
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-101
Drug-Eluting Balloon as a Bridging Strategy in CTO After Rotational Atherectomy
By Shi-Chue Hsing
Presenter
Shi-Chue Hsing
Authors
Shi-Chue Hsing1
Affiliation
Tri-Sevice General Hospital, Taiwan1,
View Study Report
TCTAP C-101
Coronary - Complex PCI - CTO
Drug-Eluting Balloon as a Bridging Strategy in CTO After Rotational Atherectomy
Shi-Chue Hsing1
Tri-Sevice General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
71 year old man with history of HTN, type 2DM and hyperlipidemia
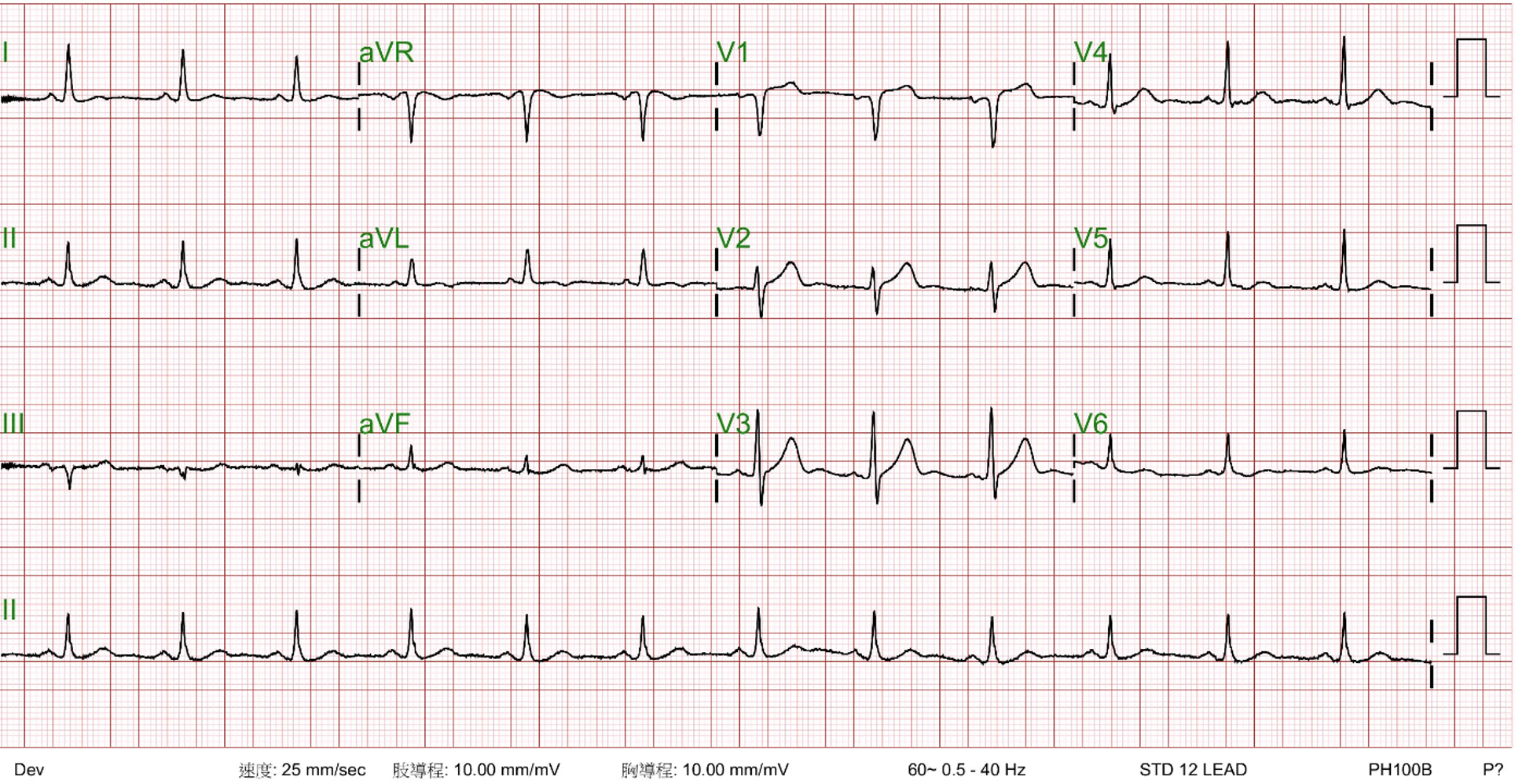
Relevant Test Results Prior to Catheterization
LDL 85 mg/dL; HbA1c 7.6%; Cre 1.1 mg/dL
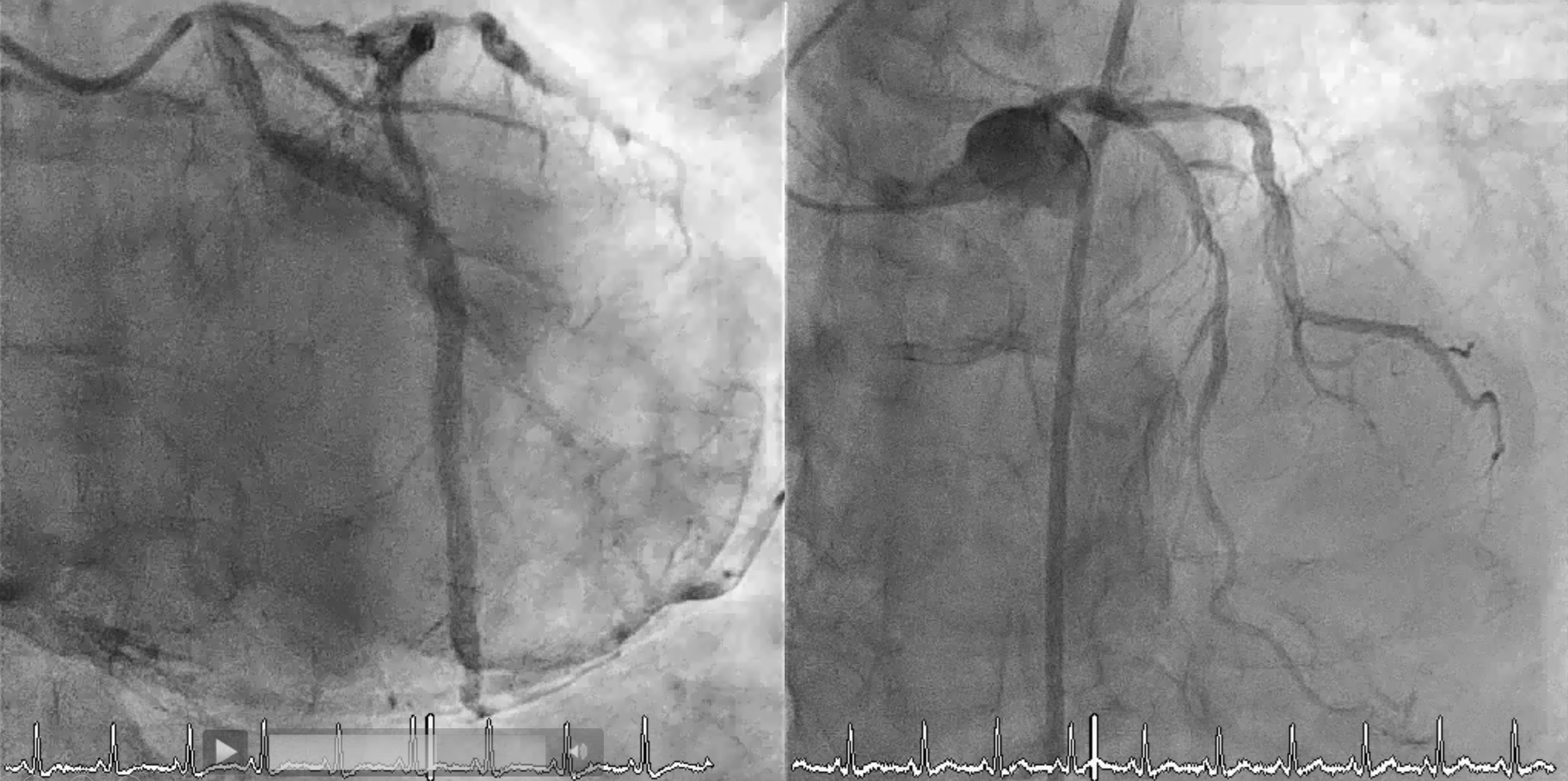
Relevant Catheterization Findings
Diagnosticcoronary angiography revealed: Chronic total occlusion (CTO) in the rightcoronary artery (RCA) with heavy calcification; Diffuse lesion in the leftanterior descending (LAD) artery; Proximal lesion in the left circumflex (LCx)artery; LAD providing collateral flow to the RCA.


