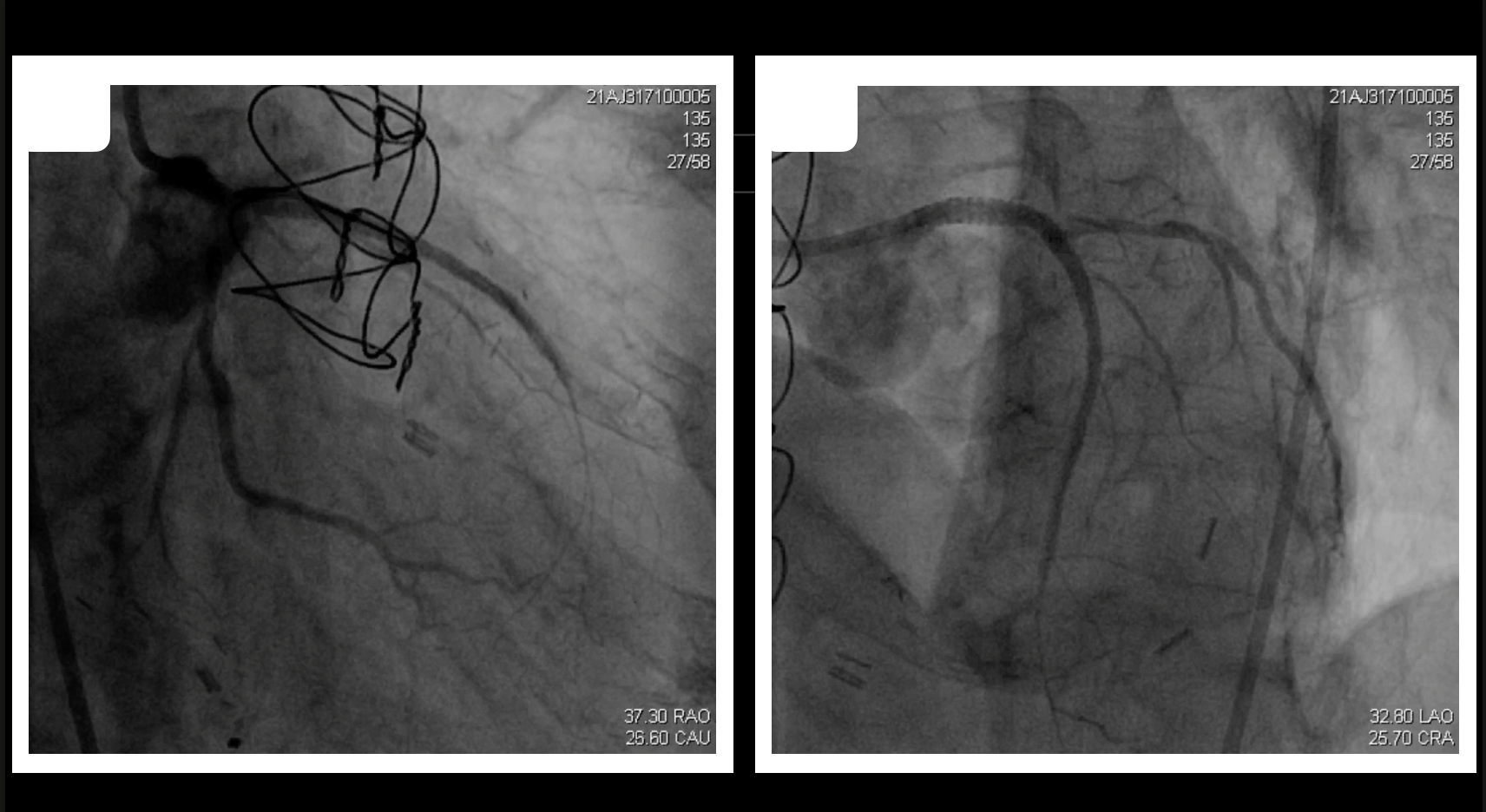
Relevant Catheterization Findings
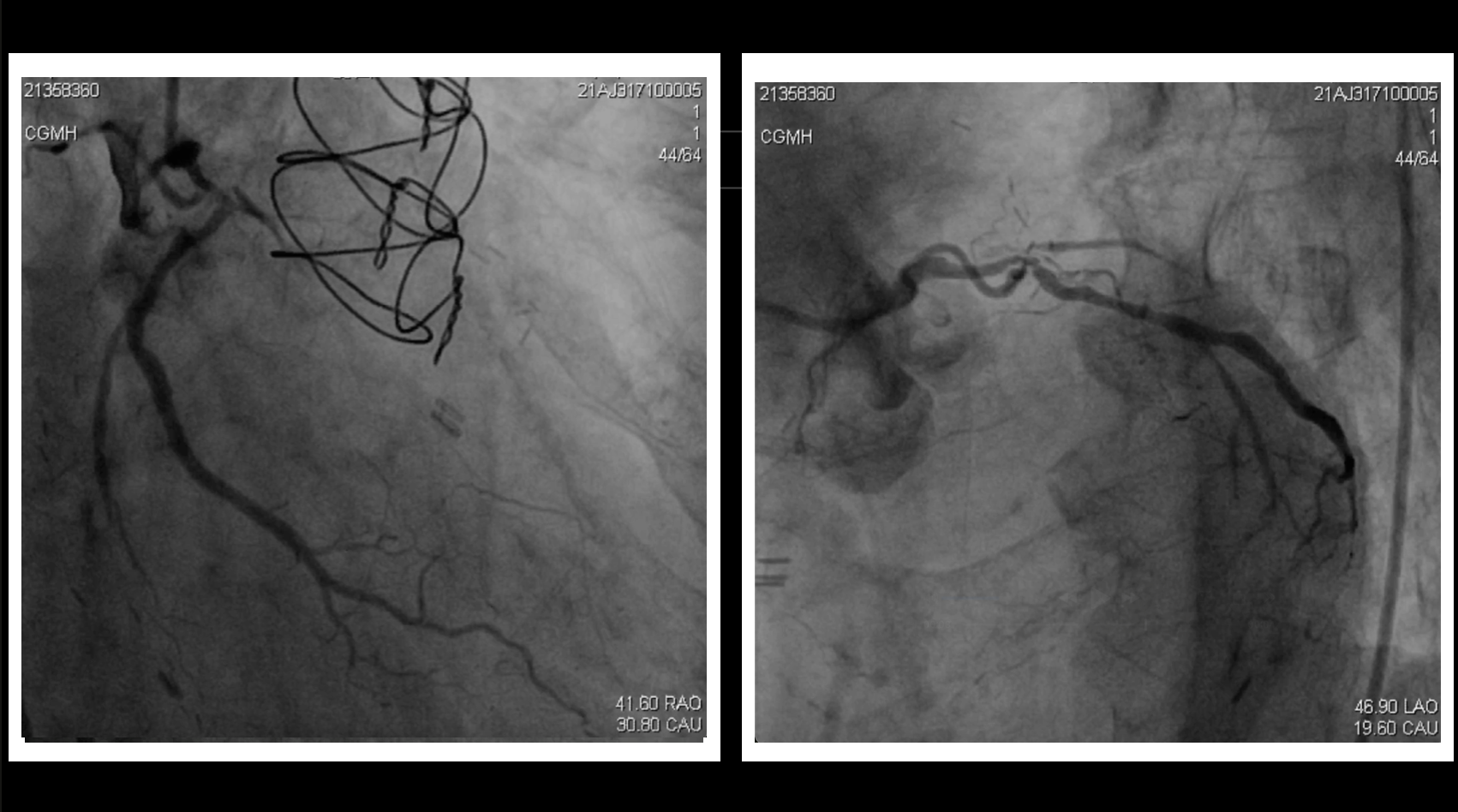
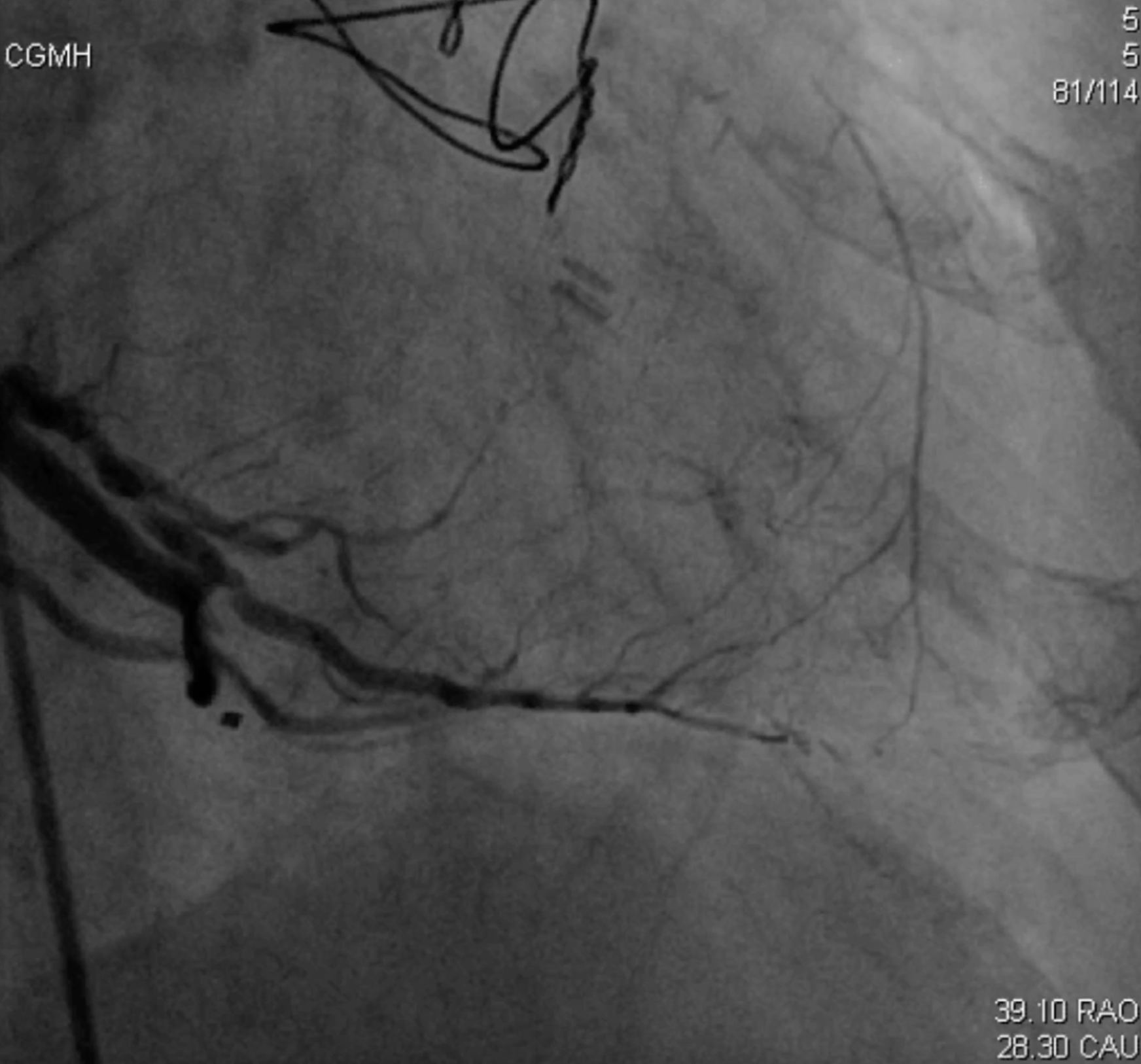
