
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-017
There's Nothing Left: Acute Left Main Occlusion
By Siew Hoon Ong, Faiz Mashood, Mugilan Sundarajoo, Hafiz Abd Hadi
Presenter
Siew Hoon Ong
Authors
Siew Hoon Ong1, Faiz Mashood1, Mugilan Sundarajoo1, Hafiz Abd Hadi1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-017
Coronary - ACS/AMI
There's Nothing Left: Acute Left Main Occlusion
Siew Hoon Ong1, Faiz Mashood1, Mugilan Sundarajoo1, Hafiz Abd Hadi1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
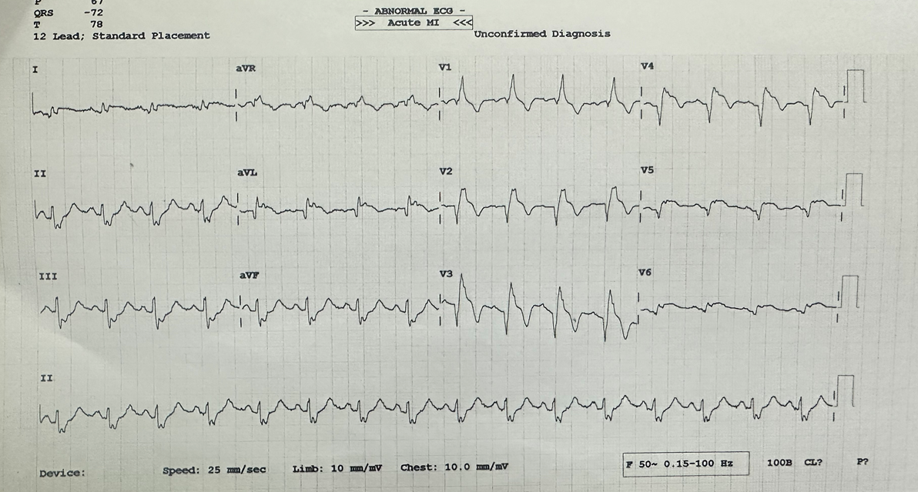
50 year-old man, who is an active smoker, presented to General Hospital with acute onset of epigastric pain after playing football. ECG showed ST elevation V2 to V5 with reciprocal changes in the inferior leads. He was diagnosed to have Acute extensive anterior MI and was referred to our center for primary PCI.
On arrival to our emergency department he was in distress, NYHA class II.
Relevant Test Results Prior to Catheterization
Bp: 140/70HR 100CVS dual rhythm no murmurLungs auscultation revealed bibasal crepitations Chest Xray : no cardiomegaly, ground glass opacities at right upper lobe lung, consolidation at right lower lobe and left lower lobe lung suggestive of pulmonary edema Bedside Echocardiogram: EF 40-45%, no dissection flap at aortic root.

Relevant Catheterization Findings


Interventional Management
Procedural Step
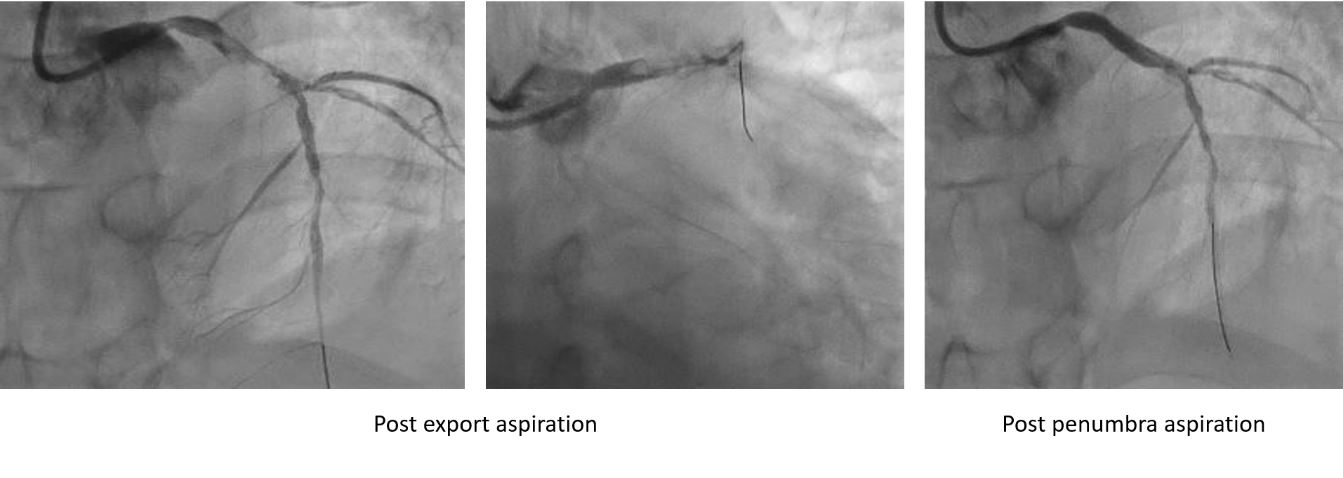
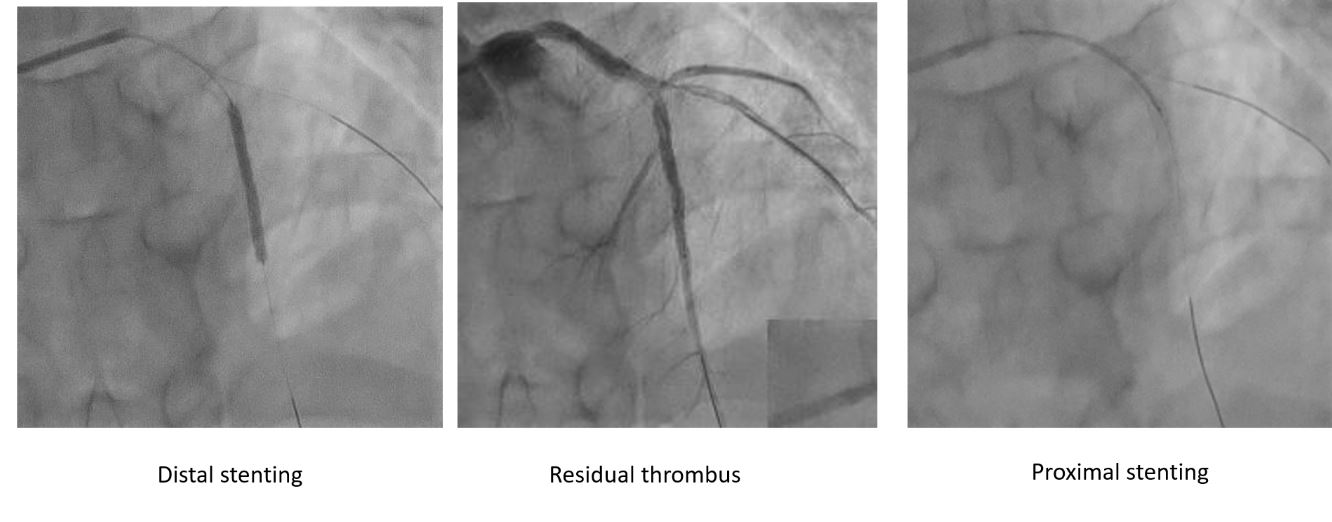
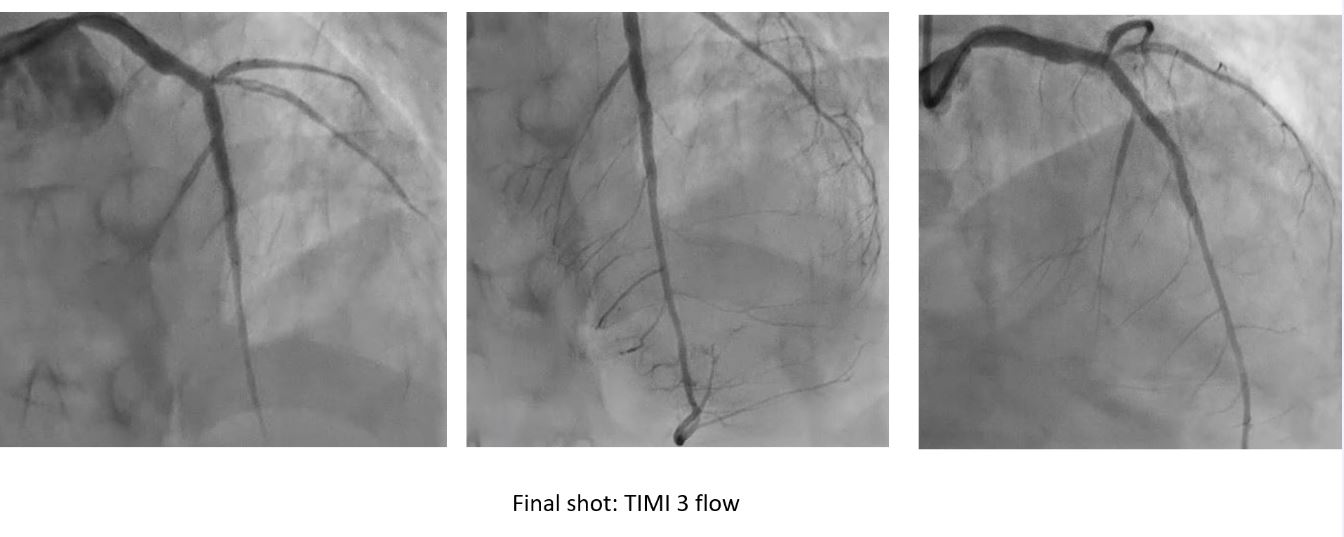