Interventional Management
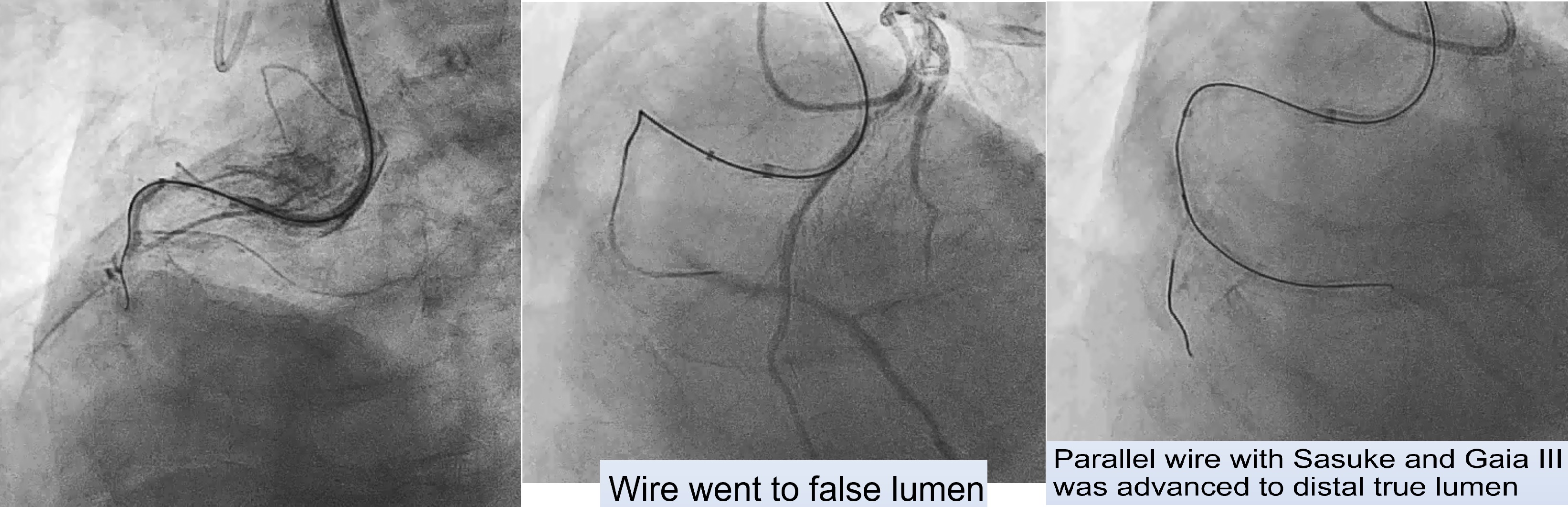
Procedural Step
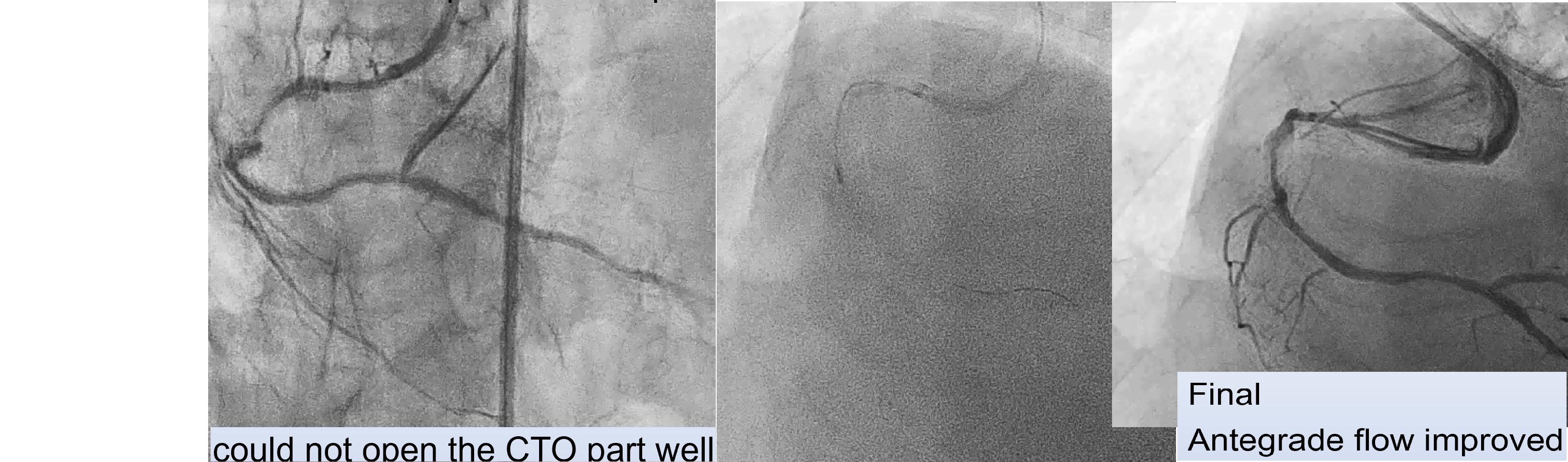
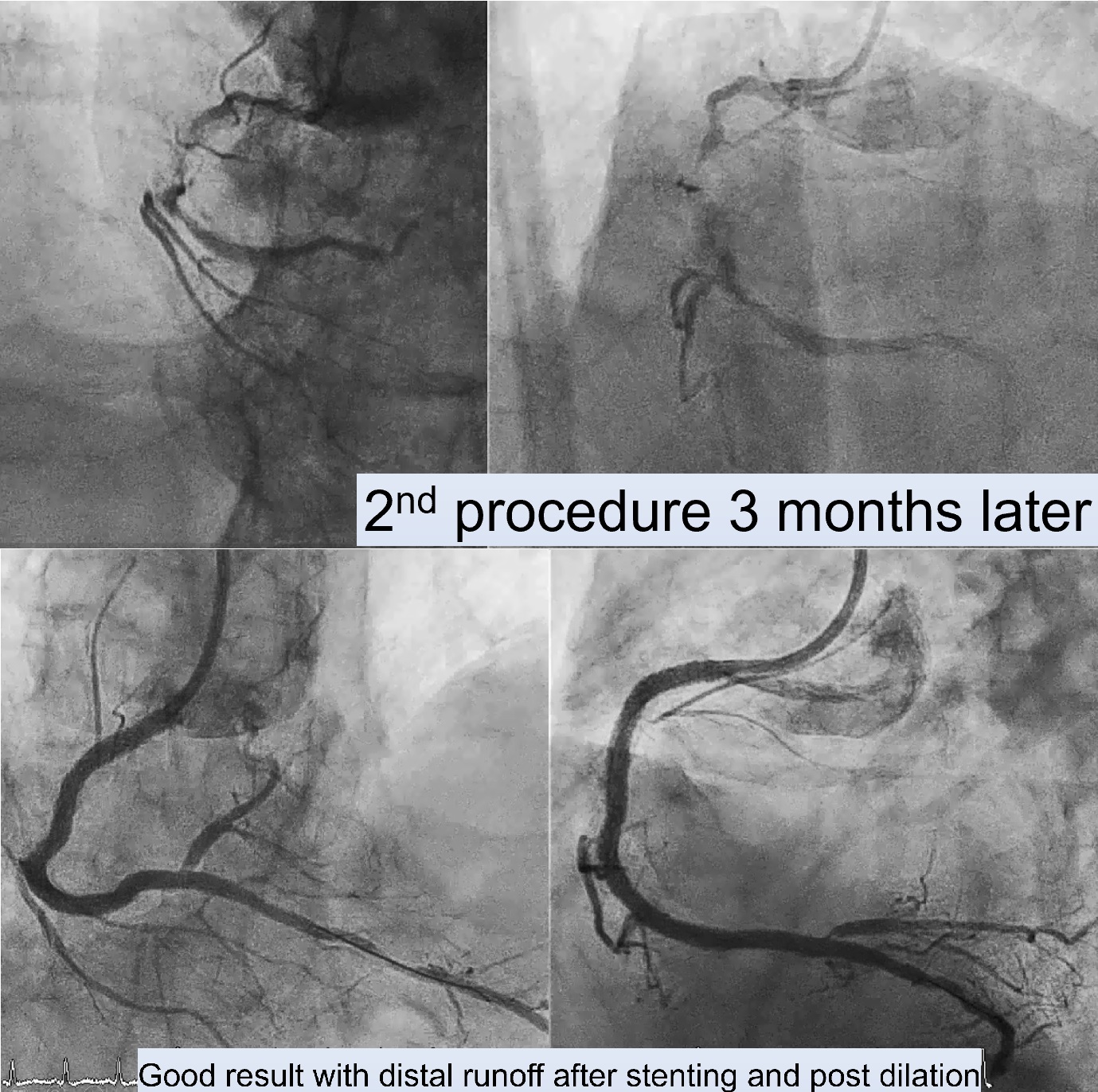
First Procedure: An antegrade approach was initially attempted with wire escalation strategies (using XTA, Fielder FC, Gaia I, II, III, Conquest pro in Cosair), but the wire entered a false lumen. Shift to parallel wire technique with Sasuke. The Gaia III wire eventually reached the distal true lumen. Balloon dilation was attempted, but the CTO segment remained undilatable. IVUS confirmed severe calcification, so a 1.25 mm rotational atherectomy (ROTA) burr was used, which led to mild improvement but still left an undilatable lesion. The procedure was paused because the patient could not tolerate lying flat for an extended time.Second Procedure was performed 3 months later. RCA still showed stenosis despite receiving collateral flow from LAD. Balloon dilation attempts were unsuccessful, necessitating a shift to a 1.75 mm ROTA burr for further plaque modification.After successful lesion modification, further preparation for stenting was performed, followed by the deployment of a 3.0 x 48 mm and a 3.5 x 48 mm drug-eluting stent (DES) in the RCA. Final IVUS confirmed adequate stent placement with good distal runoff. Additional stenting was performed in the LCx and LAD.
Case Summary
For patients who cannot tolerate prolonged procedures, particularly in complex CTO cases, a staged approach utilizing rotational atherectomy followed by drug-eluting balloon (DEB) application can be effective. The DEB provides interim drug delivery, reducing restenosis risk and allowing time for the patient to recover before the next procedure. This approach is especially beneficial for high-risk patients needing multiple sessions for complete revascularization.