
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-113
Optimal Use of Intracoronary Imaging for Recurrent Stent Failure Management With a Drug Coated Balloon
By Raja Ramesh Nukavarapu, Ramesh Babu Pothineni
Presenter
Raja Ramesh Nukavarapu
Authors
Raja Ramesh Nukavarapu1, Ramesh Babu Pothineni1
Affiliation
Aster Ramesh Hospitals, India1,
View Study Report
TCTAP C-113
Coronary - Complex PCI - In-Stent Restenosis
Optimal Use of Intracoronary Imaging for Recurrent Stent Failure Management With a Drug Coated Balloon
Raja Ramesh Nukavarapu1, Ramesh Babu Pothineni1
Aster Ramesh Hospitals, India1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
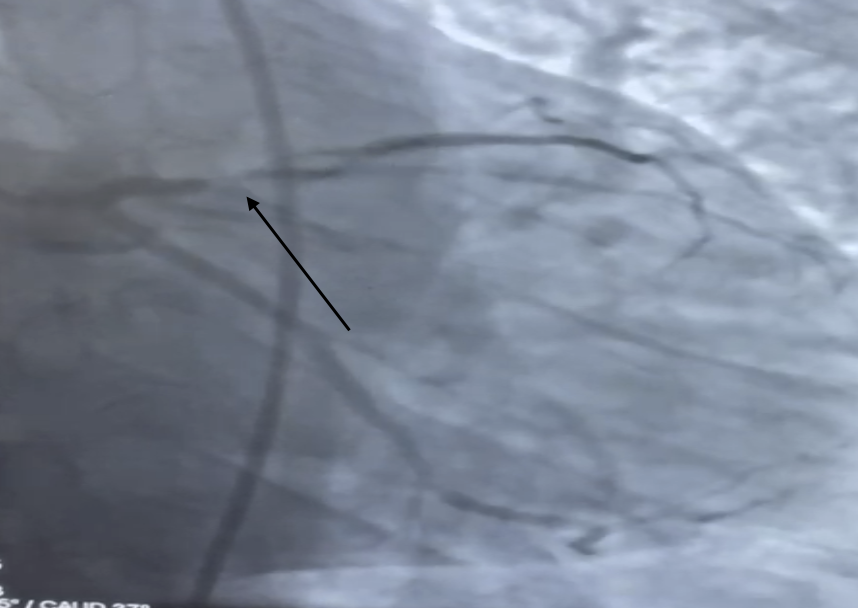
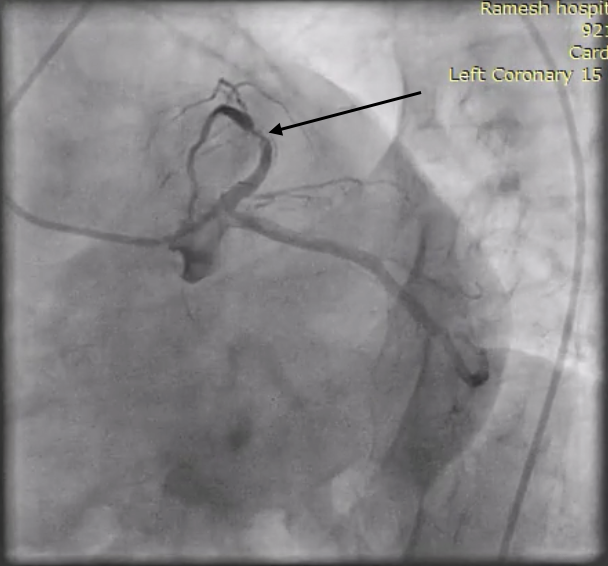
58 years male, diabetic and hypertensive had an episode of unstable angina and underwent stenting to LAD( left anterior descending artery) with everolimus DES( drug eluting stent) under angiographic guidance. Two month later had an episode of NSTEMI(non ST myocardial infarction), coronary angiogram showed mid to distal instent restenosis(ISR) with thrombus. This episode was treated PCI (percutaneous coronary intervention) with a 2.75 X 28 mm everolimus DES in LAD overlapping the previous stent.
