
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-167
Large and Ectatic Coronary Artery: Leaving Nothing Behind
By Koon Wee Koay, Lean Seng Chen, Kuo Ting Lee, Shahul Hamid Ka Ahmadsah, Poi Keong Kong, Mohamed Jahangir Abdul Wahab
Presenter
Koon Wee Koay
Authors
Koon Wee Koay1, Lean Seng Chen1, Kuo Ting Lee1, Shahul Hamid Ka Ahmadsah1, Poi Keong Kong1, Mohamed Jahangir Abdul Wahab1
Affiliation
Penang General Hospital, Malaysia1,
View Study Report
TCTAP C-167
Coronary - DES/BRS/DCB
Large and Ectatic Coronary Artery: Leaving Nothing Behind
Koon Wee Koay1, Lean Seng Chen1, Kuo Ting Lee1, Shahul Hamid Ka Ahmadsah1, Poi Keong Kong1, Mohamed Jahangir Abdul Wahab1
Penang General Hospital, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
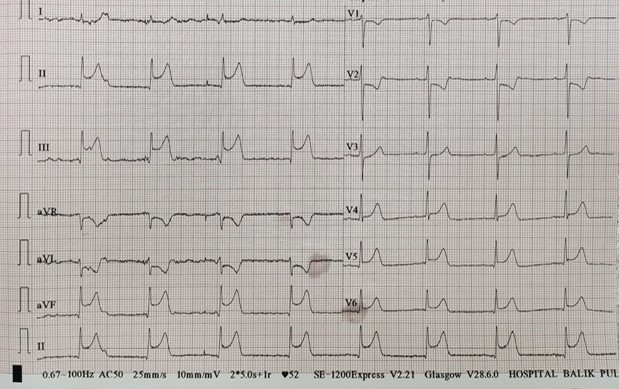
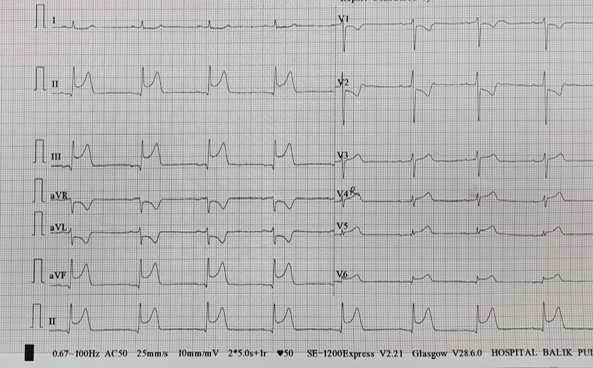
A 60 years old gentleman who has underlying hypertension and dyslipidaemia presented with sudden onset of chest pain associated with diaphoresis. He went to the nearest community hospital. ECG showed sinus rhythm with ST elevation at lead II, III, aVF, rV4-rV6. He was given intravenous streptokinase and transferred to our hospital. Upon arrival, his vital signs were stable but his chest pain persisted. We decided to activate our catheter laboratory in view of failed reperfusion.
Relevant Test Results Prior to Catheterization
Bedside echocardiogram showed left ventricular ejection fraction 45% with hypokinesia at inferolateral, inferoseptal, inferior and anteroseptal wall.
Relevant Catheterization Findings
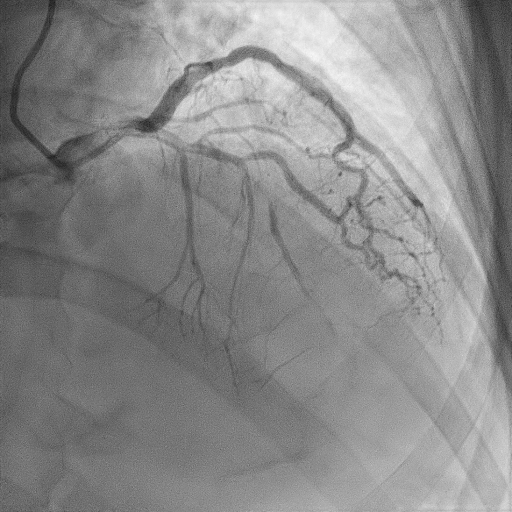
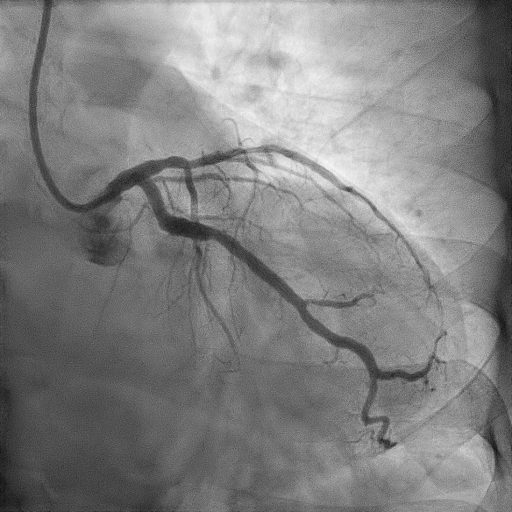
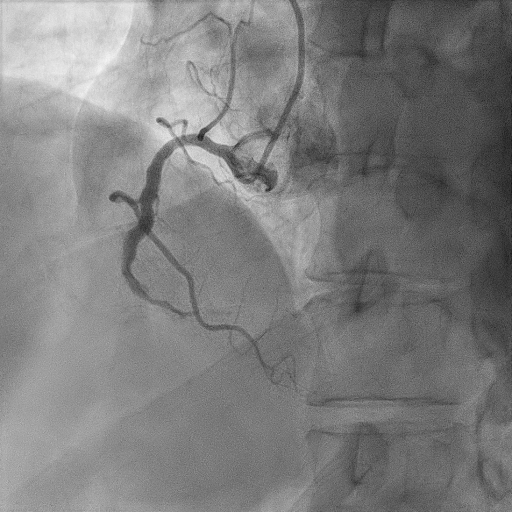
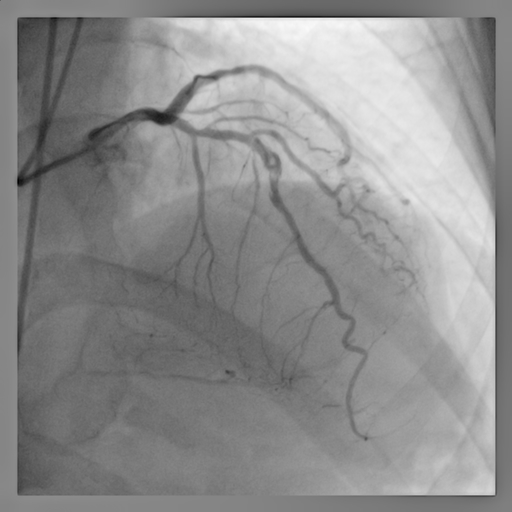
Coronary angiogram of the left coronary system showed subtotal occlusion of the mid left anterior descending (LAD) artery, minor disease at the left circumflex (LCX) artery. The right coronary artery (RCA) is a dominant artery with subtotal occlusion at the distal RCA. It was a double occlusion at both distal RCA and mid LAD with TIMI 1 flow.
