
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-203
Navigating Complexity: From Collapse to Recovery With Successful TAVI, PCI and ECMO in a High-Risk Patient
By Tsz Ho Chan, Hei Tung Chan, Ling Na Wong, Chak Yu Kent So, Ka Ho Kevin Kam, Ho Lam, Ka Lung Chui, Eugene B Wu, Yat Sun Joseph Chan
Presenter
Tsz Ho Chan
Authors
Tsz Ho Chan1, Hei Tung Chan2, Ling Na Wong2, Chak Yu Kent So2, Ka Ho Kevin Kam2, Ho Lam3, Ka Lung Chui2, Eugene B Wu2, Yat Sun Joseph Chan2
Affiliation
Pok Oi Hospital, Hong Kong, China1, Prince of Wales Hospital, Hong Kong, China2, Tuen Mun Hospital, Hong Kong, China3,
View Study Report
TCTAP C-203
Structural - Aortic Valve Intervention - Complex TAVR
Navigating Complexity: From Collapse to Recovery With Successful TAVI, PCI and ECMO in a High-Risk Patient
Tsz Ho Chan1, Hei Tung Chan2, Ling Na Wong2, Chak Yu Kent So2, Ka Ho Kevin Kam2, Ho Lam3, Ka Lung Chui2, Eugene B Wu2, Yat Sun Joseph Chan2
Pok Oi Hospital, Hong Kong, China1, Prince of Wales Hospital, Hong Kong, China2, Tuen Mun Hospital, Hong Kong, China3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 63 years old man with history of diabetes, hyperlipidemia, end stage renal failure on peritoneal dialysis was admitted for loss of consciousness and chest discomfort
