
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-175
Once in a Blue Moon
By Wittawat Wattanasiriporn
Presenter
Wittawat Wattanasiriporn
Authors
Wittawat Wattanasiriporn1
Affiliation
Rajavithi Hospital, Thailand1,
View Study Report
TCTAP C-175
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Once in a Blue Moon
Wittawat Wattanasiriporn1
Rajavithi Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Relevant Test Results Prior to Catheterization
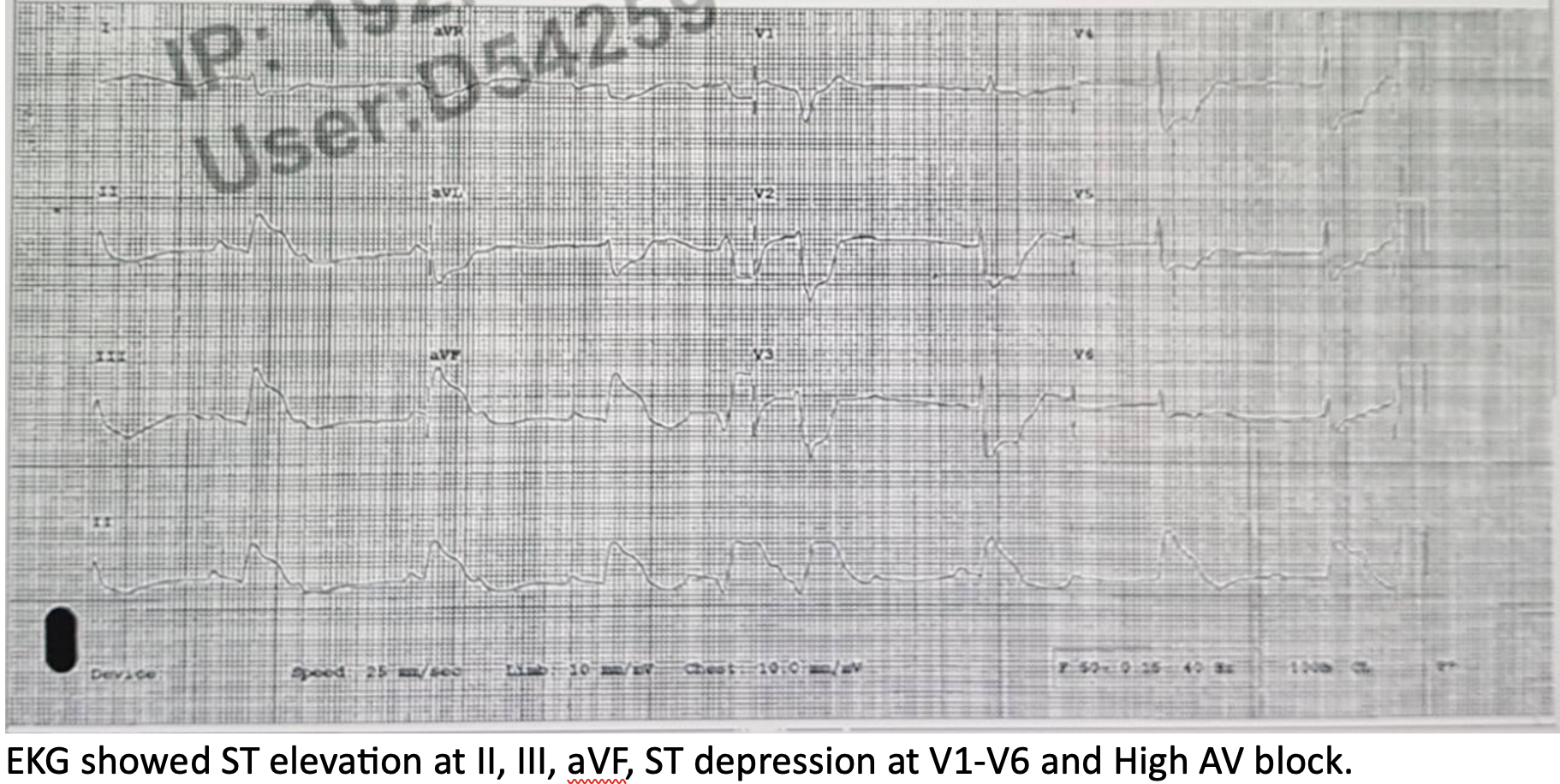
EKG showed ST elevation at II, III, aVF, ST depression at V1-V6 and High AV block. Echocardiogram showed LVEF 42%, HK at anterior, anterolateral and inferior wall, no significant Valvular heart disease. Chest x-ray showed bilateral pulmonary congestion.
