
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-014
A Curious Case of Left Main Coronary Artery Stenosis From Isolated Periaortic Immunoglobulin G4-Related Disease
By Jie Jun Wong, Jack Wei Chieh Tan
Presenter
Jie Jun Wong
Authors
Jie Jun Wong1, Jack Wei Chieh Tan1
Affiliation
National Heart Centre, Singapore1,
View Study Report
TCTAP C-014
Coronary - ACS/AMI
A Curious Case of Left Main Coronary Artery Stenosis From Isolated Periaortic Immunoglobulin G4-Related Disease
Jie Jun Wong1, Jack Wei Chieh Tan1
National Heart Centre, Singapore1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
The patient is a 50-year-old female with no significant personal medical history, cardiovascular risk factors, or family history of cardiac diseases. She reports a one-month history of worsening exertional dyspnea and postural lightheadedness. She now presents to the emergency department following a syncopal episode while standing. She denies any palpitations, chest discomfort, or diaphoresis. Cardiovascular, pulmonary, and neurological examinations are unremarkable.
Relevant Test Results Prior to Catheterization
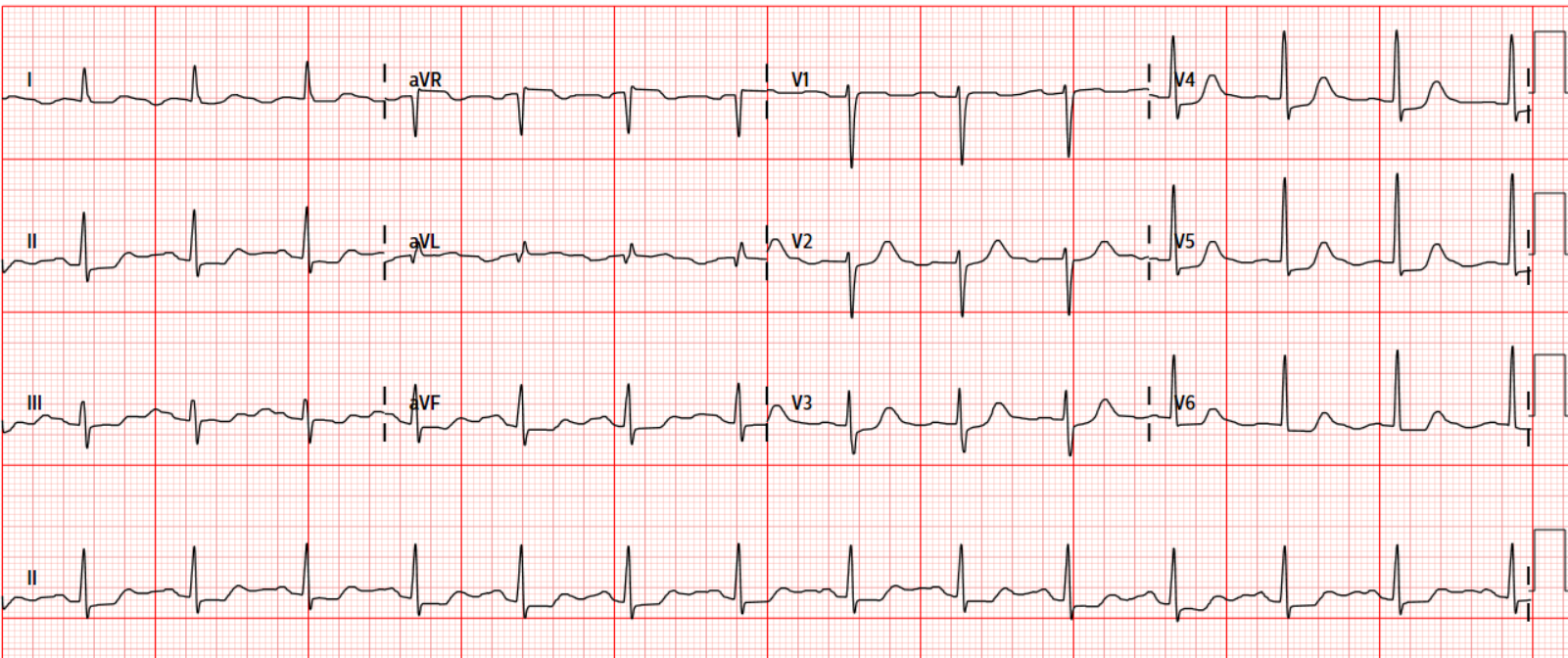
Electrocardiography found diffuse ST-segment depression with aVR lead ST-segment elevation. High-sensitivity troponin-T was raised at 127 ng/L.
