
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-170
Drug-Coated Balloon (DCB) in Treatment of Calcified De Novo Left Anterior Descending Artery (LAD) Lesion
By Jin Kiang Cheng, Wee Pang Ng, Waye Young Lau, Heng Shee Kim
Presenter
Jin Kiang Cheng
Authors
Jin Kiang Cheng1, Wee Pang Ng1, Waye Young Lau1, Heng Shee Kim1
Affiliation
Sultanah Aminah Hospital, Malaysia1,
View Study Report
TCTAP C-170
Coronary - DES/BRS/DCB
Drug-Coated Balloon (DCB) in Treatment of Calcified De Novo Left Anterior Descending Artery (LAD) Lesion
Jin Kiang Cheng1, Wee Pang Ng1, Waye Young Lau1, Heng Shee Kim1
Sultanah Aminah Hospital, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 62-year-old Chinese gentleman with known history of T2DM and dyslipidemia presented in June2024 with acute anteroseptal STEMI, Killip Class I. He was successfully thrombolysis and discharged in stable condition on day 5 of treatment, with an outpatient angiogram scheduled for August 12, 2024. His ECG showed Q waves in V1 and V2, along with deep T-wave inversions in leads I, aVL, and V2 to V5. Cardiovascular examination revealed a dual rhythm with no murmurs.