Initially blood pressure was stable and no oxygen was required.
Before completion of the workup, the patient developed hypotension required inotropic support and later expereienced 2 episodes of sudden cardiac arrest presenting as pulseless electrical activity, with good neurological recovery after resuscitation
Relevant Test Results Prior to Catheterization
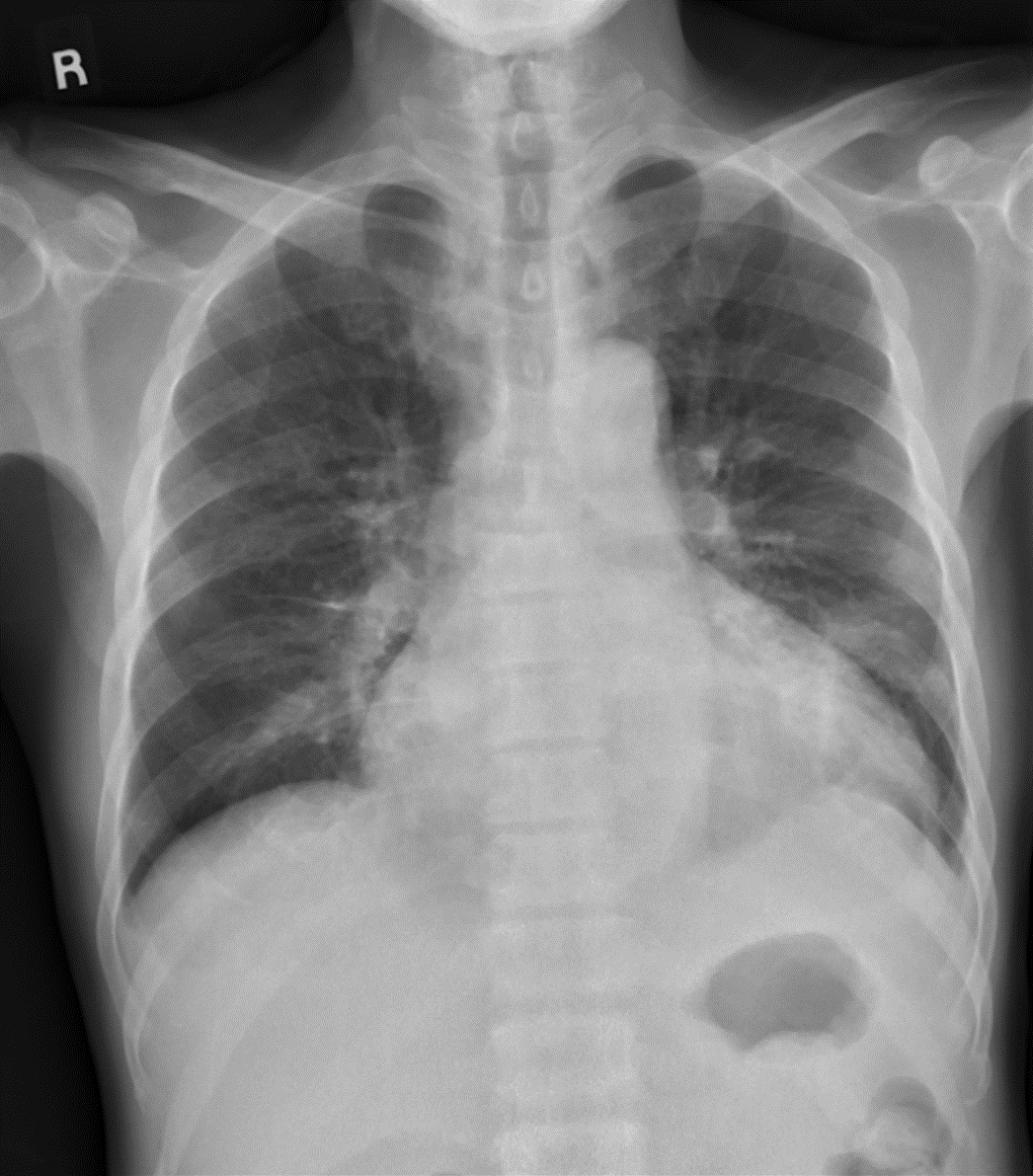
CXR: Cardiomegaly
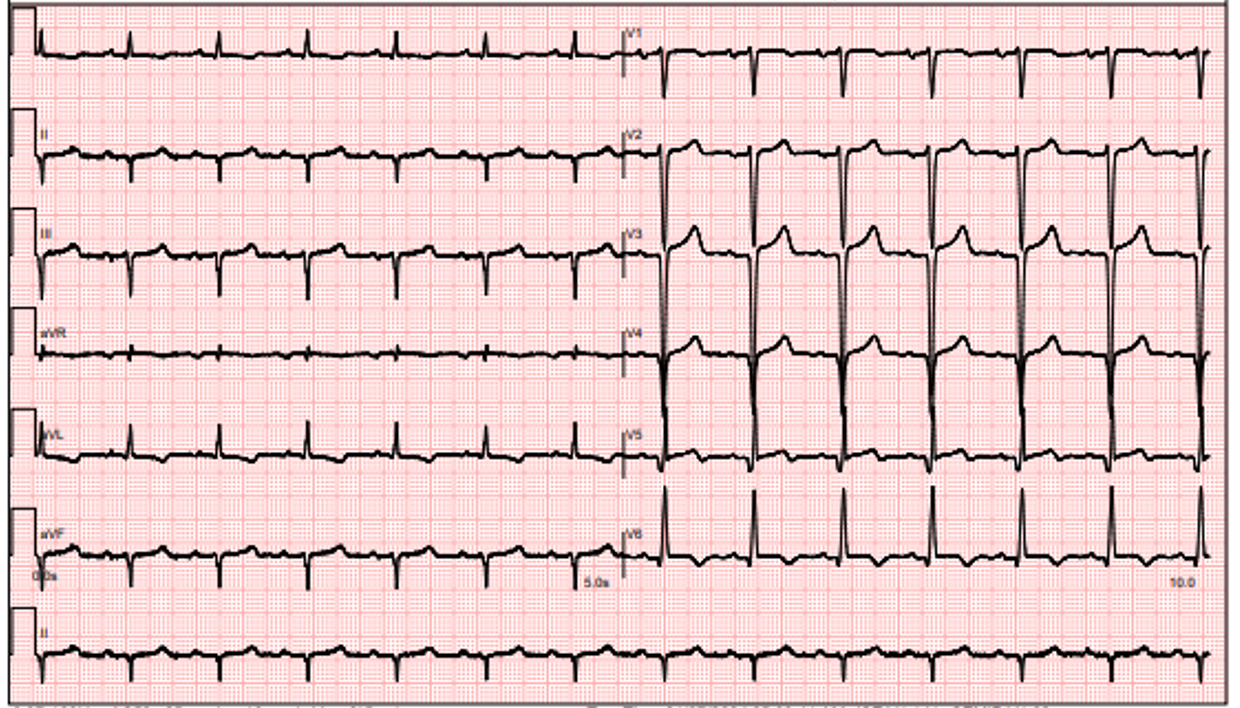
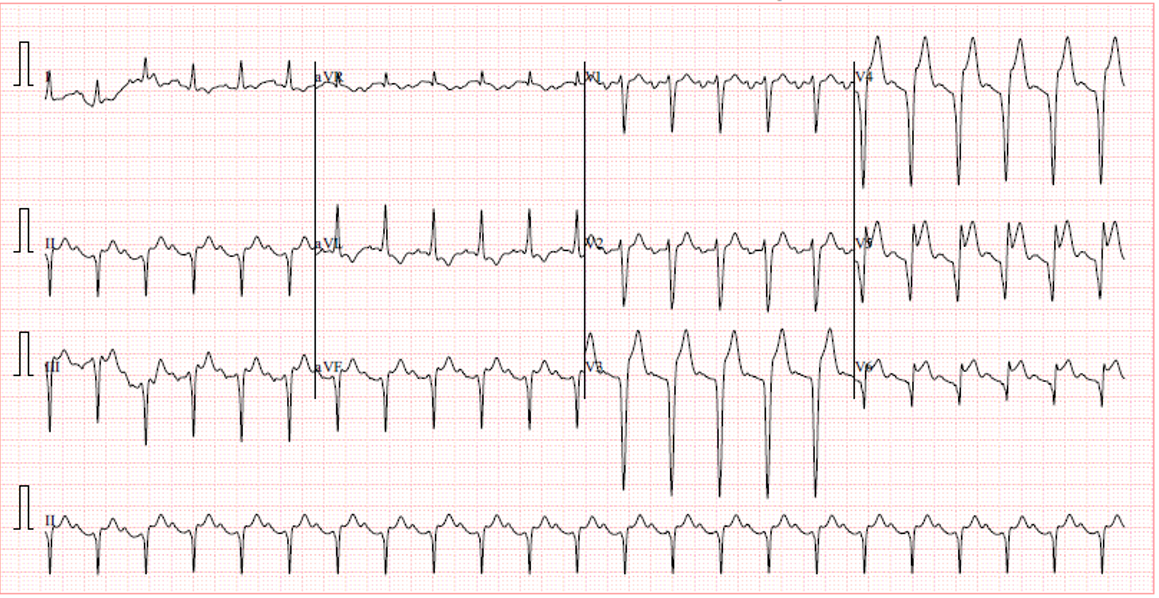
ECG: New ST elevation over anterior leads