Relevant Catheterization Findings
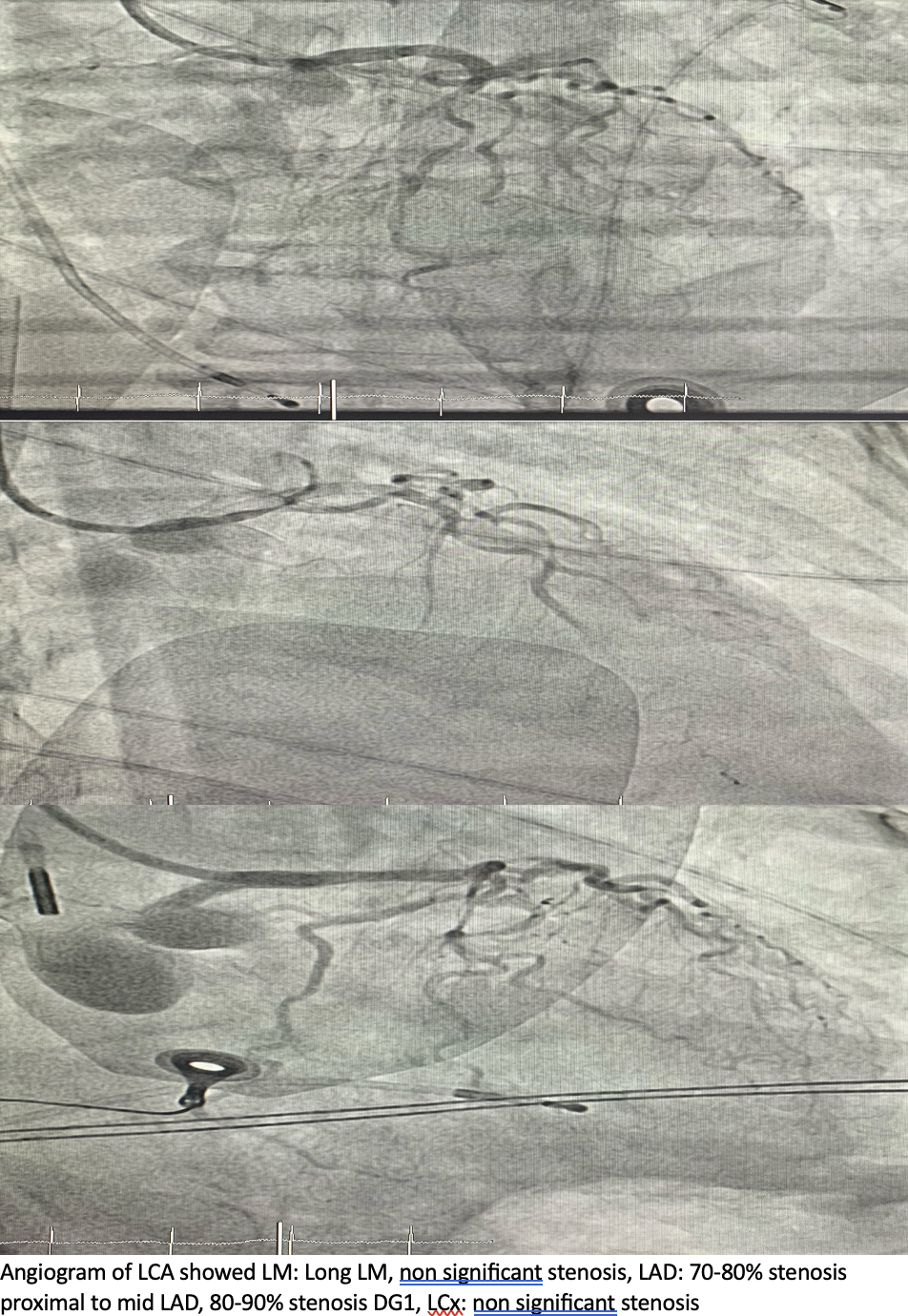
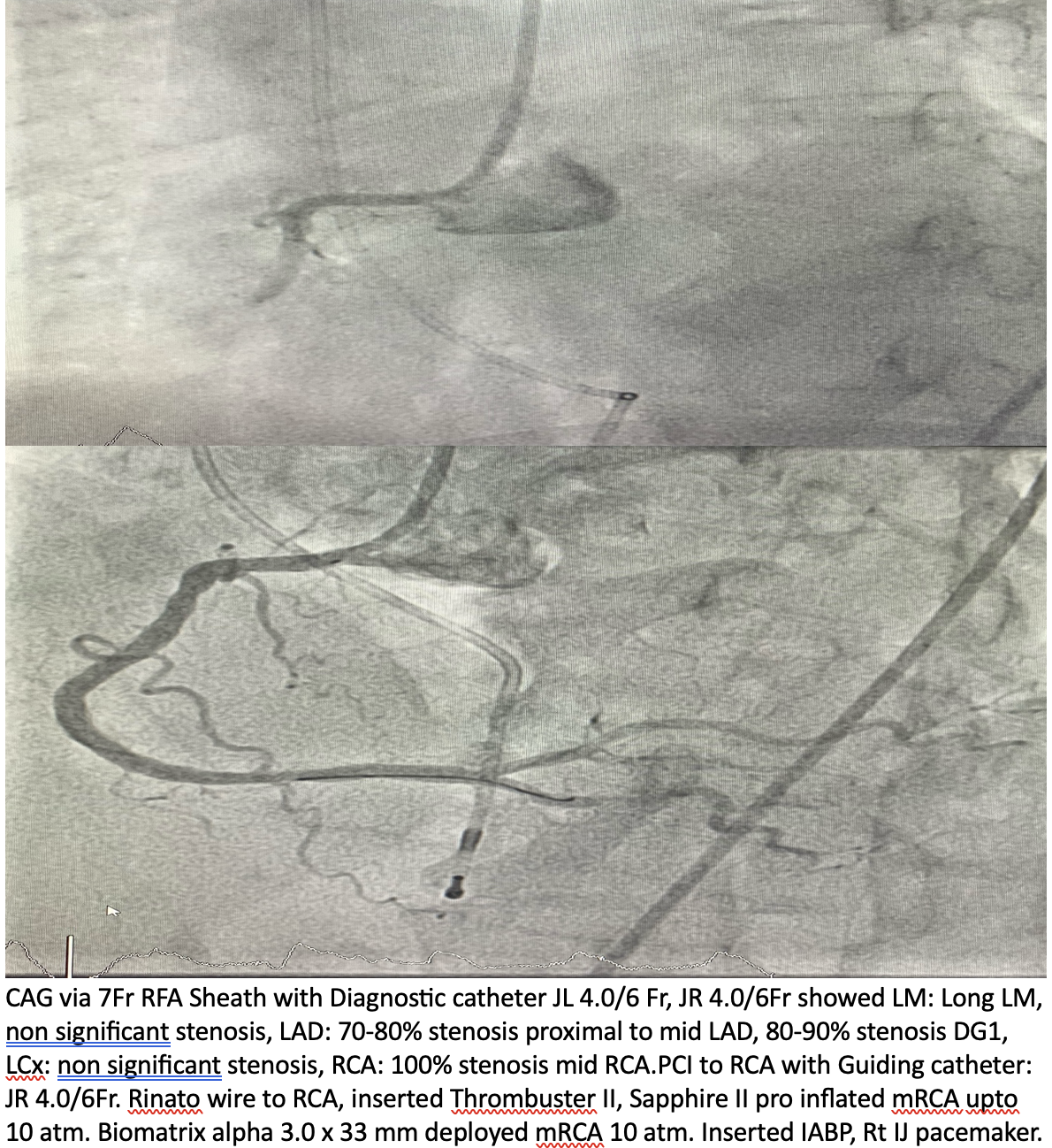
STEMI fast tract was activated. CAG via 7Fr RFA Sheath with Diagnostic catheter JL 4.0/6 Fr, JR 4.0/6Fr showed LM: Long LM, non significant stenosis, LAD: 70-80% stenosis proximal