
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-075
When Both Side Microcatheters Could Not Pass in a Right Coronary CTO
By Chanhan Hu, Cheng-Yu Ko
Presenter
Cheng-Yu Ko
Authors
Chanhan Hu1, Cheng-Yu Ko1
Affiliation
National Cheng Kung University Hospital, Taiwan1,
View Study Report
TCTAP C-075
Coronary - Complex PCI - CTO
When Both Side Microcatheters Could Not Pass in a Right Coronary CTO
Chanhan Hu1, Cheng-Yu Ko1
National Cheng Kung University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
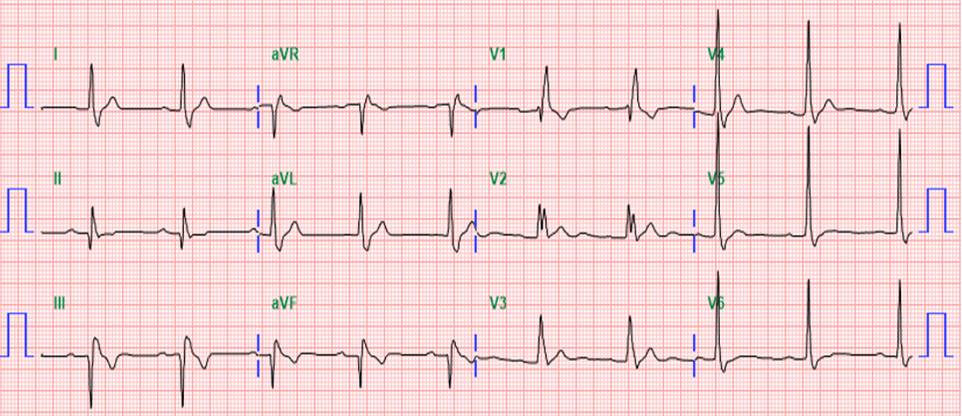
The patient is a 62-year-old man with smoking history. He sufferred from typical chest pain for six months. The baseline EKG showed sinus rhythm with RBBB. A preserved ejection fraction but basal-inferior hypokinesis was found on echocardiography. A treadmill exercise test was positive for ischemia. He therefore underwent coronary angiography.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
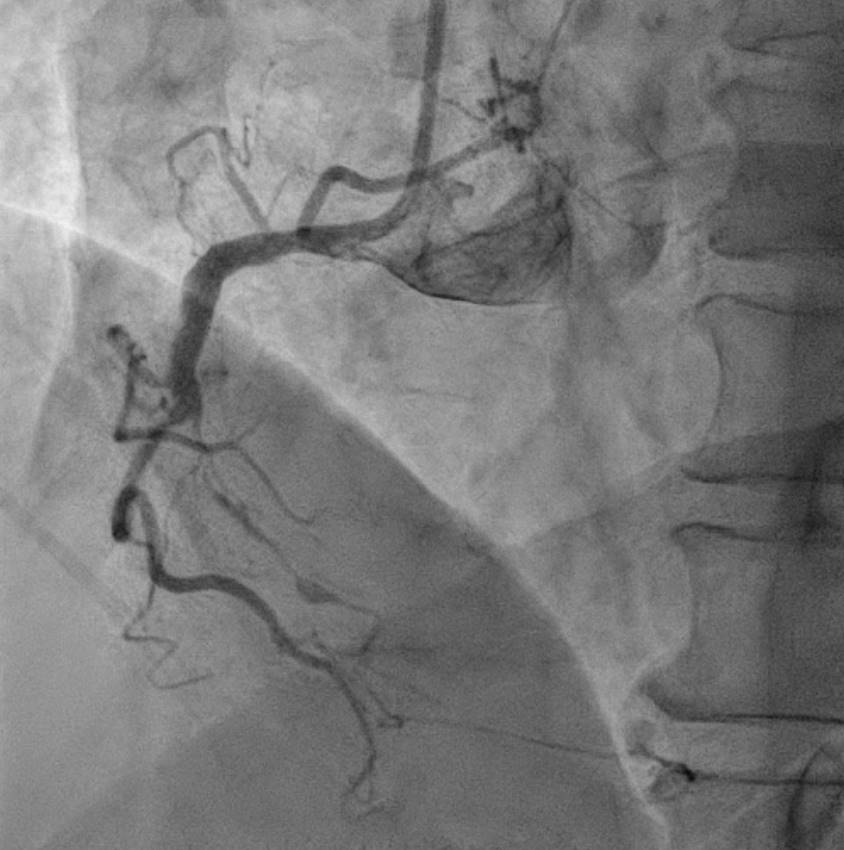
Coronary angiograpgy showed an middle RCA CTO, with septal collateral from LAD to PDA. The patient underwent an unsuccessful PCI attempt about one month before the index procedure, via RCA antegrade approach. However, due to persistent symptoms, he asked for second opinion and was admitted for another PCI attempt. Our strategy started with dual injection, The JCTO was 3 with long lesion, calcification, and re-attempt. We engaged RCA using AL1 guiding catheter, and LCA using EBU guiding catheter.