Troponin I: Elevation with a peak >50,000
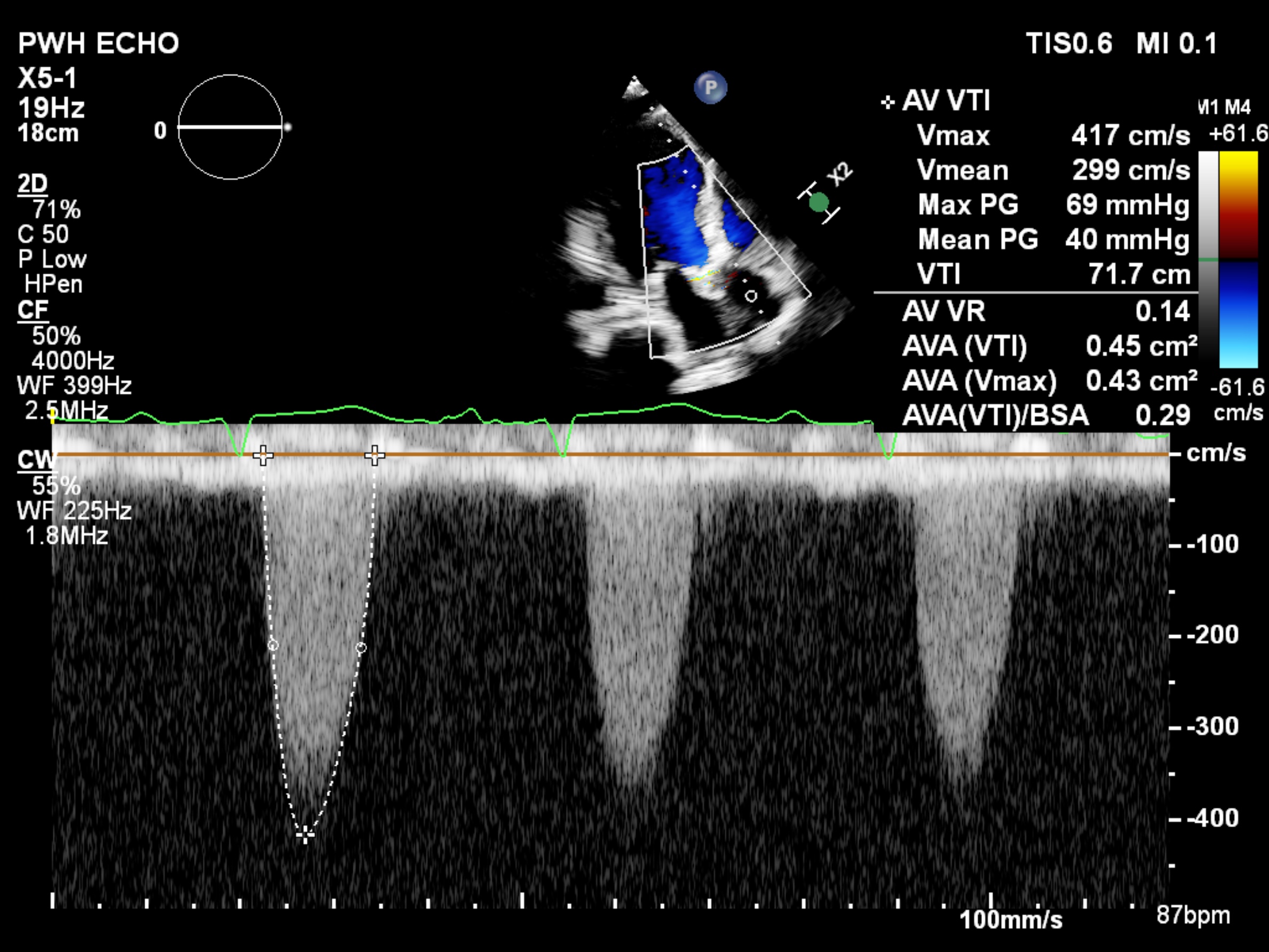
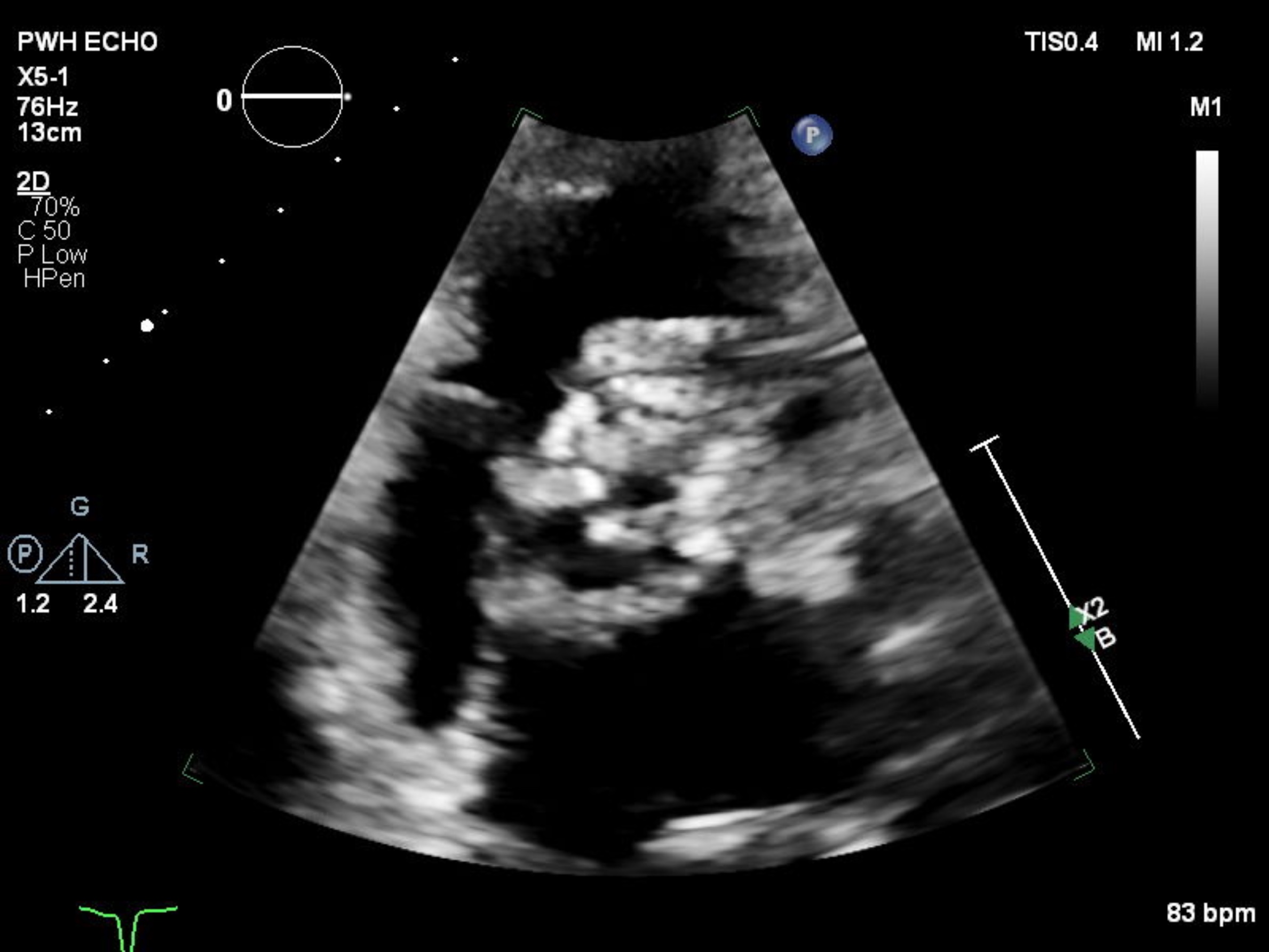
Echocardiogram: LVEF around 25%, global hypokinesia, calcified aortic valve, Severe AS ( AV Vmax 4.17m/s, Mean gradient 40mmHg, AVA 0.45cm2, AV VR 0.14) , moderate AR, MR and TR, RVSP 49mmHg
Pre TAVI CT analysis : Suitbale anatomy for TAVI
Relevant Catheterization Findings
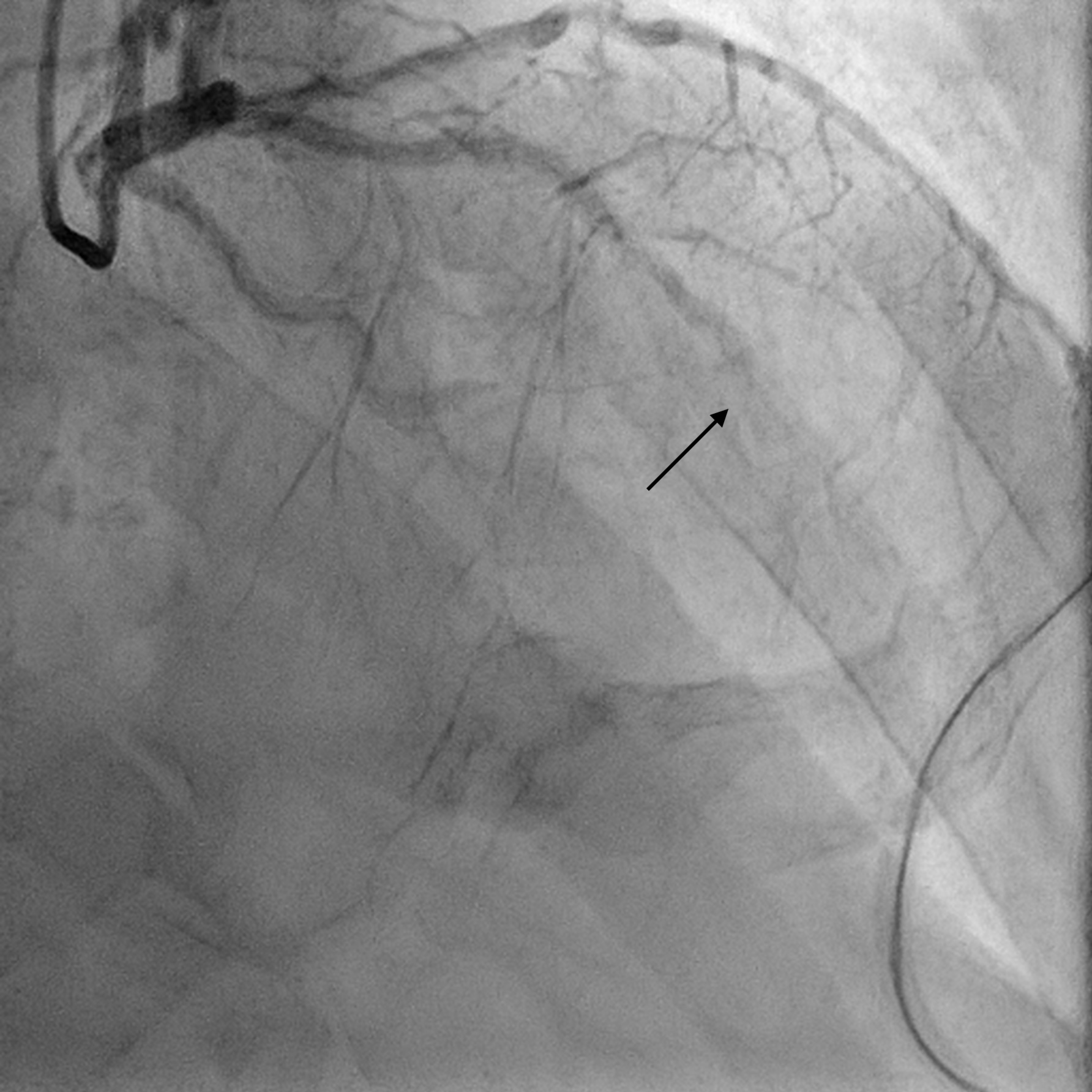
Coronary angiogram LM: Normal LAD: mLAD total occlusion LCX: dLCX total occlusion RCA: Dominant, severe lesion over a small distal PL branch