Relevant Catheterization Findings
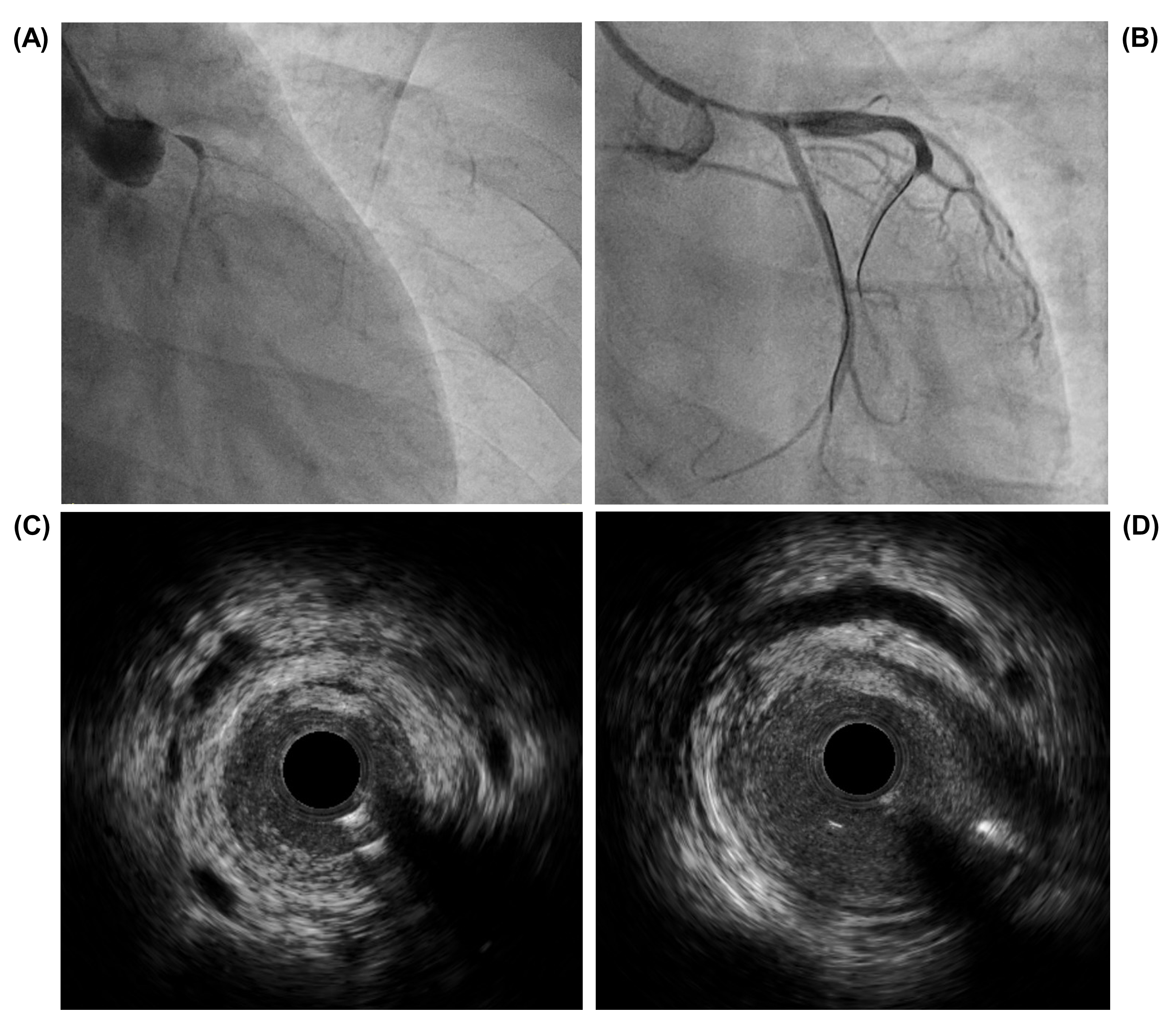
Urgent coronary angiography was performed, which showed subtotal left main coronary artery (LMCA) tapered occlusion with TIMI 1 flow and collaterals from the right coronary artery. Plain balloon angioplasty was performed with lumen and flow restoration. Intravascular vascular ultrasound (IVUS) showed extraluminal encasement LMCA and ostial left anterior descending artery with thickening of the adventitia surrounded by extraluminal masses and multiple microchannels.
