
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-230
Double Trouble: Bilateral Heavily Calcified Iliac Arteries With Chronic Total Occlusion of the Left Superficial Femoral Artery
By Ng Kwang How, Ahmad Rafizi Hariz Ramli
Presenter
Ng Kwang How
Authors
Ng Kwang How1, Ahmad Rafizi Hariz Ramli1
Affiliation
University Malaya Medical Center, Malaysia1,
View Study Report
TCTAP C-230
Endovascular - Iliac / SFA Intervention
Double Trouble: Bilateral Heavily Calcified Iliac Arteries With Chronic Total Occlusion of the Left Superficial Femoral Artery
Ng Kwang How1, Ahmad Rafizi Hariz Ramli1
University Malaya Medical Center, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Madam A, a 85-year-old female suffered from bilateral lower limbs claudication pain for 2 years, which has worsened recently and is worse on the left side. The claudication distance was 30 meters. There were no ulcers, numbness or altered sensation. Treatments options were discussed and she opted for endovascular intervention. Bilateral lower limbs examinations showed shiny skin, hair loss, brittle nails, impalpable DPA and PTA pulses. ABI of the left side was 0.37 and right side was 0.43.

Relevant Test Results Prior to Catheterization
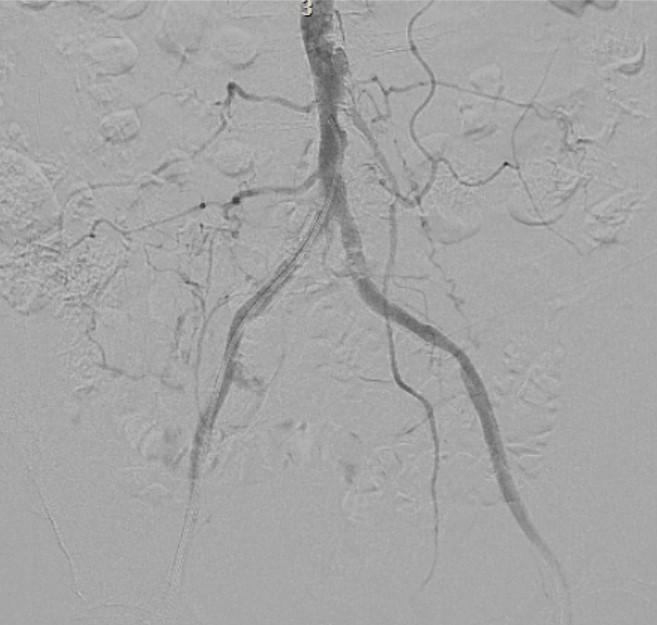
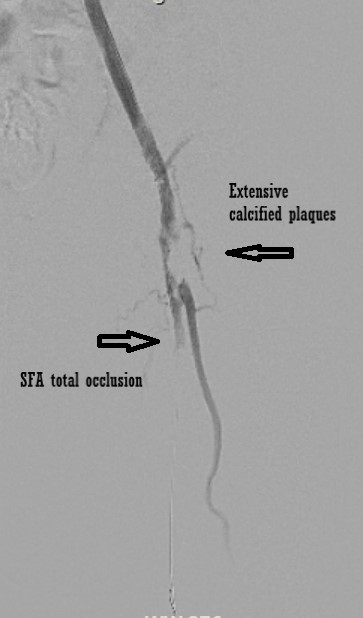
Computed tomography angiography of lower limbs revealed extensive atherosclerotic diffuse disease, with heavily calcified plaques and stenosis over bilateral common iliac, external and internal iliac arteries and common femoral arteries (CFA). Proximal left superficial femoral artery (SFA) and mid-segment of right SFA showed complete occlusion. There was also diffuse calcification over bilateral below the knee vessels.


Relevant Catheterization Findings
Ultrasound guided right Common femoral artery puncture was done and a 6Fr sheath was inserted. Heavily calcified lesions over bilateral common iliac arteries were visualized on angiography. There were moderate to severe stenosis at bilateral common iliac to common femoral arteries. Proximal left SFA and mid right SFA total occlusion were confirmed.

