
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-004
A Challenging Case Report of PCI With Ischemic Osborn Wave and POT-PUFF Sign Guided Revascularization in TVD s/p PCI to LCx, RCA
By Wichid Thirakraisri, Wittawat Wattanasiriporn
Presenter
Wichid Thirakraisri
Authors
Wichid Thirakraisri1, Wittawat Wattanasiriporn1
Affiliation
Rajavithi Hospital, Thailand1,
View Study Report
TCTAP C-004
Coronary - ACS/AMI
A Challenging Case Report of PCI With Ischemic Osborn Wave and POT-PUFF Sign Guided Revascularization in TVD s/p PCI to LCx, RCA
Wichid Thirakraisri1, Wittawat Wattanasiriporn1
Rajavithi Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A Thai 60 year-old man with T2DM, HT, CKDIII, history of NSTEMI with CHF. The CAG finding in 2016 was TVD S/P PCI to RCA with 02DES, LCX with 02DES. He presented to emergency department with acute chest pain 1 day. V/S: BT 36.9 C BP 105/62 mmHg PR 64/min RR 16/min. Heart: normal S1,S2. no murmur, Lung: clear.
Relevant Test Results Prior to Catheterization
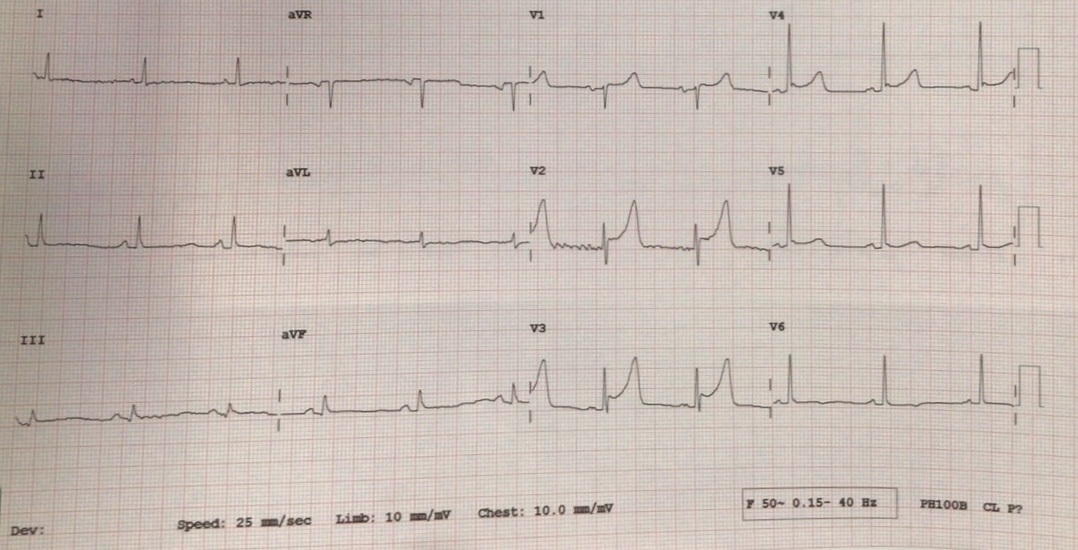
EKG showed Osborn waves in V3-V5 during chest pain. Echocardiogram showed LVEF 47%, mild anterior-anteroseptal wall hypokinesia, no significant valvular heart disease. The serum Troponin I was 12.0 ng/L on admission.