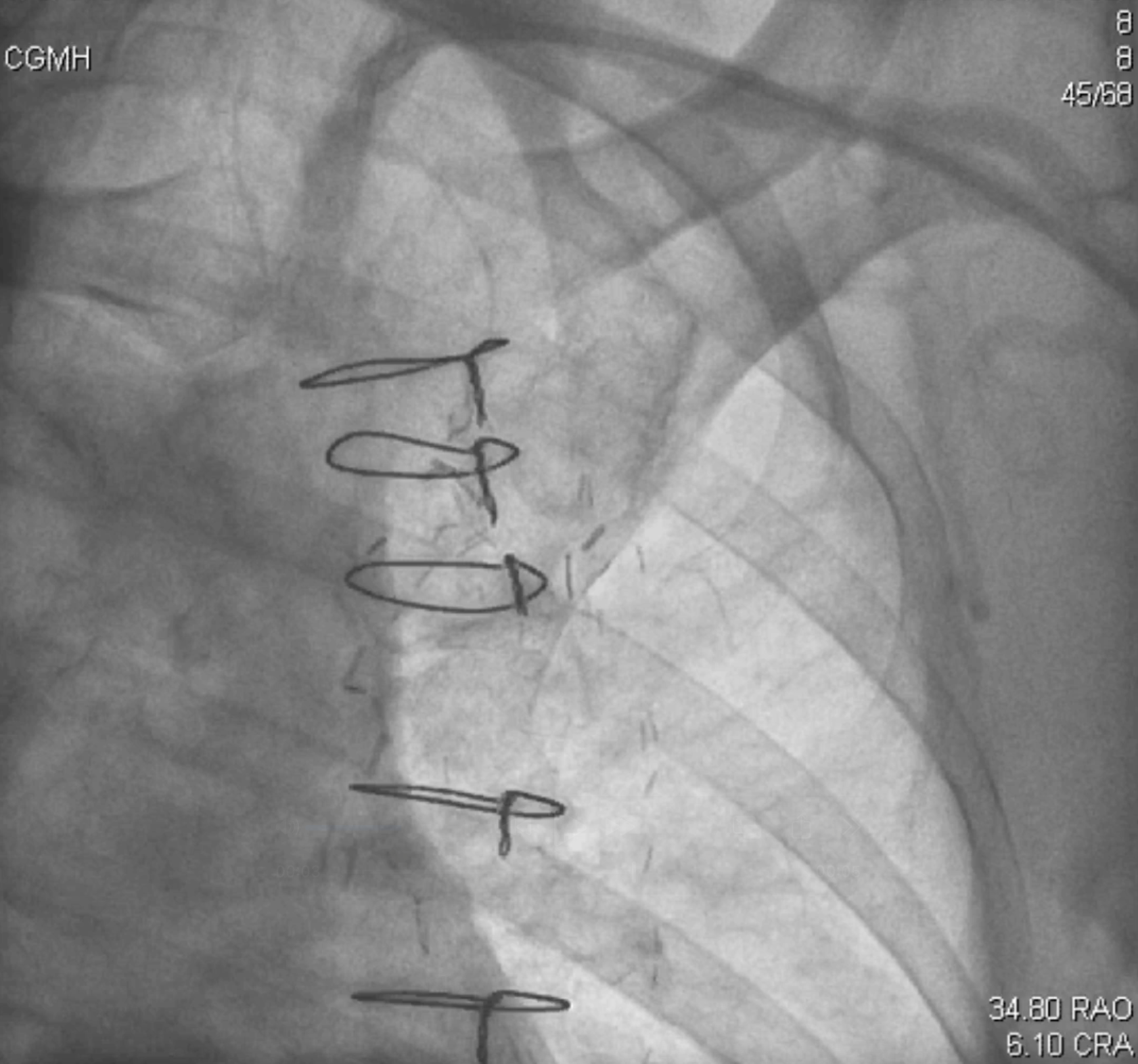
A coronary angiogram revealed calcification and diffuse stenosis in the LM coronary artery, with near-total occlusion at the distal bifurcation, followed by chronic total occlusion of the LAD at the calcified ostium. The LIMA graft was occluded. The LCX showed diffused atherosclerosis and significant stenosis in the proximal segment. The distal RCA was nearly total occluded, but the bypass graft from the SVG to the PDA was patent, providing collateral flow to the septal branch and distal LAD.