Interventional Management
Procedural Step
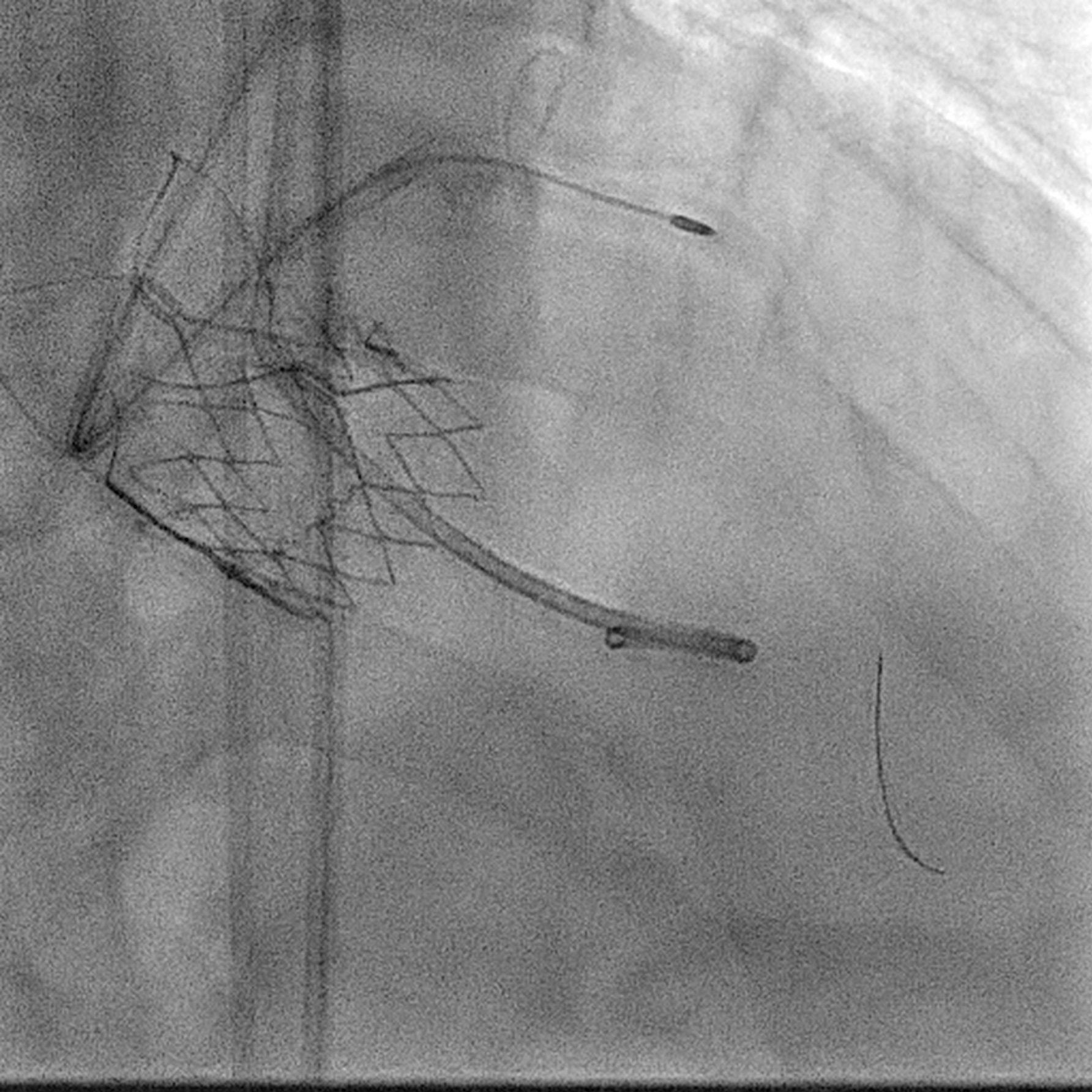
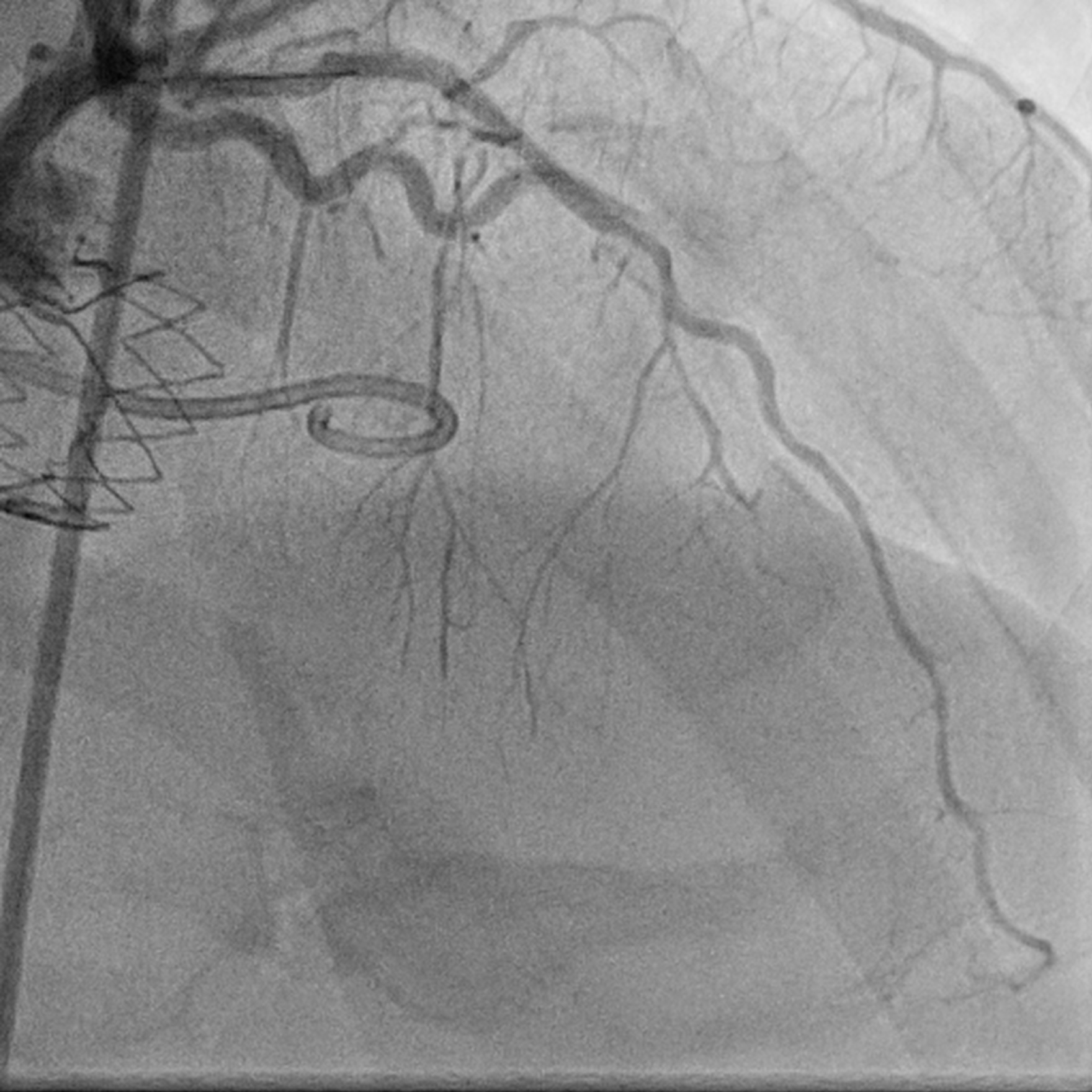
After heart team discussion, the patient was deemed unsuitable for open heart surgery due to prohibited risks. TAVI and PCI were planned for the same session In view of inotropes dependent, challenging anatomy for PCI and moderate AR, we opted for mechanical circulatory support rather than balloon aortic valvuloplasty, proceeding with TAVI before PCI. ECMO circuit was established via the left femoral artery and veinRight Femoral artery was used as major access and R radial