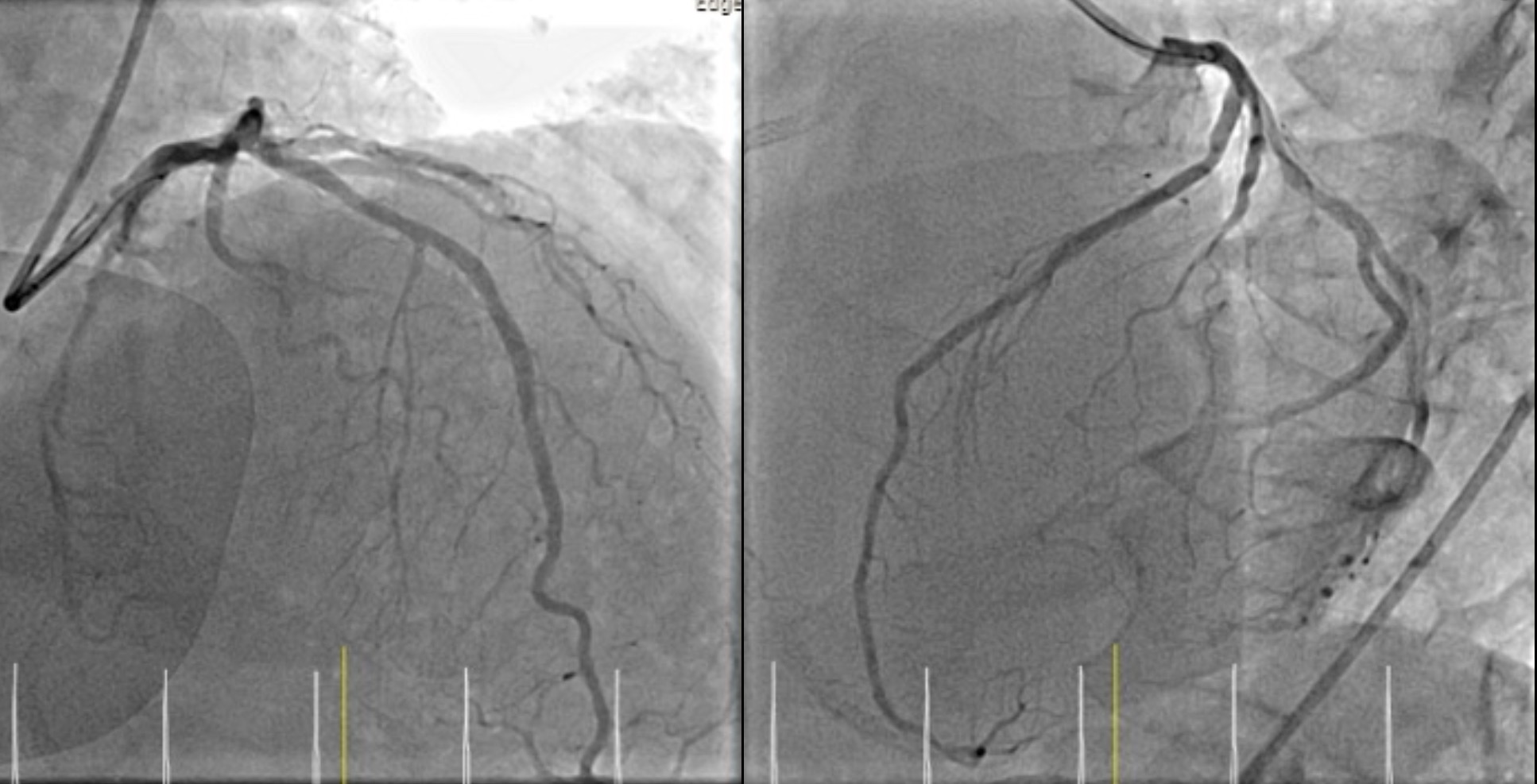
Relevant Catheterization Findings
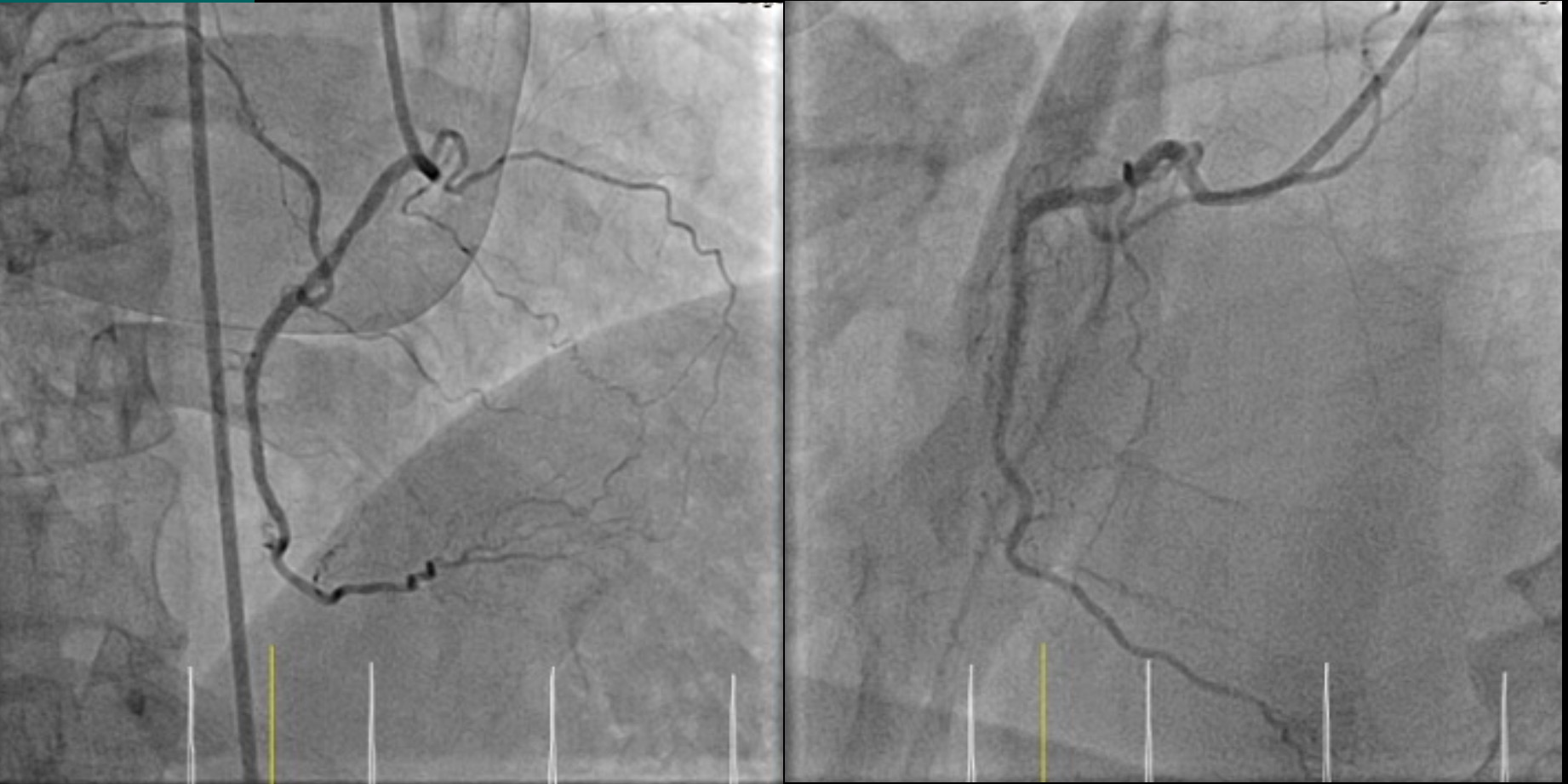
CAG was performed via right femoral approach with JL6/4, JR 6/4 diagnostic catheter. The