Relevant Test Results Prior to Catheterization
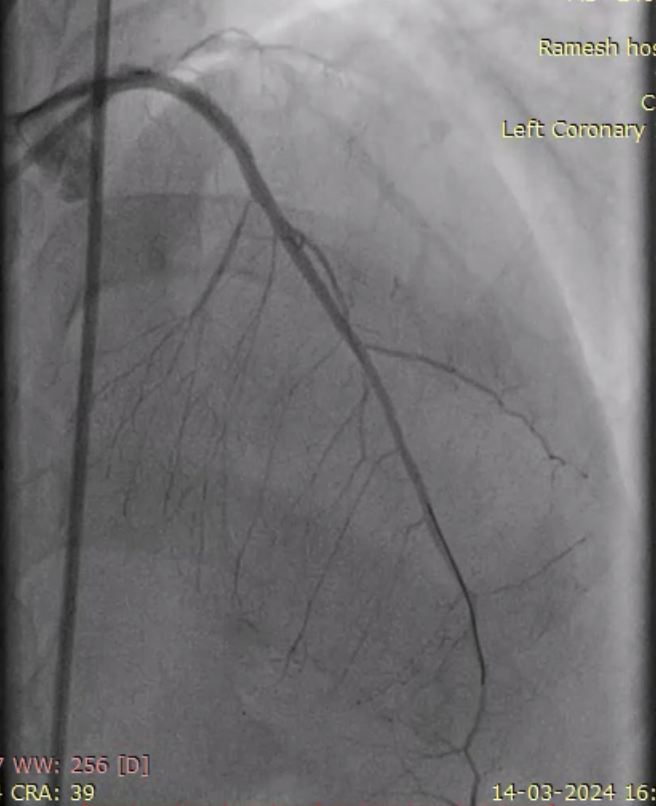
Three months after the second episode of stenting he again presented with NSTEMI and LV dysfunction. Coronary angiogram showed ISR at the overlap part of stents extending distally with TIMI II flow.
Relevant Catheterization Findings
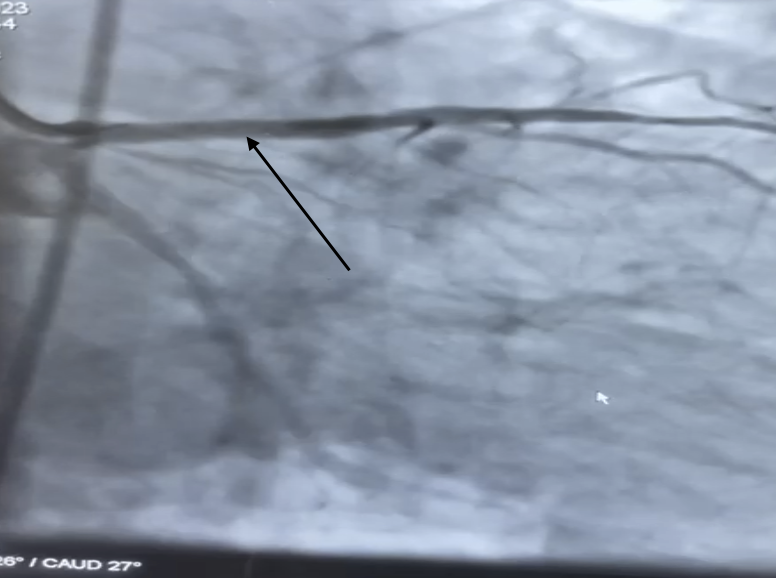
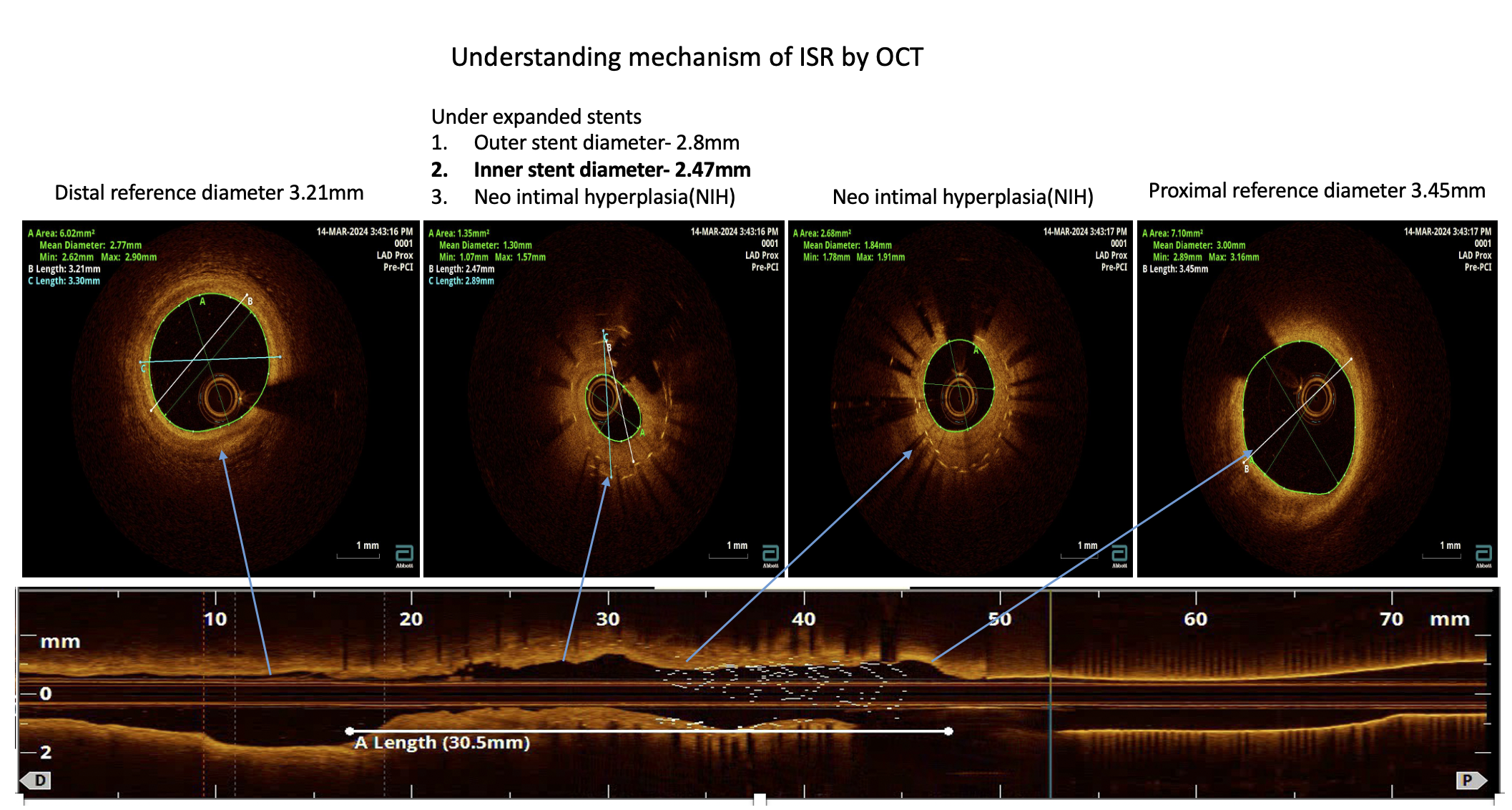
The lesion was wired with Run through wire and dilated with 2 mm NC balloon to facilitate the passage of OCT catheter as there was only TIMI II flow. OCT run was done to LAD by dragonfly opstar catheter for understanding the mechanism of ISR and to plan the management. OCT showed under expanded previous stents with neo intimal hyperplasia.