As soon as acute total occlusion was detected, left system was engaged with EBU 3.5 6FR, lesion was crossed with RTF into the LAD. Export catheter was sent down for thrombus aspiration, however only minimal thrombus. Decided to proceed with Penumbra aspiration in view of heavy thrombus burden. Lesion was then predilated with SC 3.0X15mm. After predilatation, flow to distal LAD was restored, decided to stent distal lesion with Cre8 2.75X33mm and then post-dilate with NC 3.0X15mm. Lesion was further prepared at the proximal LAD into distal LM with the same NC balloon. After preparation, noted residual thrombus in the proximal LAD and diagonal branch. Decided to stent the proximal LAD into proximal LM with Cre8 3.5X33mm, and post dilate with NC 3.5X15mm.Post LM stenting noted TIMI 1 distal flow and hence proceeded with aspiration with Penumbra, followed by IC Aggrastat 12mls over 3 minutes.Decided to POT LM with NC 3.5 again. We performed a post IVUS run that showed well opposed stent with no dissection. Final result showed TIMI III flow with no immediate complications.
Case Summary
Many patients with acute total occlusion of left main artery present with cardiogenic shock with significant number develop cardiac arrest. This patient survived a complete occlusion of LMCA with heavy thrombus burden giving the quick intervention with the PCI, he remained hemodynamically stable throughout the procedure, however his condition further deteriorated despite close and meticulous care in the CCU. Hence PCI procedure with intra-aortic balloon pump should be offered early for patient with STEMI complicated with cardiogenic shock as this is very critical in improving survival rates for those patients.