finding show 50-60% stenosis mid LAD, 90-95% stenosis DG1, 75-80% stenosis pLCX, patent LCX, RCA stent.
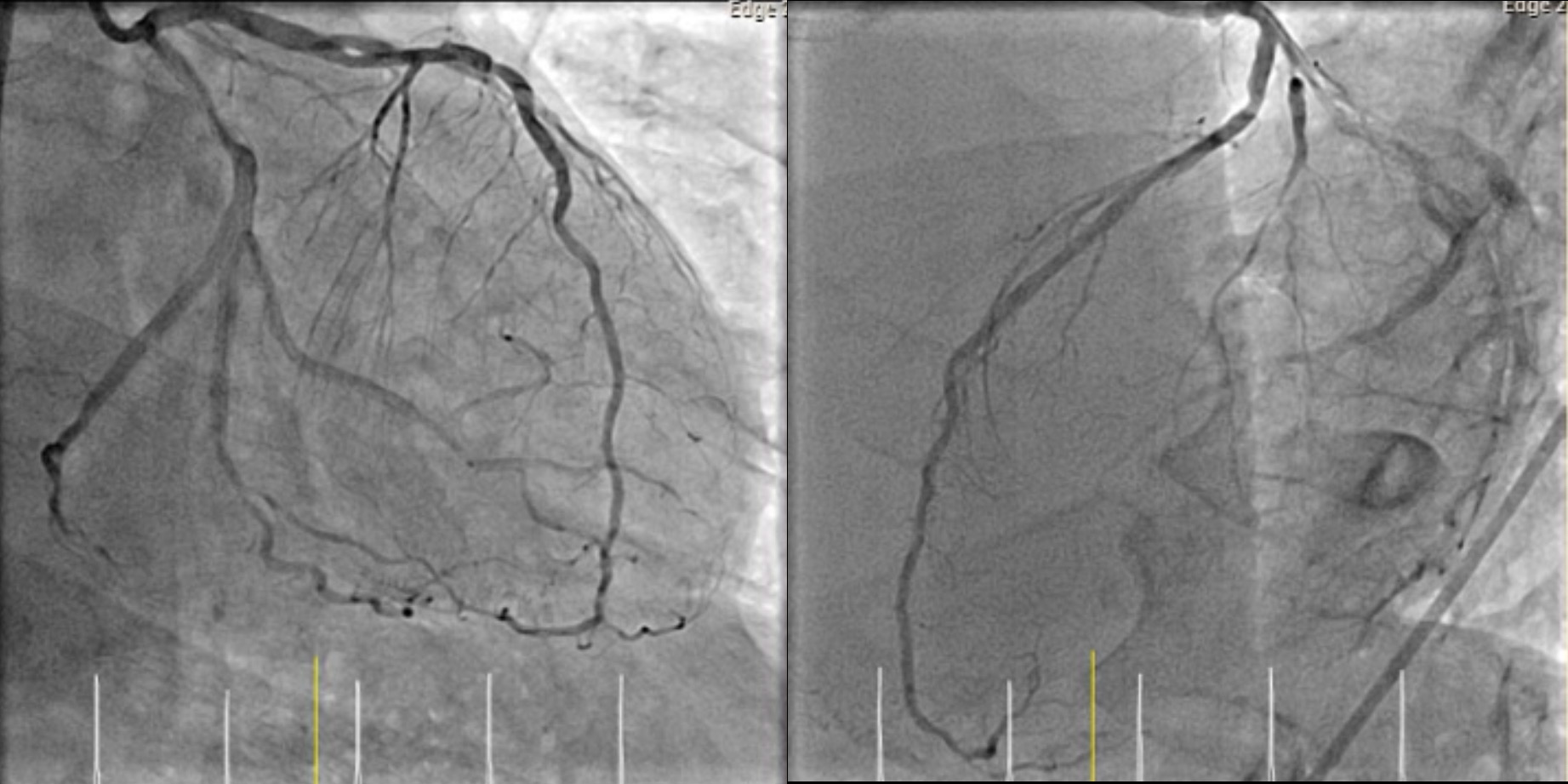
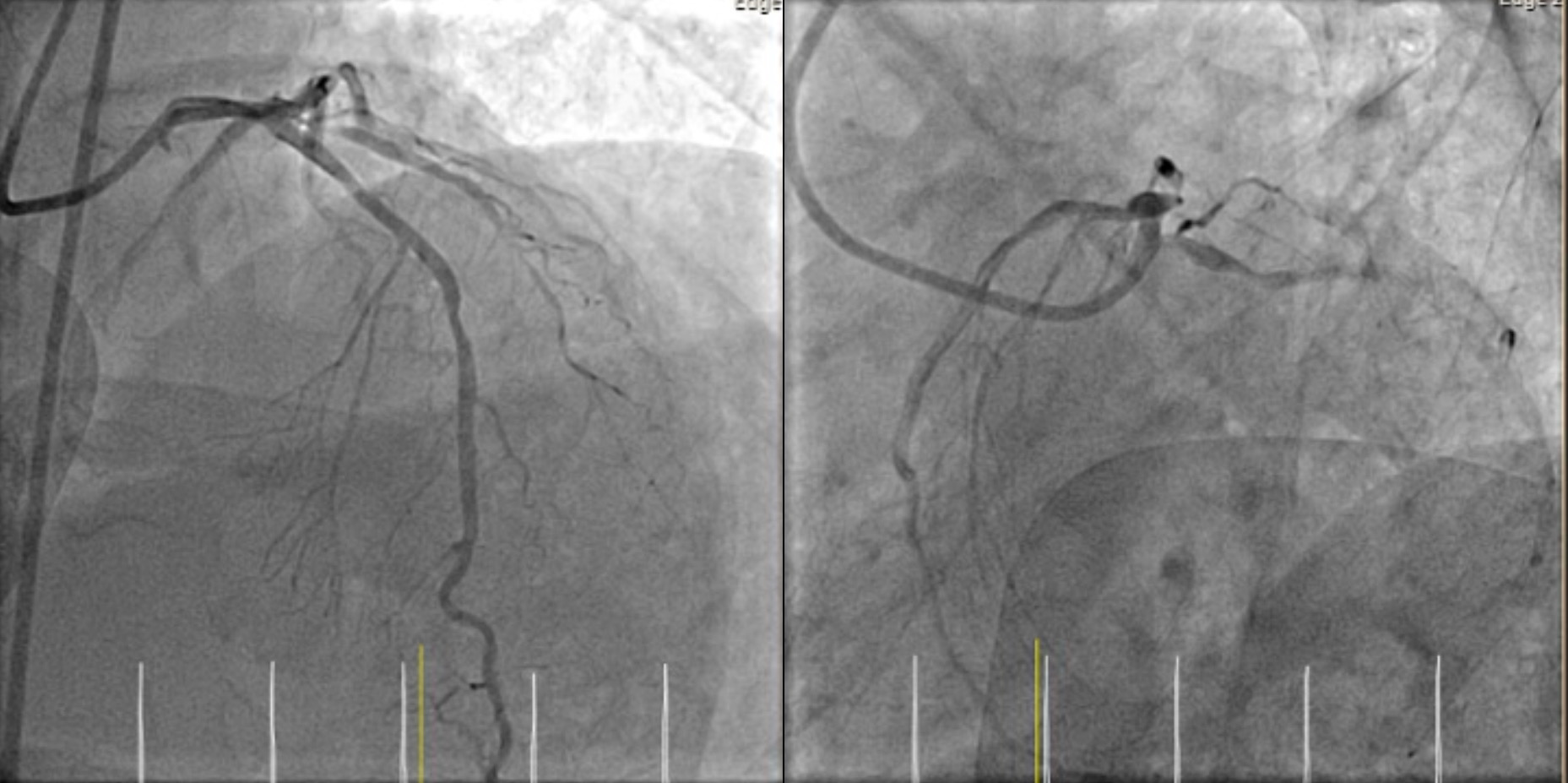