Interventional Management
Procedural Step
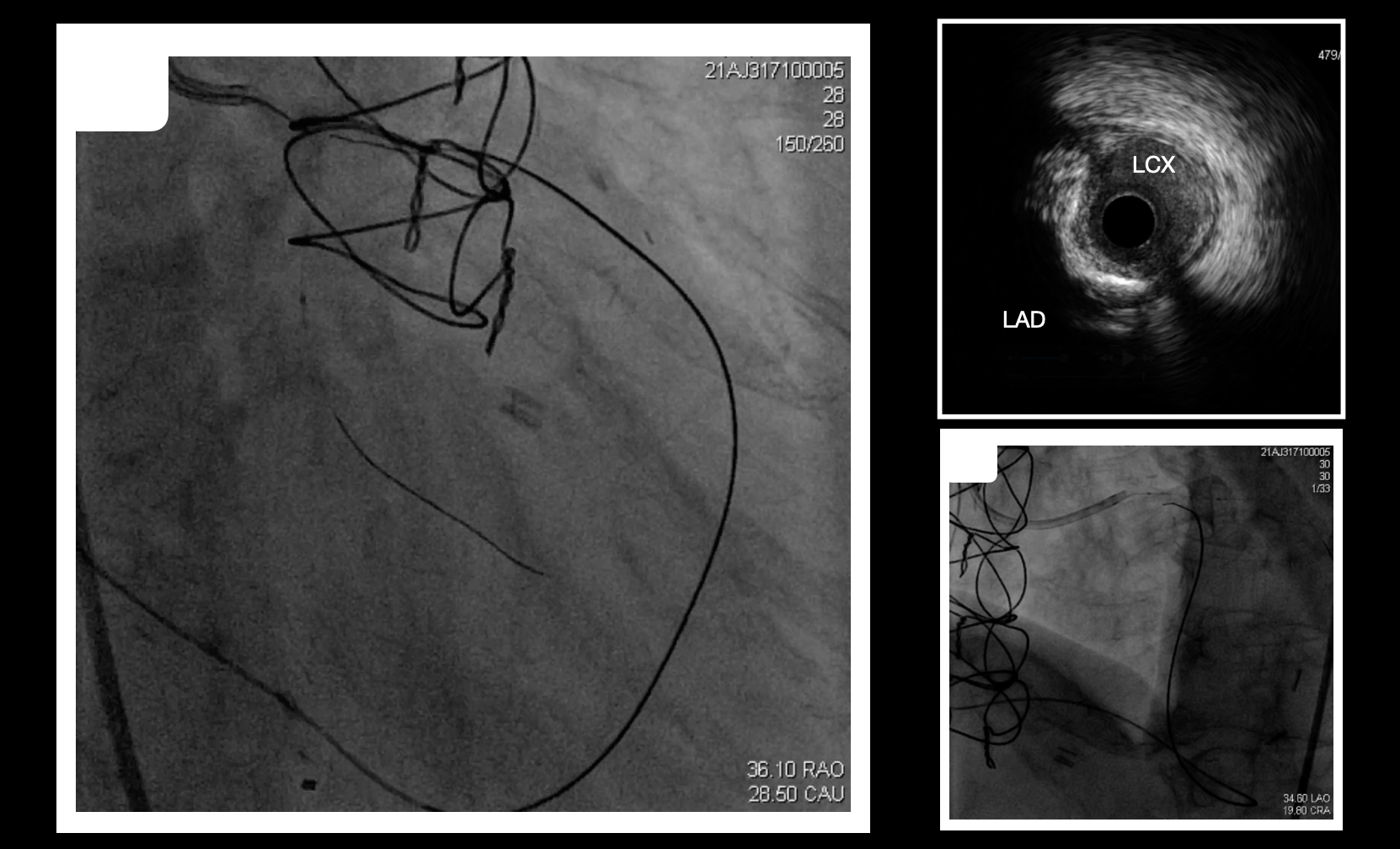
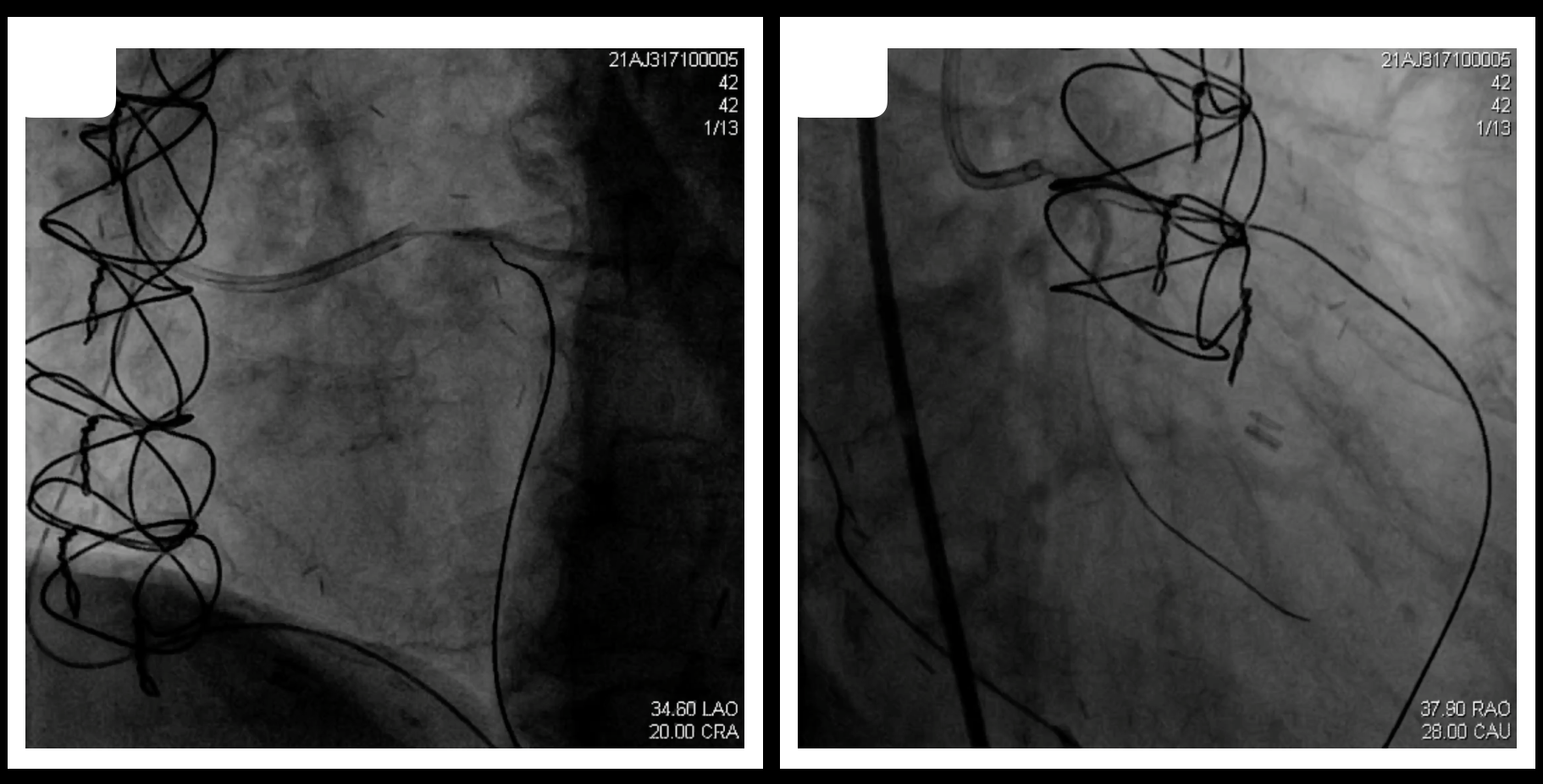
A 6F JR4 and a 7F EBU3.5 guiding catheter were engaged in the SVG and LCA. A retrograde approach was started due to poor identification of entry site of LAD by IVUS, which showed severe ostial calcification. We used Fielder FC wire and Cosair Pro microcatheter to reach the PDA via the SVG, employing septal surfing to access the distal LAD with a SION wire. However, the wires cannot across the total occlusion at proximal LAD. The antegrade wiring attempt failed due to a lack of a steady position at the ostial LAD for penetration. We attempted retrograde wiring using the Gaia series, placing a wire as a marker inside the LCX. However, both the Gaia Second and Gaia Third wires were unable to enter the true lumen. Real-time IVUS-guided wiring was ineffective, with poor image quality resulting from the ostial calcification of the LAD.While upgrading to a stiffer wire, a relatively small balloon was inflated at the LM bifurcation. The Conquest Pro was targeted at the inflated balloon and gradually penetrated through the calcification. The balloon was inflated for 20 seconds during each attempt. Eventually, the wire crossed the lesion at the proximal LAD and advanced into the distal LCX. We trapped the wire and advanced the microcatheter. The Fielder FC wire was exchanged and processed into the guiding catheter at the LM, completing externalization.After pre-dilatation, a 2.50mm DEB was inflated from the LM to the LCX. Provisional stenting was performed from the LM to the distal LAD.
Case Summary
Approaching a blunt stump with calcification in a chronic total occlusion is challenging. The bifurcation and calcification make the lesion difficult to cross using either antegrade or retrograde approach. Additionally, the calcification limits the effiectiveness of intravascular imaging. Avoiding subintimal tracking is crucial in LM bifurcation. Standard CTO wiring techniques may not effectively address the type of lesion. In this case, we applied an inflated balloon in the main vessel to magnify the target, increasing the likelihood of successful retrograde wire entry into the true lumen. This may be an effective and safe procedure for patients post CABG with adequate bypass graft supply.