Interventional Management
Procedural Step
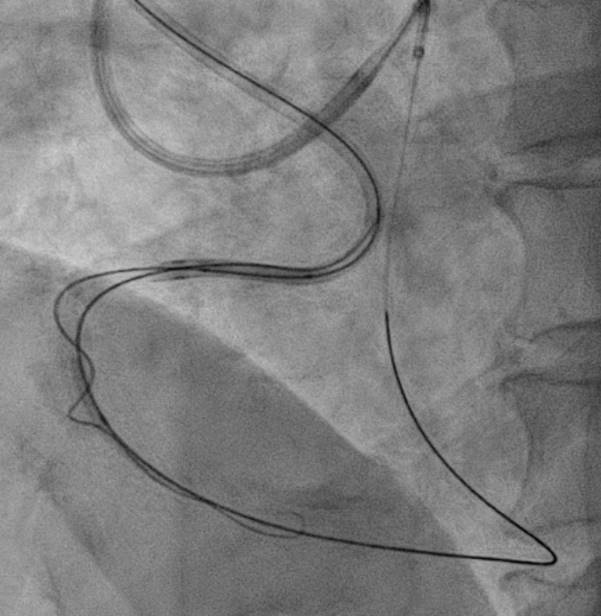
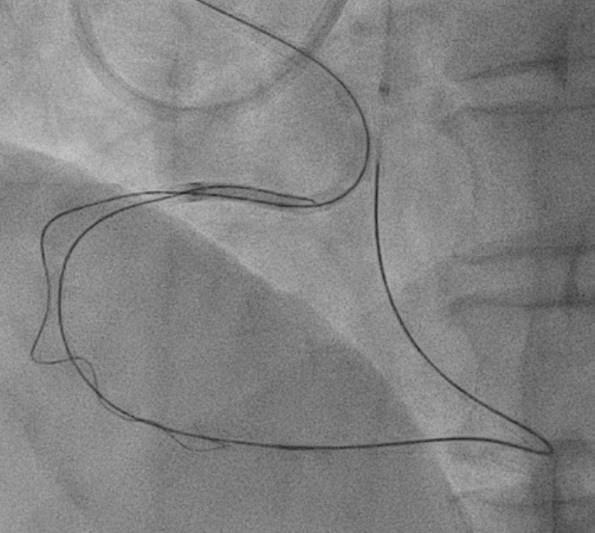
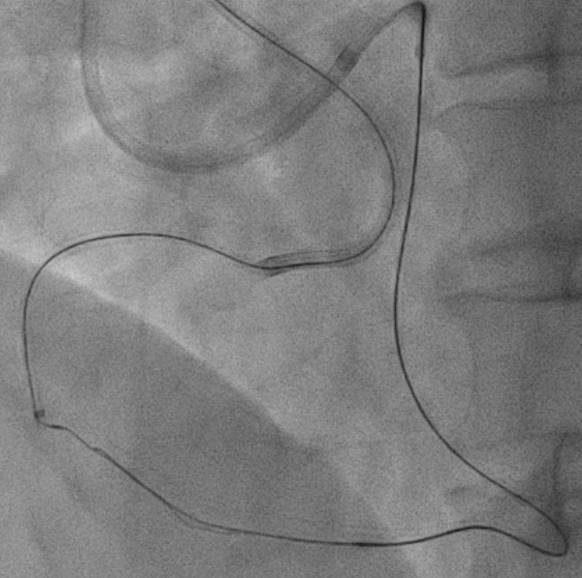
The strategy we plan was antegrade preparation and early retrogradly approach, due to challenging antegrade approach and also distal bifurcation1.XTA+Caravel microcatheter for antegrade preparation, failed advancement in mRCA2.retrograde with suoh03, but could not advance caravel and cosair pro microcatheters through septal channel3.extension catheter use, and balloon dilation for septal channel with low pressure4.caravel could enter dRCA, distal injection5.retrograde wire escalation for calcified CTO: Gaia2, Gaia3, Conquest pro6.kissing wire technique within dRCA7.both side MC could not pass the CTO, despite both side extension catheter use(img: step01)8.intracoronary tip-in, with retrograde wire anchored within AL1(img: step02)9.still failed advancing both side MC10.retrograde balloon dilation, sequentially from distal to middle RCA(img: step03)11.successful antegrade wiring to PL12.lesion preparation and drug-eluting stent placement13.good final angiography results
Case Summary
For this complex CTO case, we applied the following methods for a successful PCI:1. better support by using AL and EBU guiding catheters, both side extension catheters and microcatheters2. switching microcatheters3. septal channel dilation for microcatheter advancement4. tip-in technique, and then antegrade balloon anchor 5. retrograde balloon dilation when both side microcatheters could not pass the CTO lesion and failed by antegrade balloon dilation