
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-204
Transfemoral Transcatheter Aortic Valve Replacement for a Severe Aortic Regurgitation With Stanford Type B Aortic Dissection: A Case Report
By Shangdian Liu
Presenter
Shangdian Liu
Authors
Shangdian Liu1
Affiliation
Shenzhen Hospital of Guangdong Provincial People's Hospital, China1,
View Study Report
TCTAP C-204
Structural - Aortic Valve Intervention - Complex TAVR
Transfemoral Transcatheter Aortic Valve Replacement for a Severe Aortic Regurgitation With Stanford Type B Aortic Dissection: A Case Report
Shangdian Liu1
Shenzhen Hospital of Guangdong Provincial People's Hospital, China1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
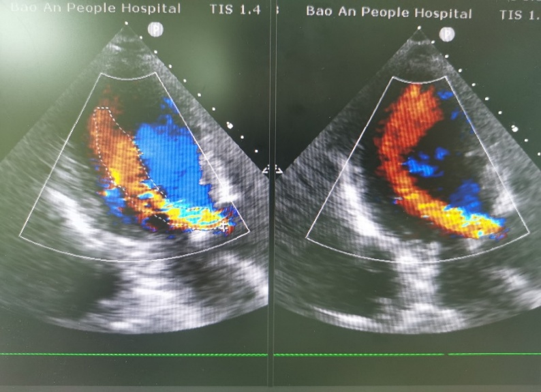
Patient Demographics:man, 82-year-old Chief Complaint:tachypnea for 2 yearsPast Medical History: hypertension 20 years;Stanford type B aortic dissection 2 yearsPersonal History: denied smoking and alcohol historyPhysical examination:Clear respiratory sounds are present in both lungs, with no audible dry or wet rales.A grade 3/6 diastolic murmurs can be heard in the aortic valve area.TEE before surgery showed severe AR , regurgitation area was about 8.3 cm2, Ascending aorta diameter was 33 mm.

Relevant Test Results Prior to Catheterization
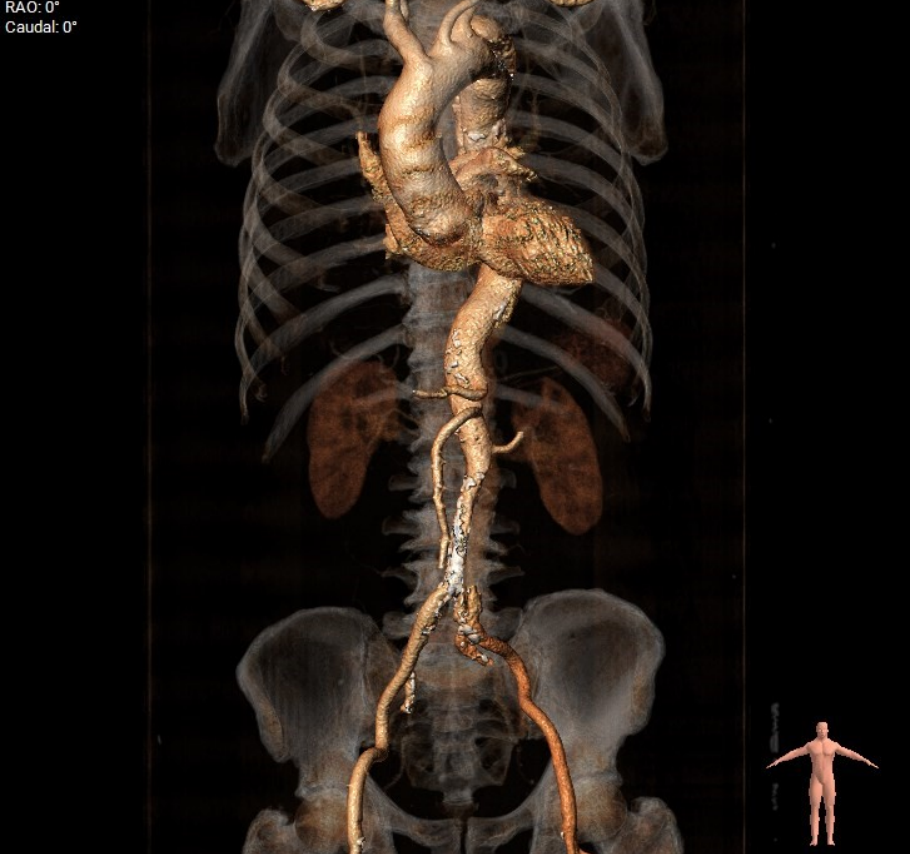
Computed tomography angiography (CTA) measurements showed significant dilation of the descending thoracic aorta to approximately 38 mm. The dissection began at the distal end of the left subclavian artery (LSA) and extended through the descending aorta to the left common iliac artery (LCIA).