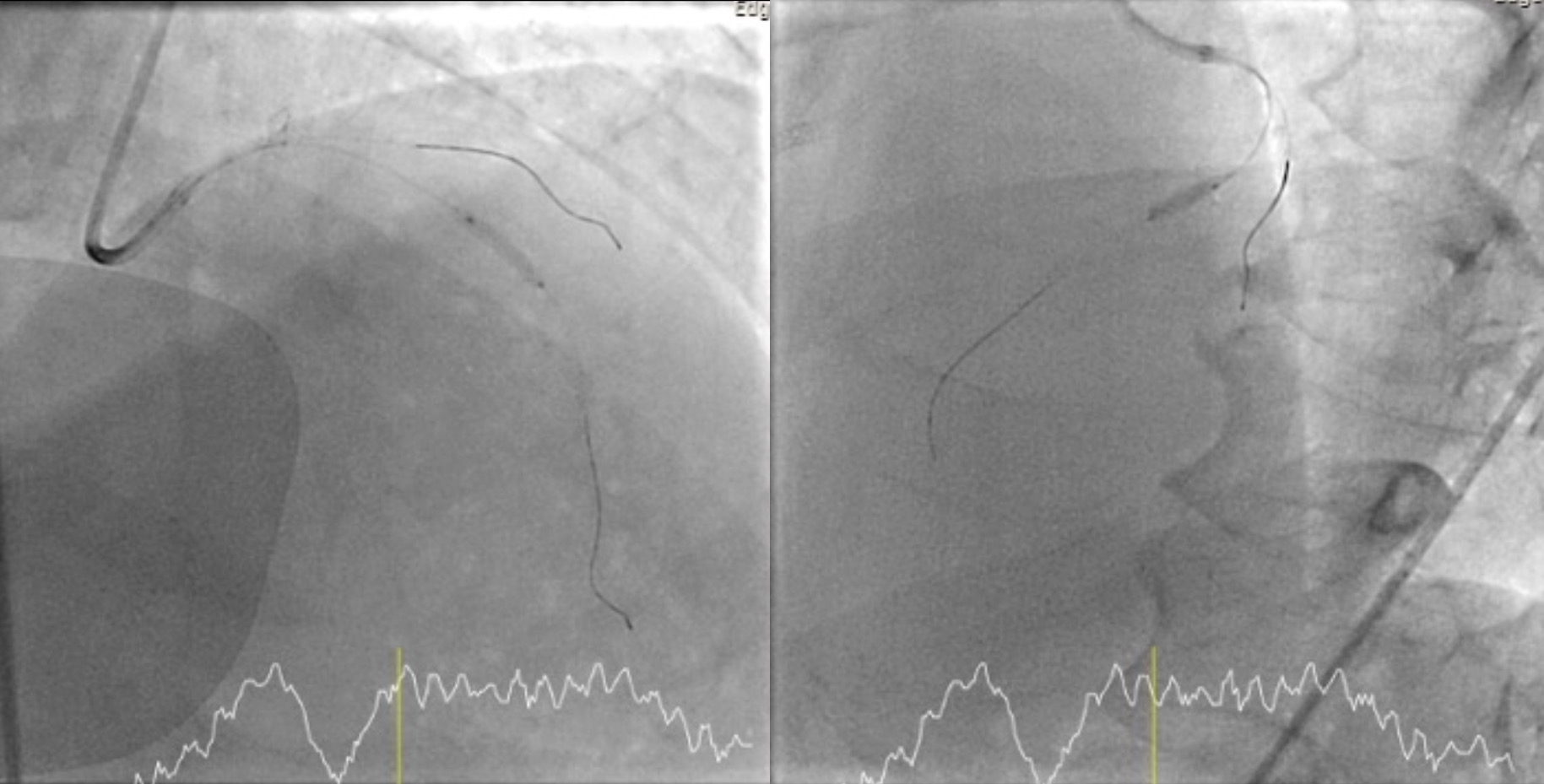
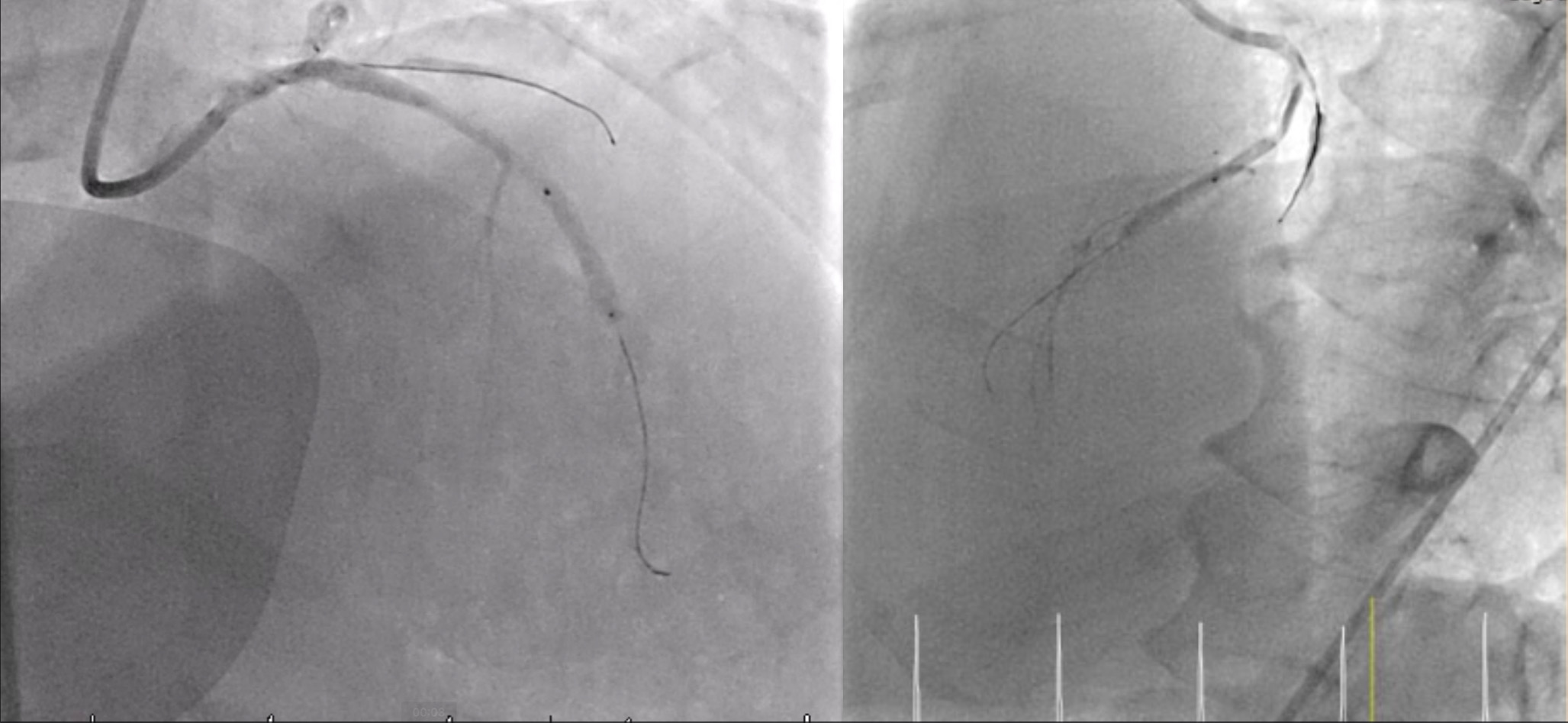
Interventional Management
Procedural Step
CAG was performed via right femoral approach with JL6/4, JR 6/4 diagnostic catheter show 50-60% stenosis mid LAD, 90-95% stenosis DG1, 30-40% stenosis pLCX, patent LCX and RCA stent.PCI with JL 6/4. PCI to LAD. GD: JL6/4. Turntrac to LAD. DG. SC balloon 2.5x12 mm inflated mLAD upto 14 atm. Biolimus eluting stent 2.75x14 mm deployed mid LAD 12 atm with POT-PUFF sign technique. NC balloon 2.75 x 12 mm postdilated upto 16 atm. SC balloon POBA DG1 upto 12 atm. The final angiogram was acceptable result.