Interventional Management
Procedural Step
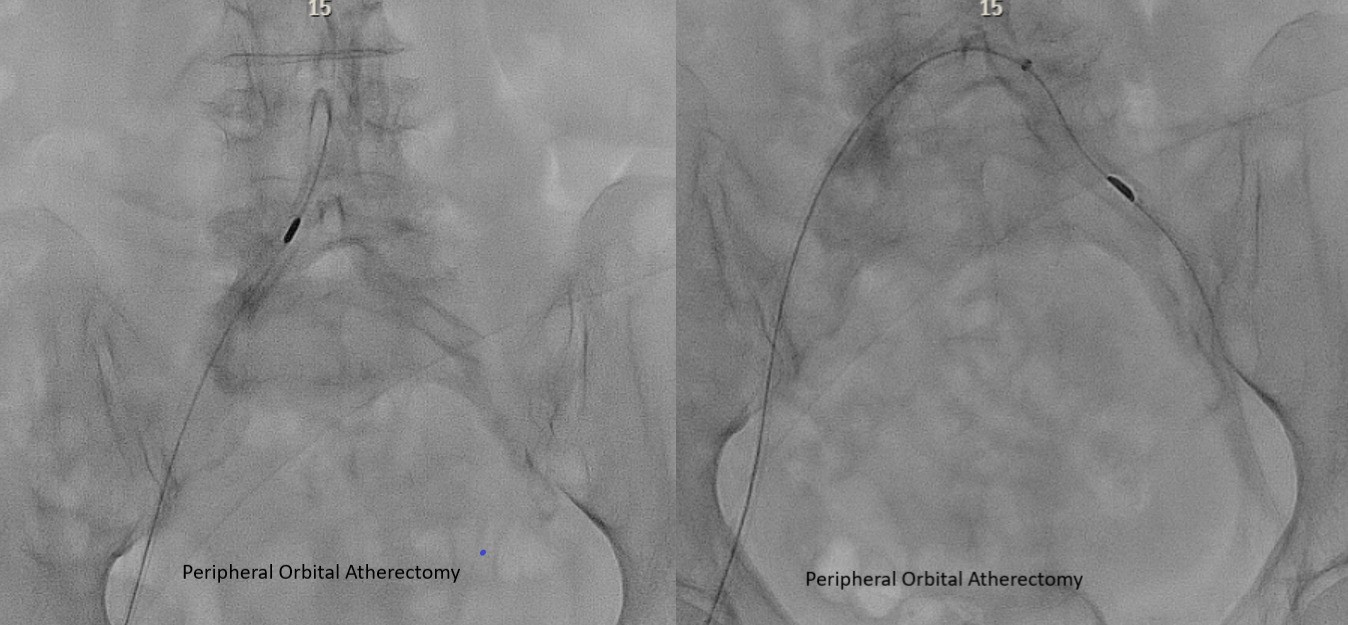
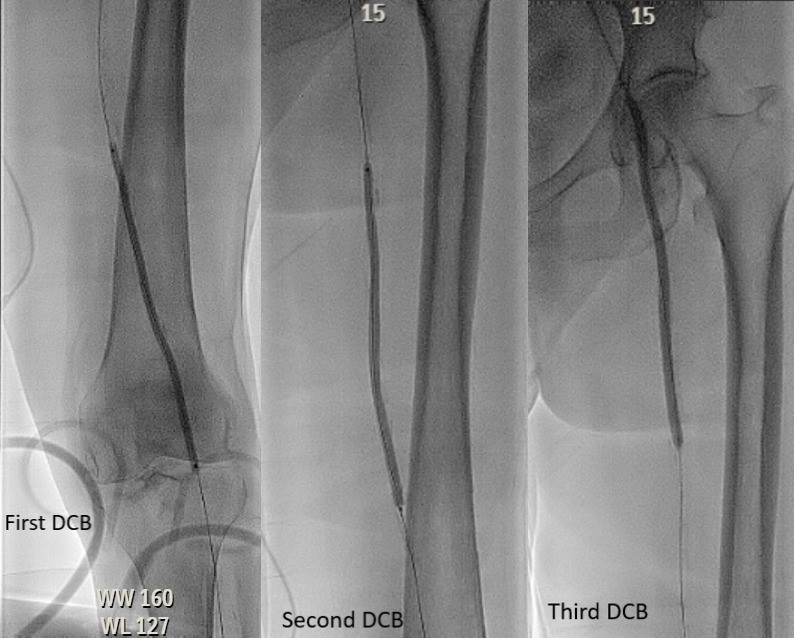
Terumo wire 0.035-inch with catheter JR 3.5 was advanced to descending aorta and exchanged to Viperwire. Stealth 360 Peripheral Orbital atherectomy (CSI, USA) was performed to right common iliac for 5 runs. Pre-dilatated right CFA, external iliac and common iliac with Balloon Jade 6.0x 150mm(OrbusNeich,HongKong).Proceeded with angioplasty to the left side. Standard sheath was exchanged to 6Fr Fortress crossover-45 sheath(Biotronik, Germany). Orbital atherectomy to left common iliac was done. Exchanged to Amplatz Superstiff 0.035” wire(Boston Scientific,USA) and pre-dilatated left external iliac and common iliac with Balloon Jade 6.0 x 150mm(OrbusNeich, HongKong). Left SFA complete occlusion was crossed with Terumo wire. Extensive calcium plaques were seen at left CFA and Orbital atherectomy to left CFA was performed. Subsequently, Hi-Torque Command™ 18 ST wire(Abbott Laboratories, USA) was advanced to posterior tibial artery. Left popliteal, SFA and CFA were predilated with Jade(OrbusNeich, HongKong)3.0x60mm, Jade 4.0x120mm and Jade5.0x120mm sequentially. The balloons were inflated until full expansion and demonstrated angiographically.Angioplasty with Drug-Coated Balloon IN.PACT Admiral(Medtronic,USA) 4.0x150mm, IN.PACT Admiral 5.0x150mm and IN.PACT Admiral6.0x150mm were performed from distal SFA to CFA. The final angiography showed successful perfusion to the left popliteal trifurcation. She was discharged well and planned for staged angioplasty to the right lower limb.

Case Summary
Peripheral artery diseases are very common and often under-diagnosed. Calcified lesion is not unusual and is expected to increase in prevalence. Heavily calcified lesion is a predictor of poor long-term outcome as it is difficult to prepare the lesions optimally, and is associated with dissection, the need of bailout stenting, failure to deliver devices, stent under-expansion, and eventually higher target lesion failure. Endovascular revascularization of symptomatic chronic limb-threatening is less invasive, safe and effective. Atherectomy can effectively modify calcium plaques, hence timely use of appropriate atherectomy devices can save time, achieve better preparation and optimal results.