Relevant Test Results Prior to Catheterization
An echocardiogram revealed good left ventricular function with anterior hypokinesia, an ejection fraction of 59%,normal chamber sizes, thin and well-coapted cardiac valves with no regurgitation or stenosis, and no evidence of thrombus or pericardial effusion. Key blood investigations included: HB 11.7 g/dL, creatinine 61 µmol/L, urea 3.9 mmol/L, total cholesterol 2.8 mmol/L, LDL 1.1 mmol/L, HDL 1.0 mmol/L, triglycerides 1.5 mmol/L, and random blood glucose 6.0 mmol/L
Relevant Catheterization Findings
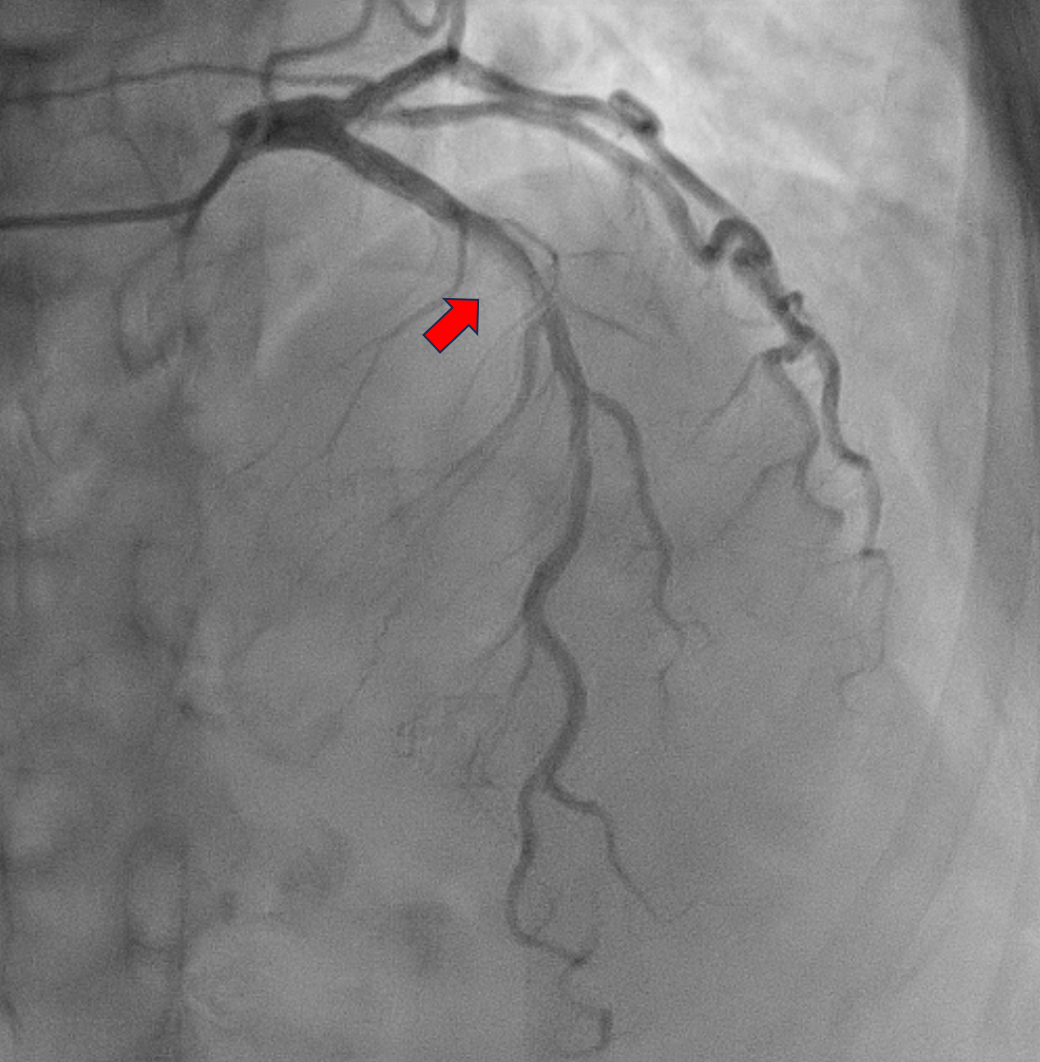
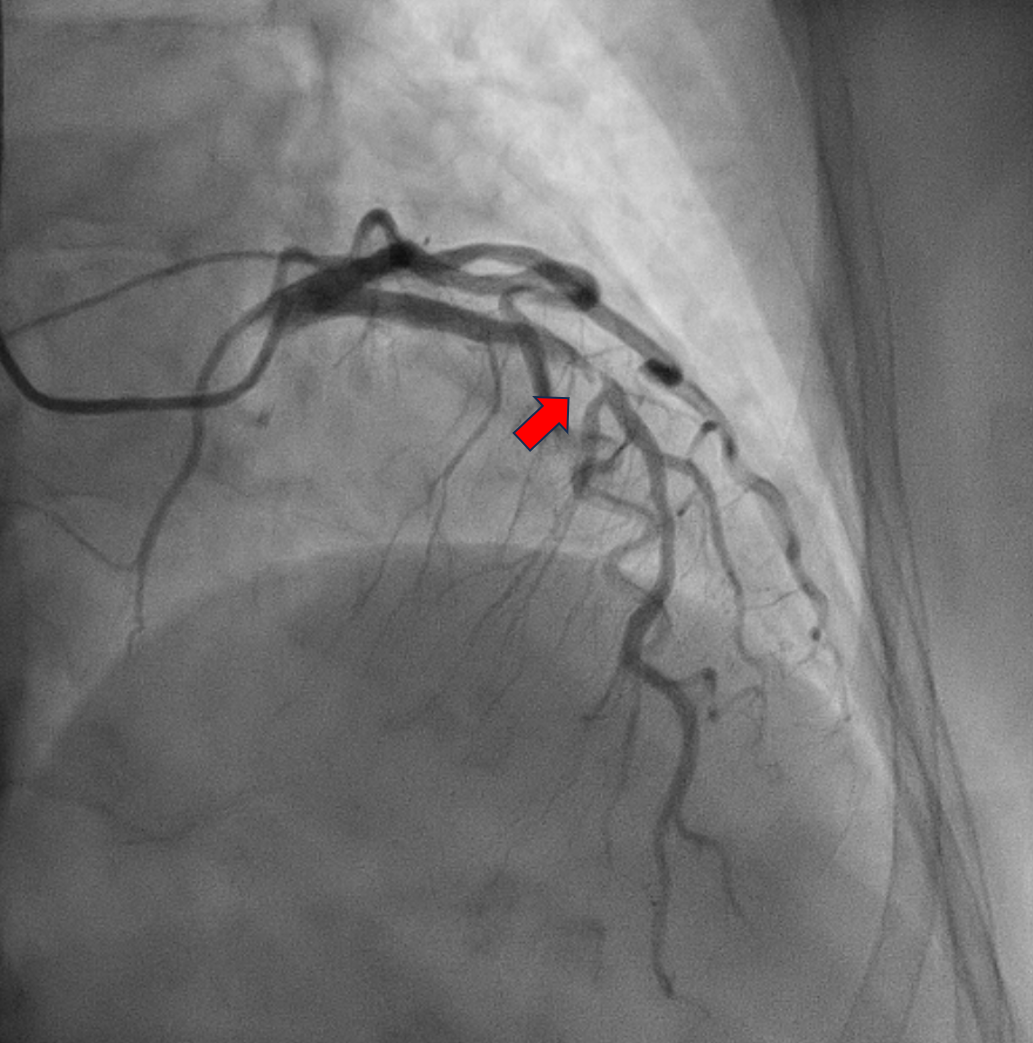
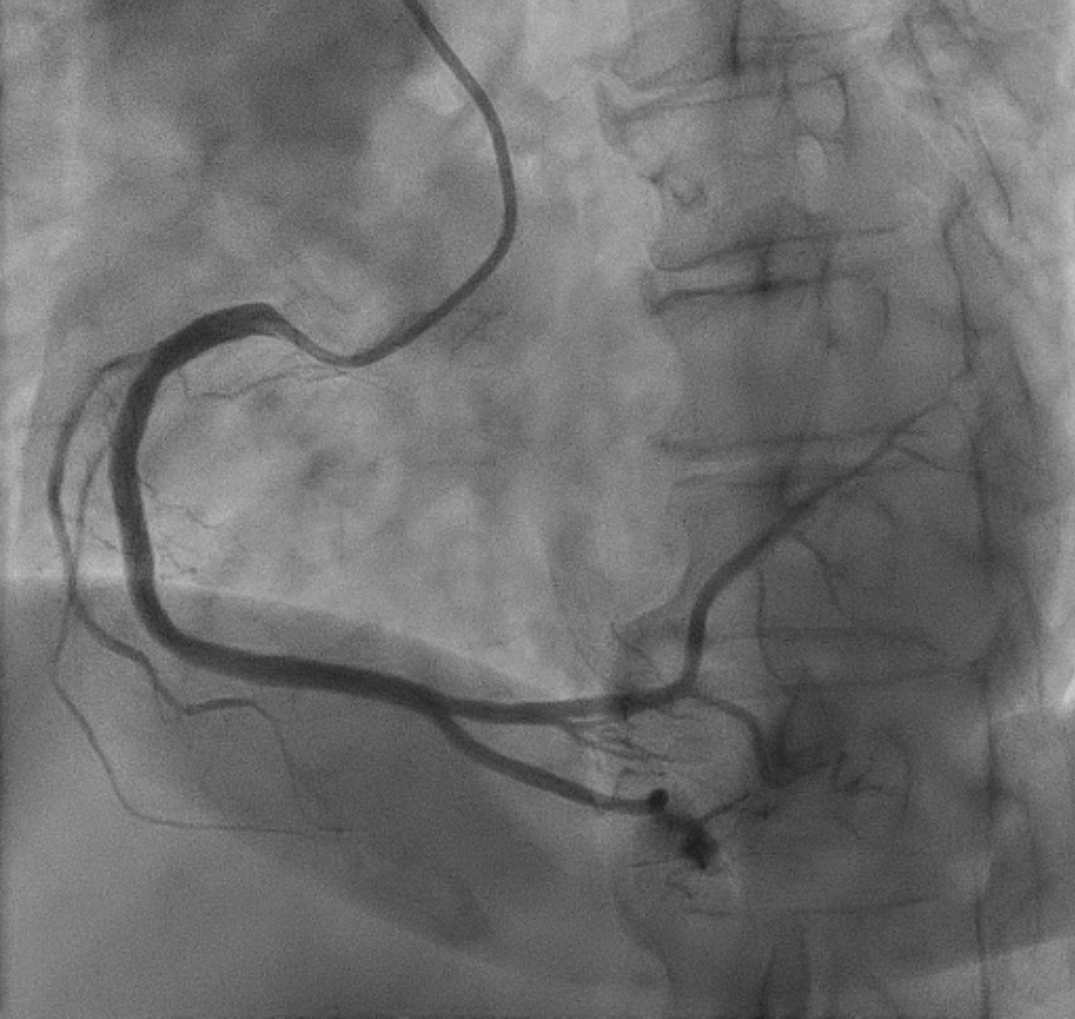
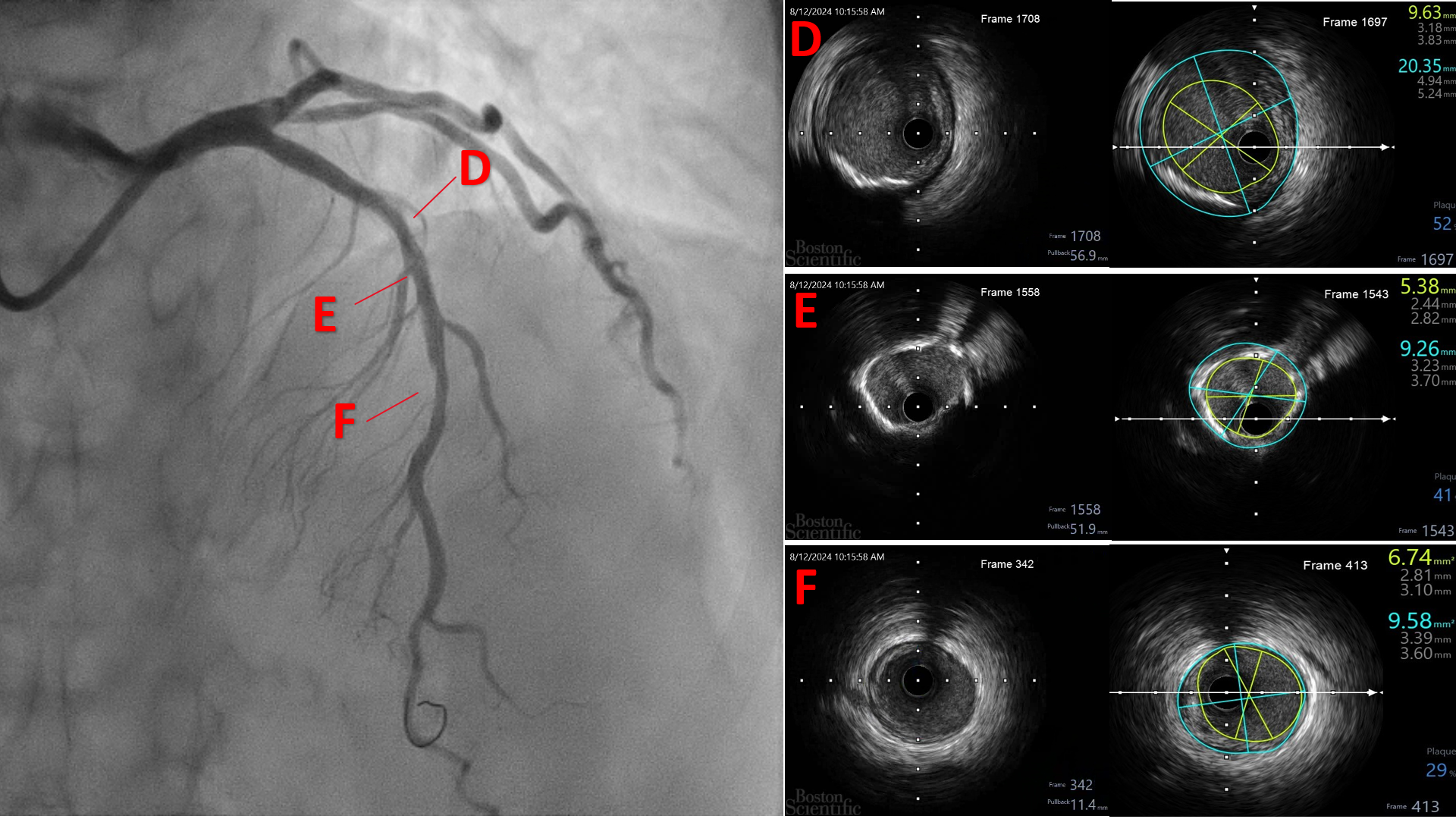
The patient was electively admitted for diagnostic coronary angiography on August 12, 2024, which revealed single-vessel disease (SVD) with 95% stenosis in the proximal to mid left anterior descending (LAD) artery. The LAD lesion is tight and calcified. His Left circumflex vessel and right coronary vessel are normal. We proceeded with percutaneous coronary intervention (PCI) to the LAD with DCB only strategy.