Interventional Management
Procedural Step
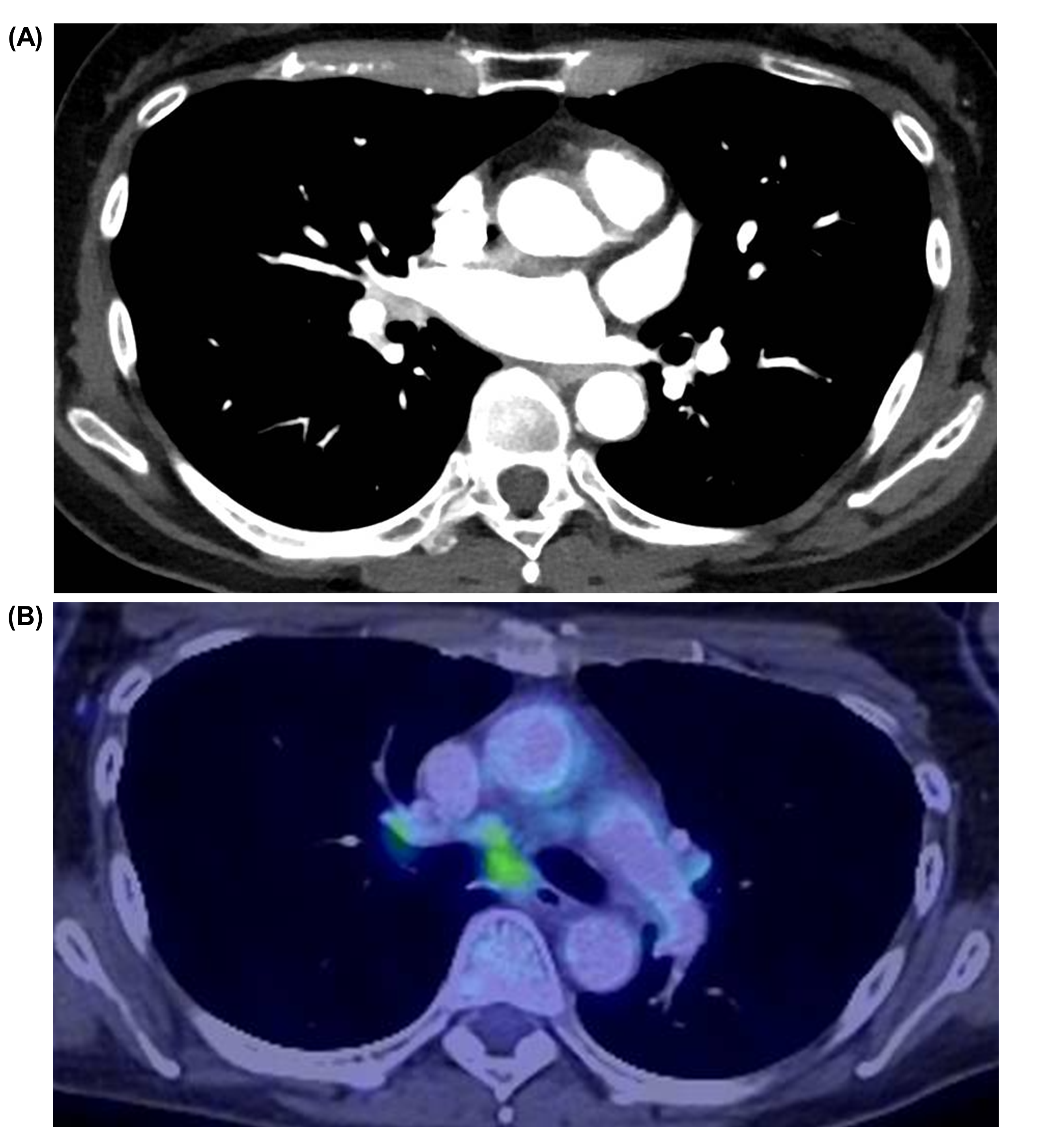
Laboratory tests showed low C3 and C4 complements with raised Immunoglobulin G4 subclass levels. Transthoracic echocardiography showed preserved left ventricular ejection fraction and no resting regional wall motion abnormalities. 18F-Positron emission tomography (PET) with contrast-enhanced multi-slice computed tomography (CT) with myocardial suppression showed FDG-avid circumferential thickening of the aortic root extending along the LMCA, pulmonary trunk, and carotids. Mild FDG-avidity was seen in the supra- and infra-diaphragmatic lymph nodes and spleen. High-dose prednisolone was initiated with plans for subsequent coronary reassessment.
Case Summary
ImmunoglobulinG4-related disease (IgG4-RD) is a multiorgan chronic fibroinflammatory disordercharacterized by dense plasma cell infiltration. Here, we describe a rare caseof symptomatic LMCA stenosis from isolated periaortic IgG4-RD.