Relevant Catheterization Findings
Interventional Management
Procedural Step
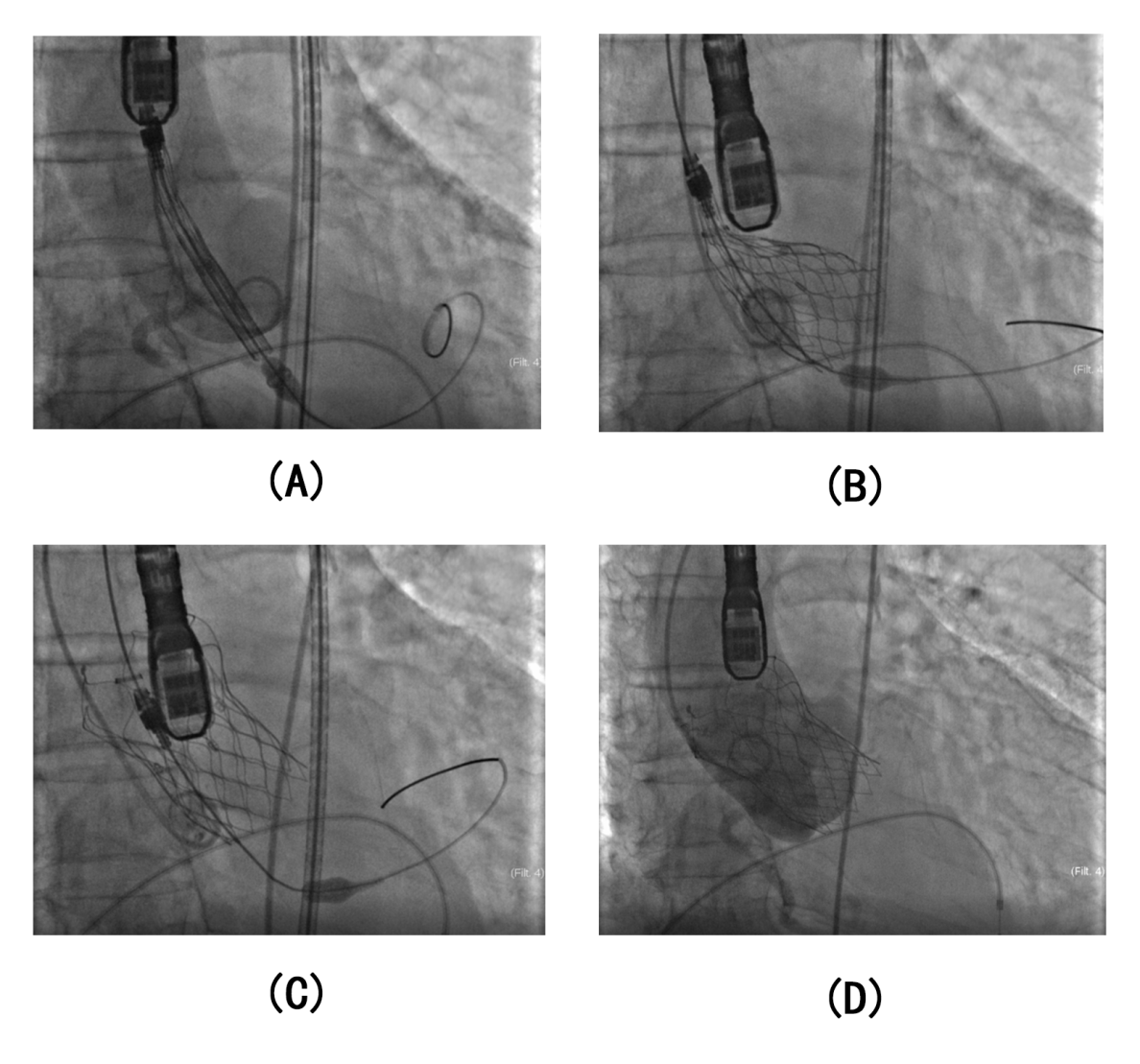
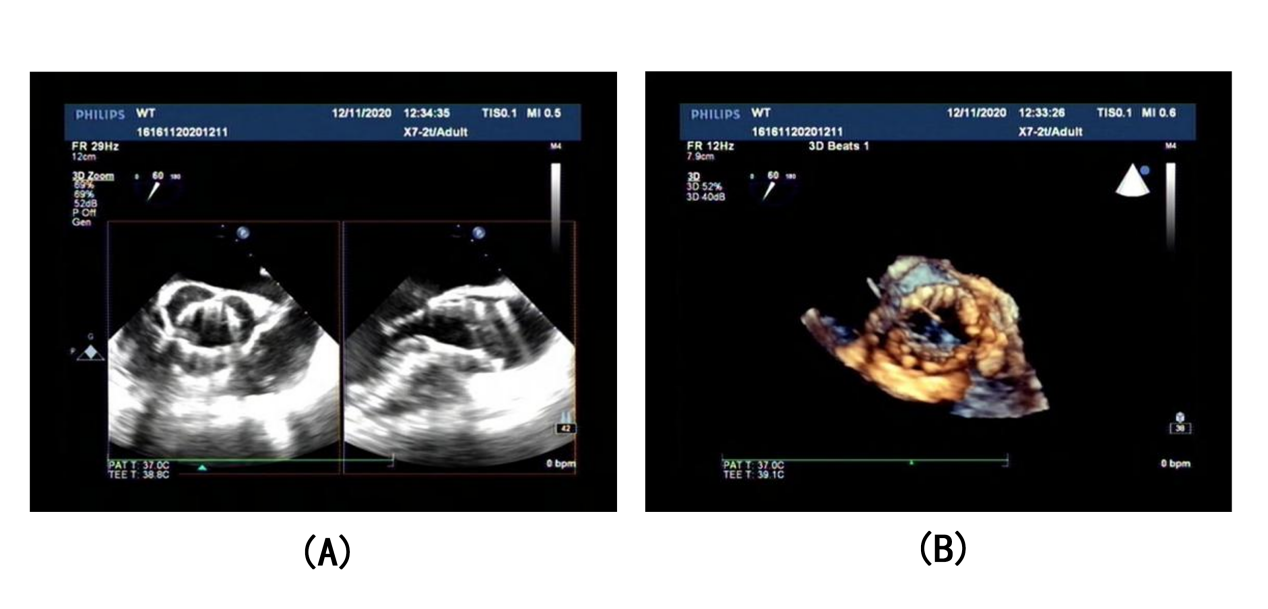
TAVR was performed under general anesthesia (Figure 3). At first, we sent the pacing electrode to the apex of right ventricular via one side of the femoral vein and tested whether the pacing was working properly. Then we delivered into a pig-tail centimeter sizing catheter to nadir of non-coronary sinus through one side of the femoral artery. The 18-Fr long sheath was inserted from the other side of the femoral artery to the descending aorta, and the super stiff guidewire was sent across the aortic valve into the left ventricular. Angiography by this route showed the aortic valve was tricuspid and had severe regurgitation. Adjusted the angle so that the nadir of three sinuses were shown on common flat. In 3D TEE, we accurately measured the diameter of left ventricular outflow tract was 23 mm, aortic annulus diameter was 25 mm, sinus diameter was 46 mm, diameter of sinus canal junction was 38mm and the diameter of ascending aorta was 39 mm. The results of preoperative CTA assessment were further refined. Combined with preoperative CT estimation results and TEE results during surgery, the 29M VenusA delivery system was selected to carefully fed along the super stiff guidewire. After confirming the position, rapid ventricular pacing was undertaken that controlled the heart rate to 180 beats/min, and the systolic blood pressure was adjusted to 40 mmHg. The prosthesis was released while cardiac output completely abolished (Figure 4).
Case Summary
As the population continues to age, there will be an increasing number of older patients with complex aortic diseases. Many cases have demonstrated the application of TAVR under special conditions.Multidetector row computed tomography can provide accurate measurement of the annulus of the aortic valve both in pre-TAVR and intra-TAVR, which has emerged as the gold standard in procedure. Although our patient had TBAD and there was a risk of aortic rupture or retrograde expansion of the dissection, we still chose the TF approach for surgery after careful consideration. We used long sheath to minimise contact with the false lumen.TAVR is an alternative treatment for patients with AR.