Case Summary
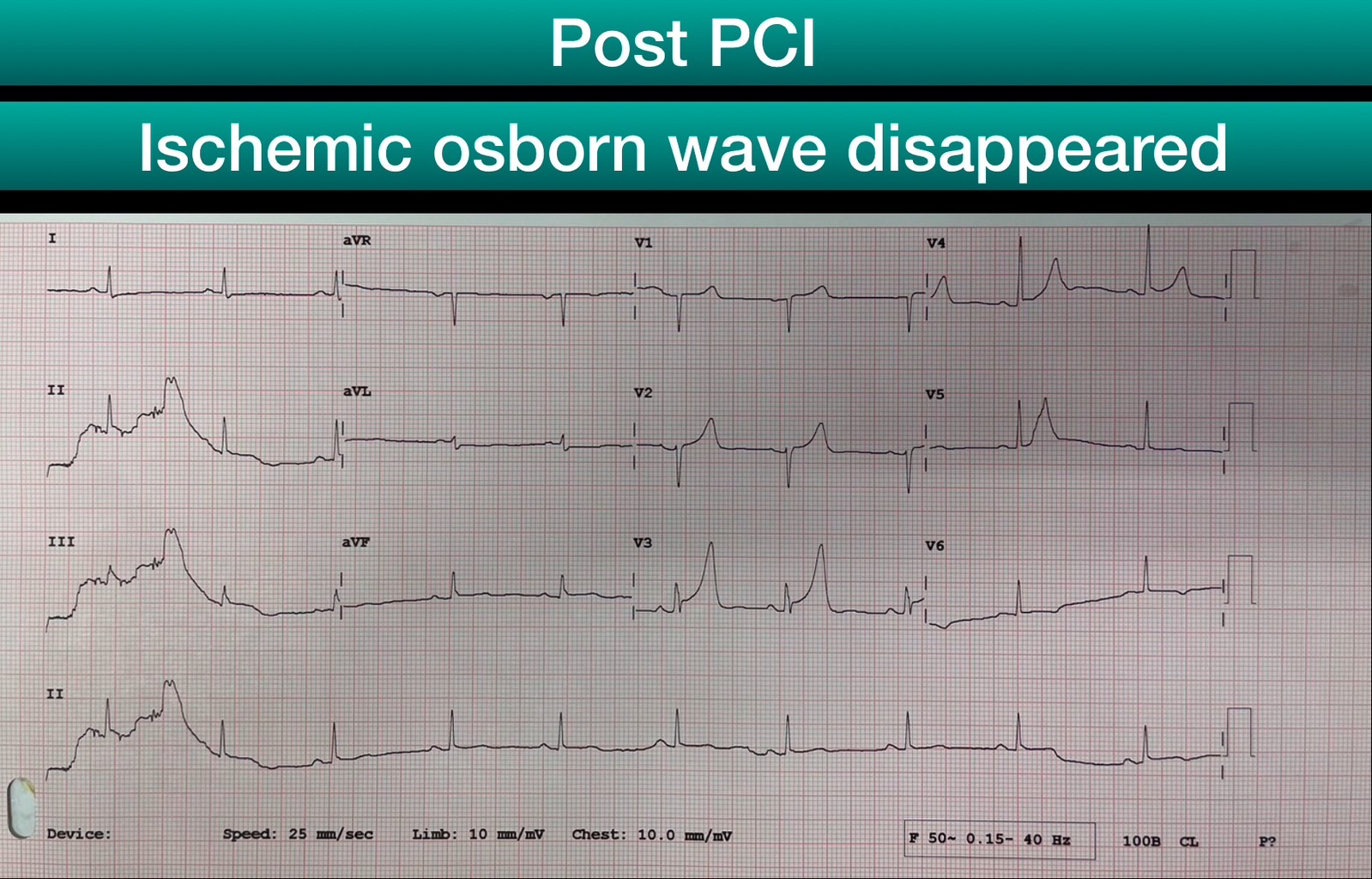
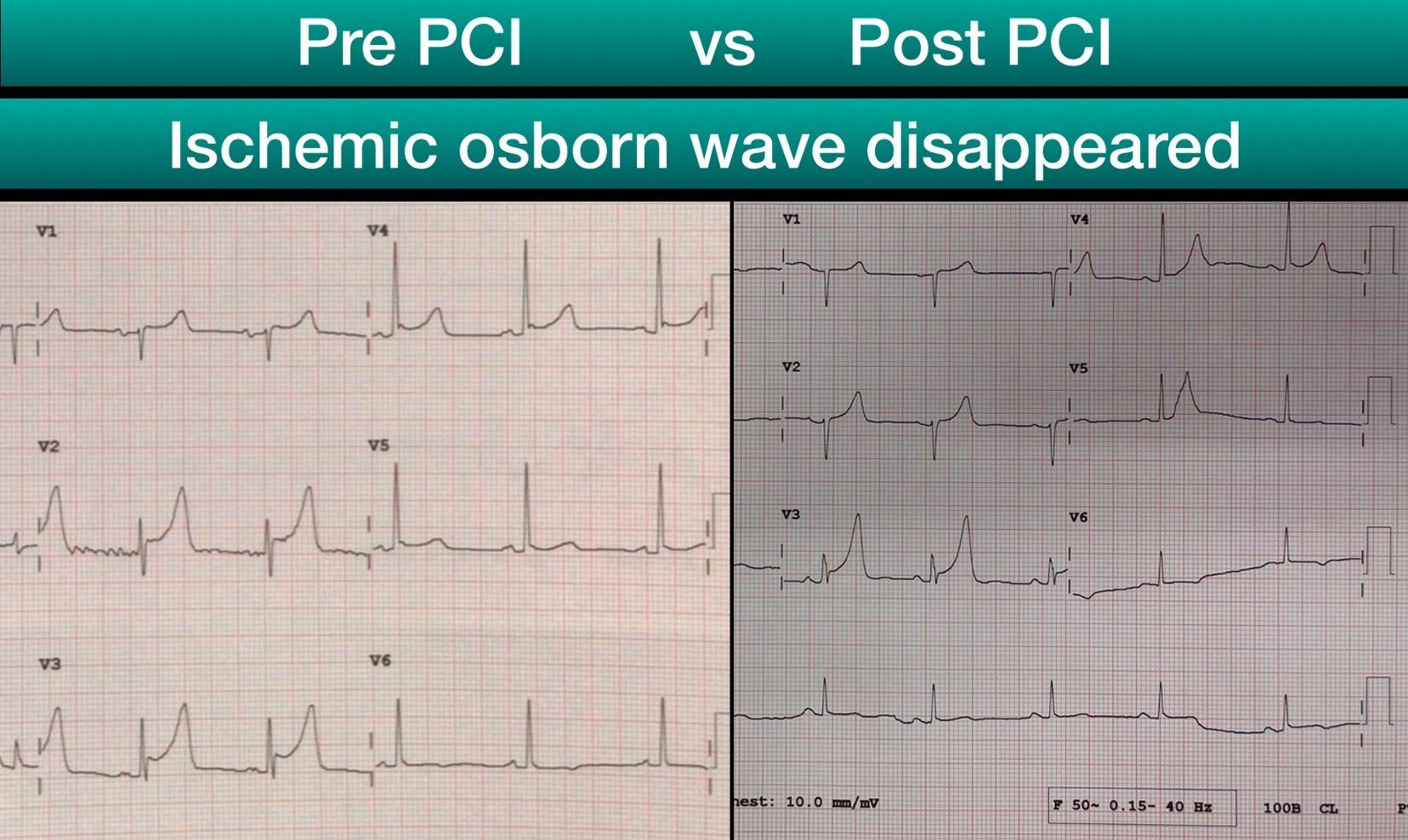
1. The Osborn waves is not pathognomonic of hypothermia, and it can be seen in a number of other condition such as acute myocardial ischemia, idiopathic ventricular fibrillation, clinical hypercalcemia, Brugada syndrome. 2. Ischemic Osborn wave would be useful in localizing culprit artery. 3. Recognition of the ischemic Osborn wave is important because it is associated with an acute ischemic process and carries a potential risk of developing phase II reentry and subsequent ventricular fibrillation(VF), thereby facilitating the selection of the most effective therapeutic approaches.4. The "POT-PUFF sign" is a potentially useful alternative for detecting stent malapposition during PCI.