Interventional Management
Procedural Step
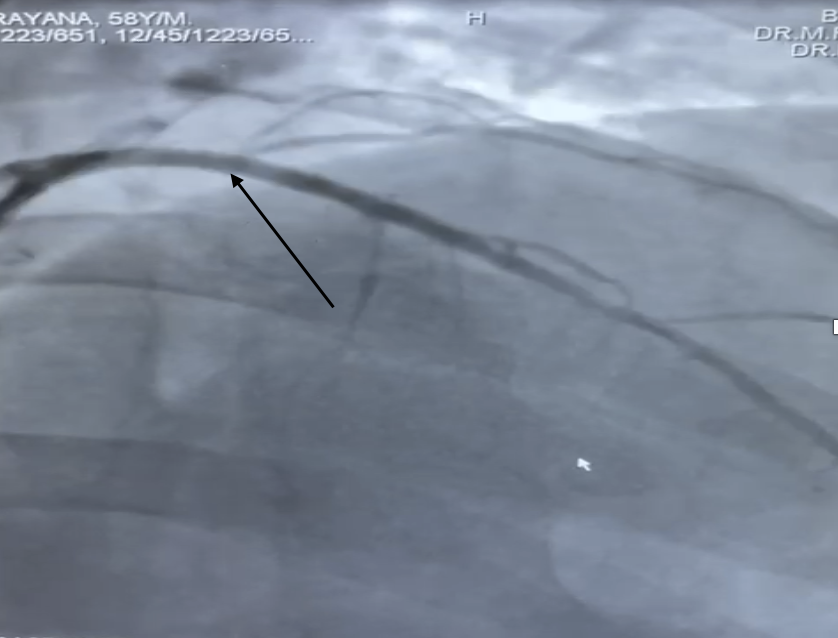
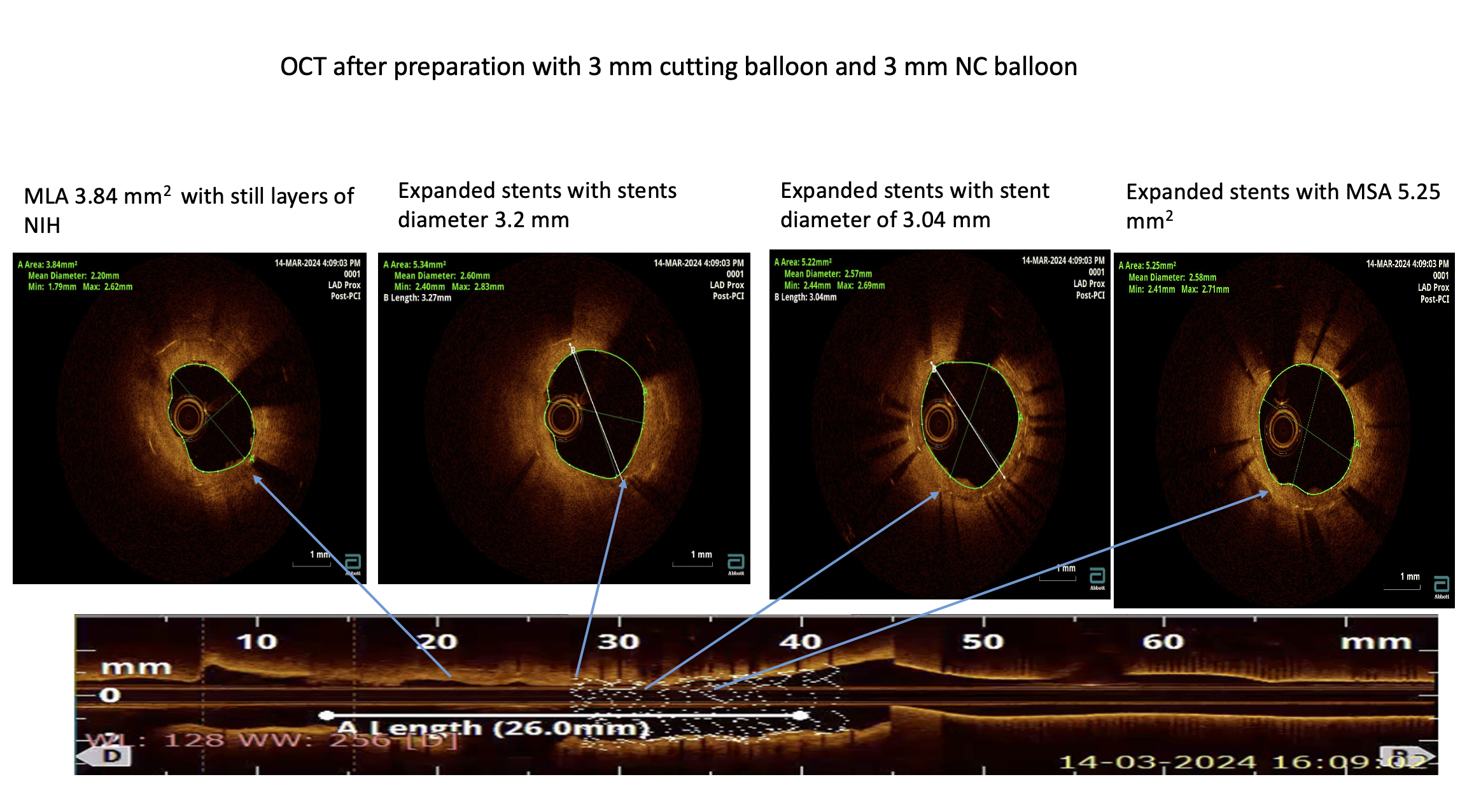
Lesion preparation was done with 3 mm Wolverine cutting balloon to address the neo intimal hyperplasia and further preparation was done with 3 mm NC balloon to further gain MLA(minimal luminal area) and to optimise the previously placed stents. After the lesion preparation OCT was repeated to check the lesion preparation and MLA. OCT showed well expanded previous stents and good gain luminal areas. Only at distal edge of stent the MLA is still 3.84 mm2 with some layers of NIH, so a 3.5 mm NC was used at the site to further gain the MLA. After satisfactory lesion preparation a 3x 25 mm Sirolimus DEB( drug eluting balloon) was applied which was well expanded with out any waist. The final angiogram showed good TIMI III with no flow limiting dissections.

Case Summary
•Recurrent ISR is not unusual in contemporary practice.Recurrent ISR occurs in approximately 20% of all ISR cases.Use of Intracoronary imaging may provide insights into the underlying mechanisms and to guide management.Optical coherence tomography (OCT) allows for better tissue characterisation of ISR .Lesion preparation with special balloon like cutting balloons may required in ISR .Patients with recurrent ISR are refractory to usual treatment modalities. Drug-coated balloons may have a beneficial effect in recurrent ISR .