artery as minor access for TAVIThe AV was predilated by True balloon, followed by Accurate NEO 2 valve deployed with Commissural alignment achieved. During deployment of valve, on top of rapid pacing required, the ECMO flow also need to be turned down to very low flow to minimize the risks of valve embolization.After TAVR done, LAD lesion was managed by EBU 3.5Fr guiding catheter. Due to large open cells of valve with commissural alignment achieved, the guiding catheter was engaged easily. The lesion was prepared by rotablator and non compliant balloon. In view of torturosity, eccentric calcified long lesion, we decided to managed with DCB. Final result showed TIMI 3 flow of LADThroughout the procedure patient's hemodynamics was stableInotropes were weaned off. ECMO flow reversed and patient tolerated well. Therefore ECMO was off on same procedure. Bilateral artery access was closed by preclosed proglide, providing possiblity of artery reaccess in case needed shortly. Final angiogram showed hemostatis achieved
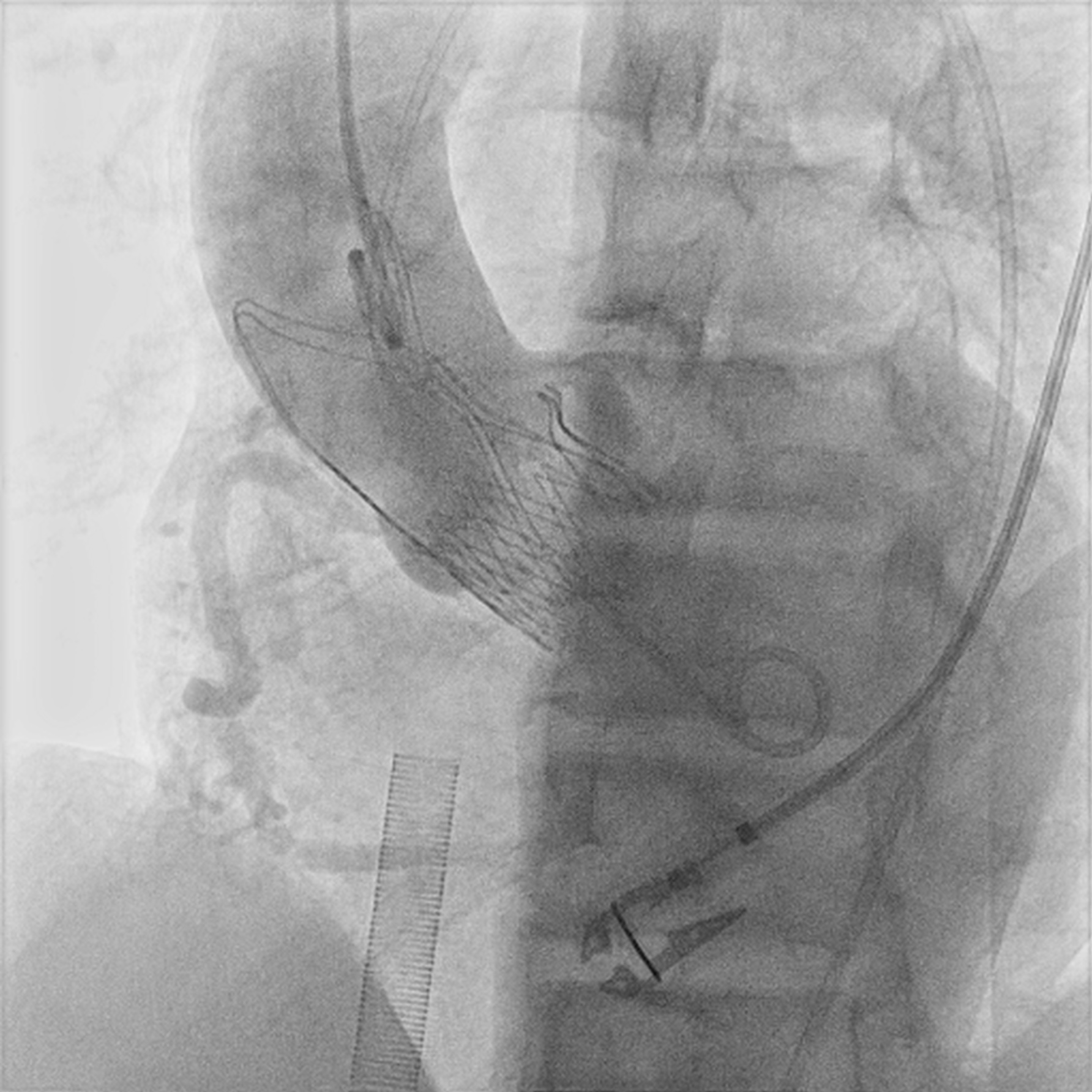
 TAVI implant with commissural alignment.jpg
TAVI implant with commissural alignment.jpg
Case Summary
Severe AS, Acute coronary syndrome with cardiogenic shock carry a high mortality risk. Prompt management is essential, but meticulous planning is necessary to determine the seequence of mechanical circulatory support, TAVI and PCI This case demonstrates the successful completion of PCI followed by TAVI and ECMO within the same procedure. With the use of ECMO support, the patient's hemodynamic remained stable throughout the procedure. Utilizing TAVI with an open-cell design with commissural alignment technqiue enabled the team to access coronary arteries effectively using a supportive guiding catheter in this complex case.