Interventional Management
Procedural Step
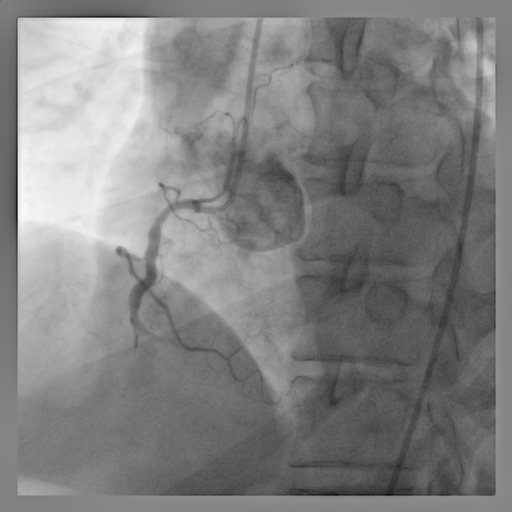
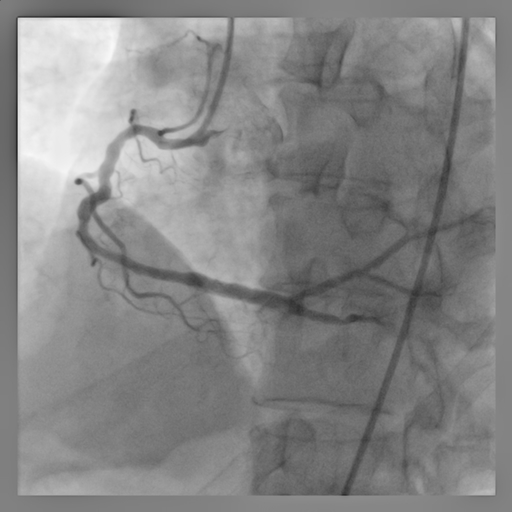
The RCA was engaged with a 6 Fr XBRCA guiding catheter. The distal RCA occluded lesion was crossed by workhorse wire and predilated with a 2.5mm semicompliant (SC) balloon. There was large thrombus burden at the distal RCA and hence manual thromboaspiration was done. TIMI 2 flow was established and we decided to defer stenting in view of high thrombus burden. The left coronary artery was engaged with 6Fr XB guiding catheter. The mid LAD occluded lesion was crossed by workhorse wire and subsequently predilated with a 2.5mm SC balloon. TIMI 2 flow established at LAD. Patient was started on anticoagulant for 1 week. Repeated coronary angiogram 1 week later showed a total occlusion at distal RCA and remnant thrombus at mid LAD with TIMI 3 flow. The distal RCA was wired with workhorse wire and predilated with a 2.5mm SC balloon. Flow was established and it showed an ectatic segment at distal RCA. It was further prepared with a 3.5mm scoring balloon and 4.0mm non-compliant (NC) balloon. A 4.0mm drug coated balloon (DCB) was deployed at distal RCA. Final result showed TIMI 3 flow at RCA. Patient was started on triple therapy for 1 month before changing to dual therapy. Repeated angiogram after 3 months showed good luminal gain at RCA with TIMI 3 flow. There was an aneurysm after the mid LAD stenotic lesion and therefore DCB strategy was opted as well. The mid LAD was prepared and deployed with a 2.5mm DCB. Final result was good with minimal recoil.
Case Summary
This case showed the usage of drug coated balloon (DCB) in a large and ectatic culprit RCA in an inferior STEMI with 3 months follow-up angiography showing a good result. In ectatic vessel, there is always size discrepancy between the normal and the ectatic segment and hence it poses a challenge for proper stent size selection and ensuring good stent apposition. The advantage of DCB usage is it will prevent leaving a permanent metal scaffold and reduce the risk of stent thrombosis. Currently, DCB is widely used for the treatment of in-stent restenosis and small vessel disease. It is an option for large vessel if the lesion is prepared adequately with no significant recoil or dissection.