Interventional Management
Procedural Step
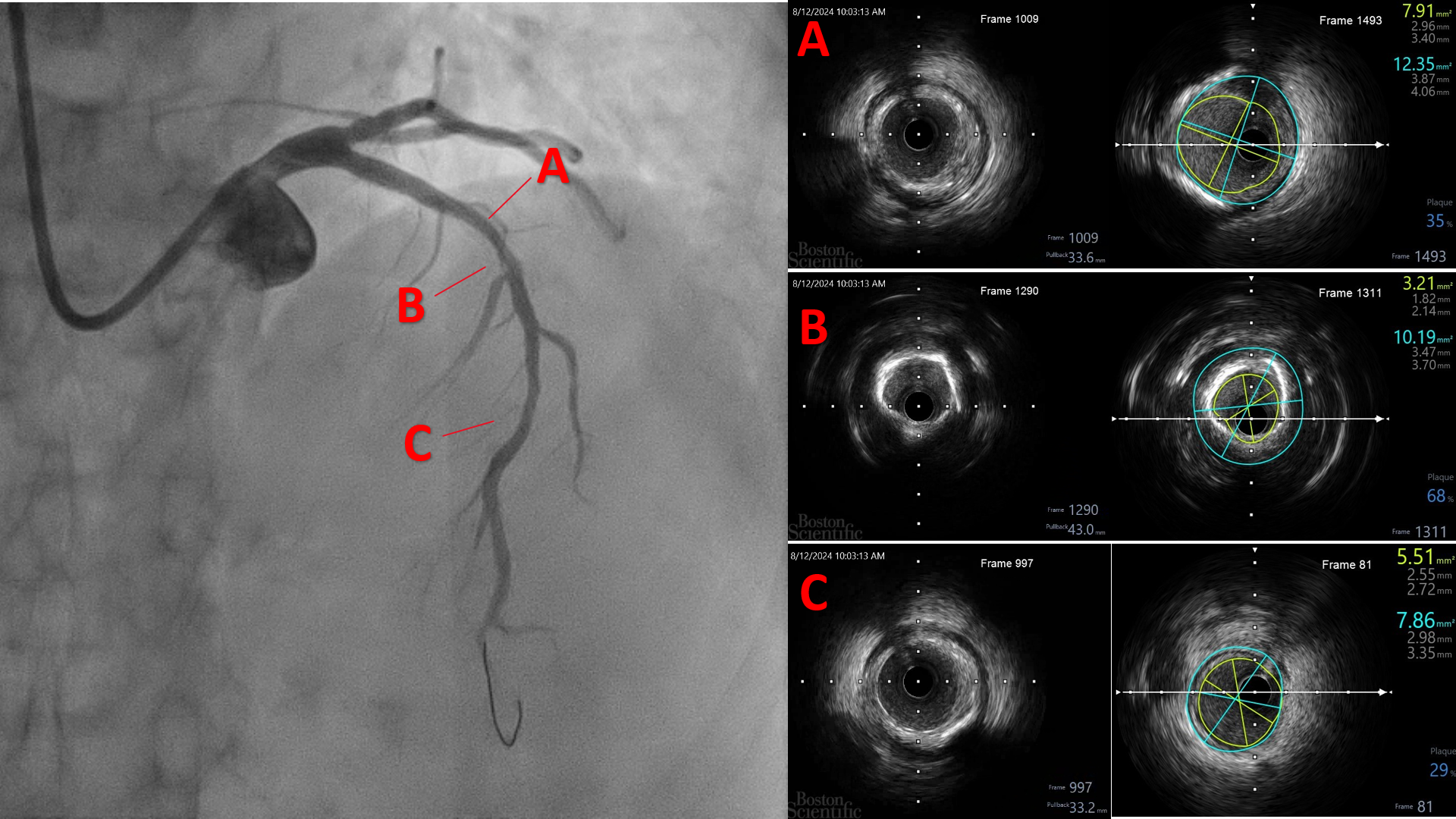
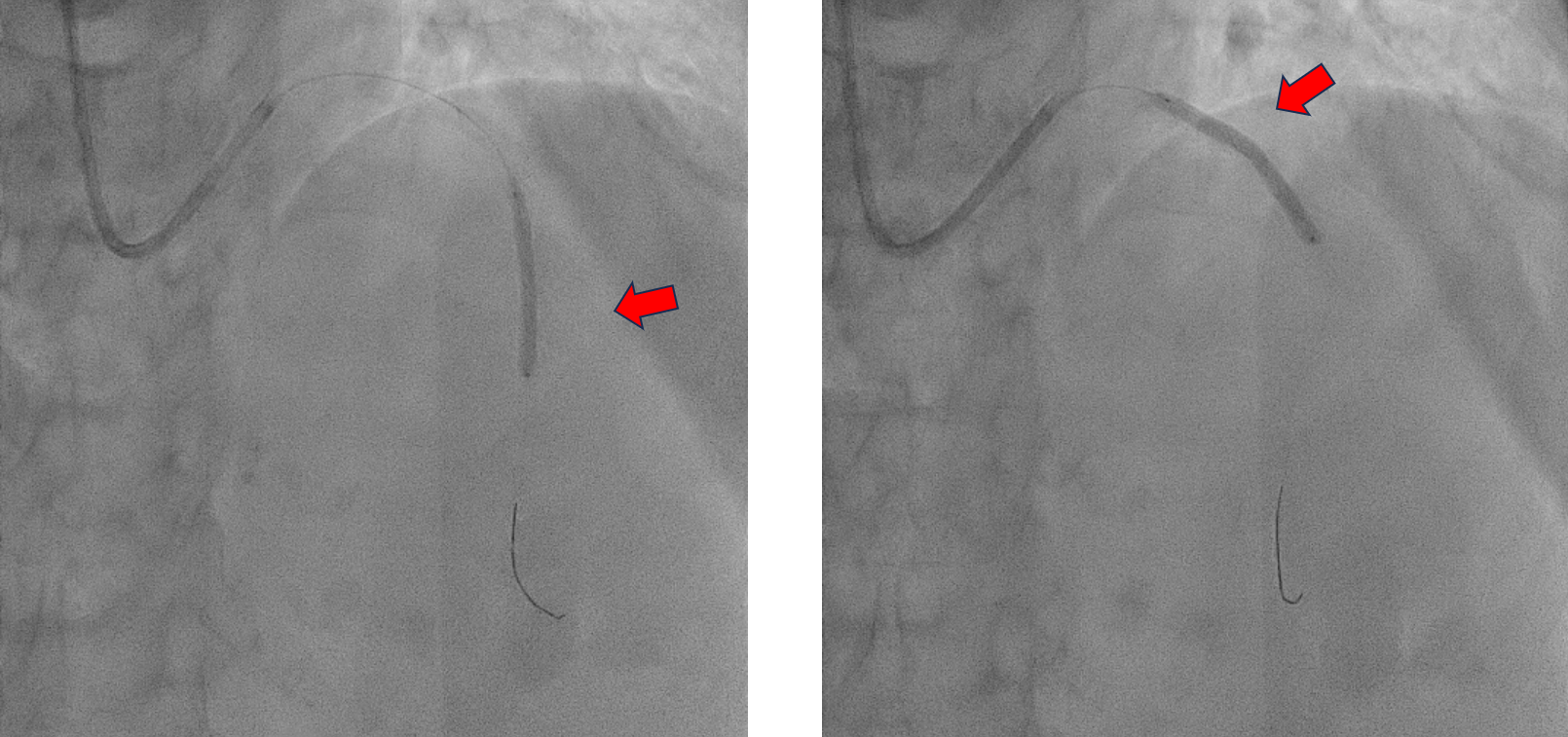
The procedure was performed using a 7 Fr right radial approach. A total of 6000 units of intracoronary heparin and 300 mg of oral clopidogrel were administered. The left coronary system was engaged with a 7 Fr extra-backup (EBU) 3.5 mm guiding catheter, and the lesion was successfully crossed with a Run-through floppy wire extending to the distal LAD. Pre-dilation was performed with a 2.0 mm x 15 mm Genoss balloon, inflated to 16 atm. Intravascular ultrasound (IVUS) imaging revealed 360-degree superficial calcium at the tight LAD lesion, a vessel diameter under 3.5 mm, and a calcium score of 2. The mid-LAD measured 3.0 mm and the proximal LAD measured 4.0 mm. Pre-dilation was performed in the mid-LAD using a 3.0 mm x 16 mm Genoss non-compliant (NC) balloon, and in the proximal LAD with a 3.5 mm x 20 mm NC Emerge balloon, both inflated to 16 atm. Post-pre-dilation IVUS imaging showed cracking of the superficial calcium with vessel expansion to 3.0 mm. Subsequently, drug-coated balloon (DCB) angioplasty was performed with a 3.0 mm x 30 mm Magic Touch DCB in the mid-LAD and a 3.5 mm x 35 mm Magic Touch DCB in the proximal LAD. Final angiography demonstrated a non-flow-limiting Type A dissection with less than 30% recoil, and the procedure was successfully concluded.
Case Summary
Superficial calcium lesions can be effectively prepared or fractured using a NC balloon. The decision to use an NC balloon is based on its ability to achieve adequate lesion preparation with minimal risk of severe dissection, which is particularly important in calcified lesions. Intravascular ultrasound (IVUS) plays a pivotal role in the assessment of calcified lesions by providing detailed insights into the extent and distribution of calcium, determining the precise vessel size, and guiding appropriate treatment strategies. DCB therapy, when preceded by adequate lesion preparation, has proven to be a safe and effective strategy for both de novo calcified and non-calcified lesions.