to mid LAD, 80-90% stenosis DG1, LCx: non significant stenosis, RCA: 100% stenosis mid RCA.PCI to RCA with Guiding catheter: JR 4.0/6Fr. Rinato wire to RCA, inserted Thrombuster II, Sapphire II pro inflated mRCA upto 10 atm. Biomatrix alpha 3.0 x 33 mm deployed mRCA 10 atm. Inserted IABP, Rt IJ pacemaker.
Interventional Management
Procedural Step
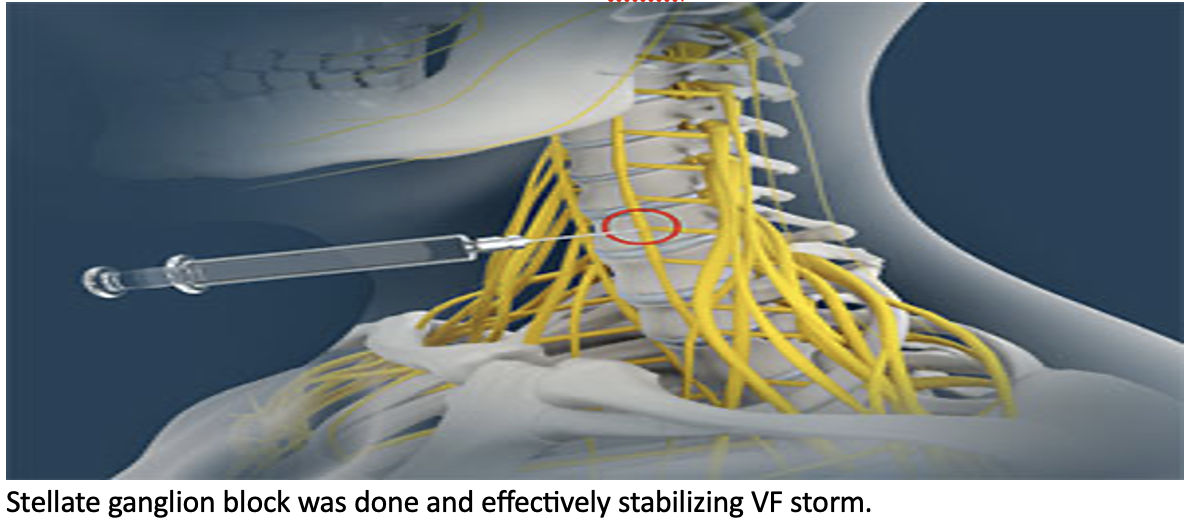
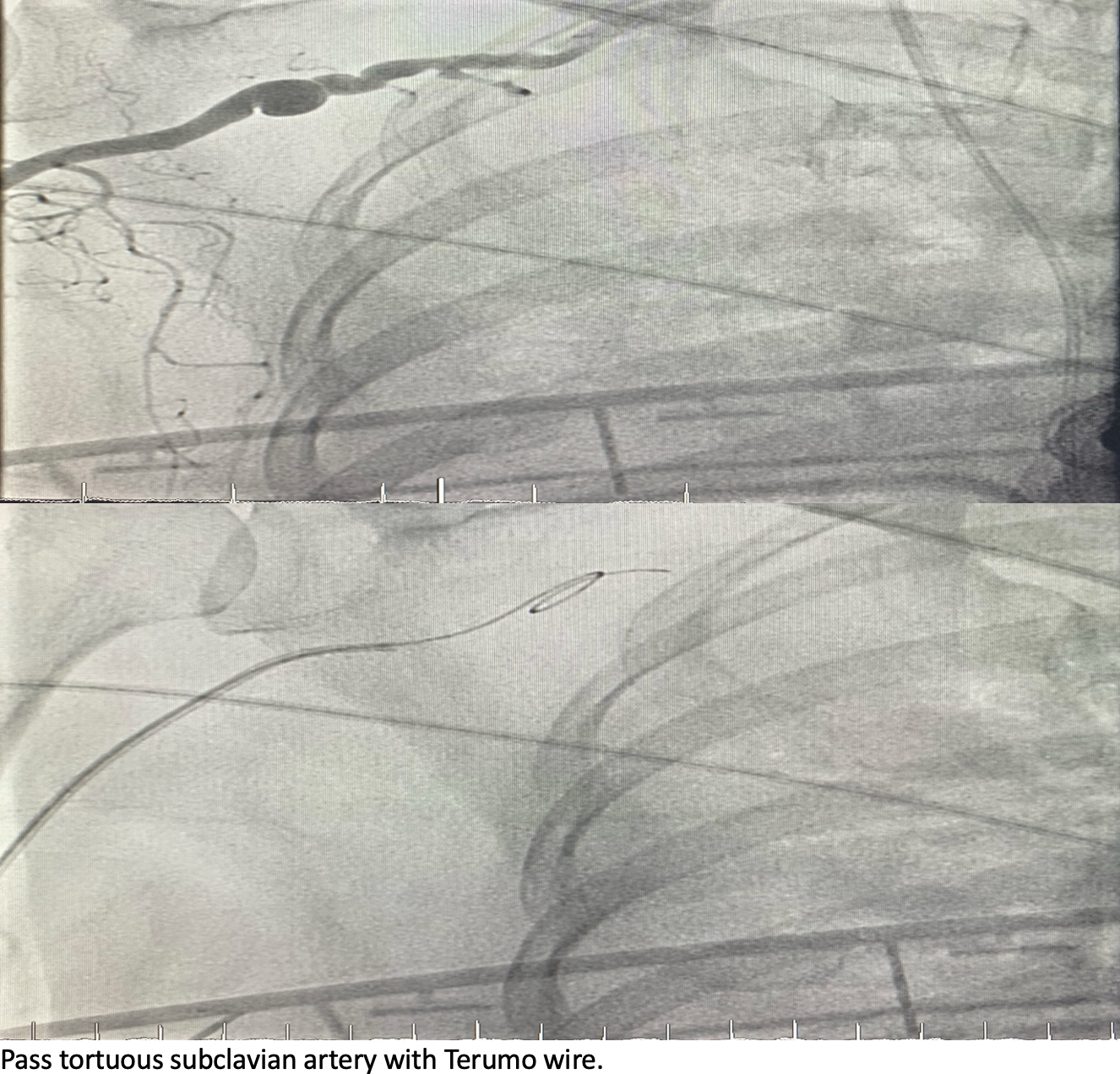
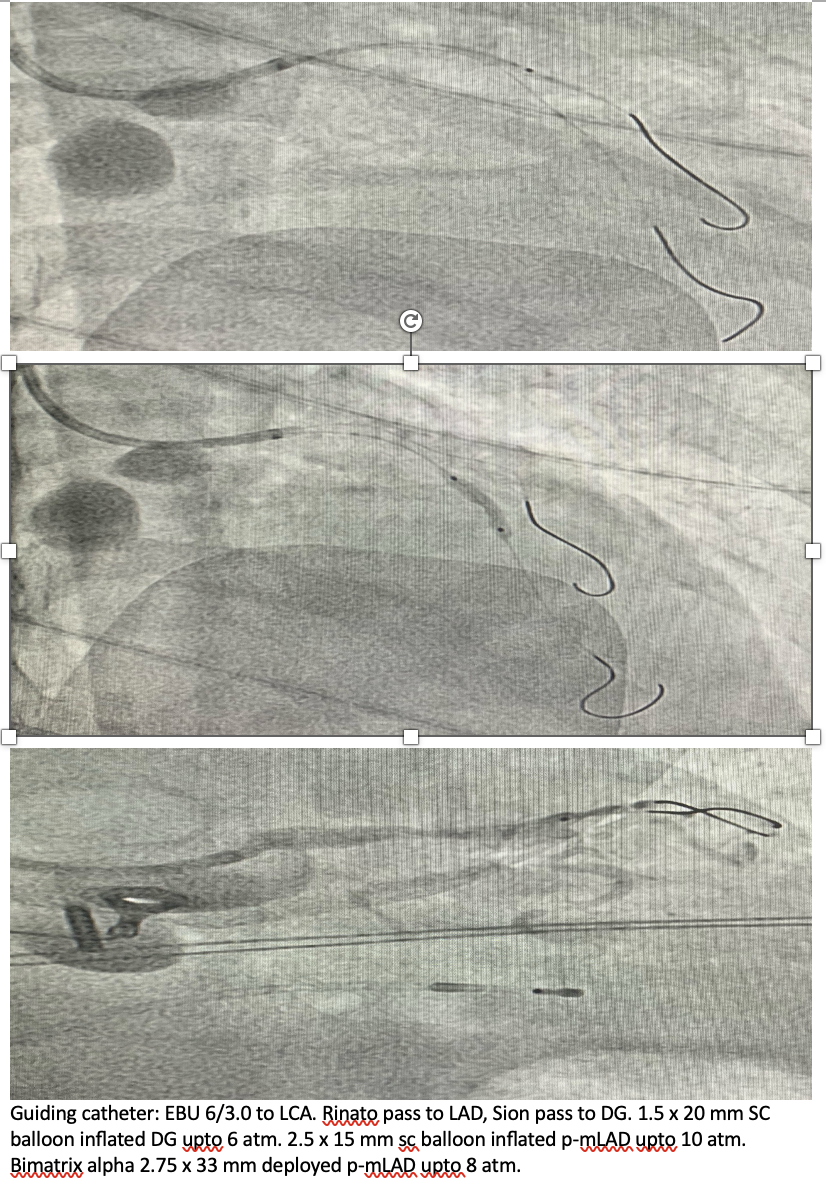
After sent the patient back to CCU developed cardiac arrest with VF storm.Multiple defibrillator shocks was done. The patient was given IV Amiodarone then IV Lidocaine. Anti-tachycardia overdrive pacing can not break VF storm. VA ECMO was initiated. Stellate ganglion block was done and effectively stabilizing VF storm and sent the patient to perform PCI to LAD-DG. PCI to LAD-DG via Rt radial access using 6Fr sheath. Pass tortuous subclavian artery with Terumo wire. Guiding catheter: EBU 6/3.0 to LCA. Rinato pass to LAD, Sion pass to DG. 1.5 x 20 mm SC balloon inflated DG upto 6 atm. 2.5 x 15 mm sc balloon inflated p-mLAD upto 10 atm. Bimatrix alpha 2.75 x 33 mm deployed p-mLAD upto 8 atm.
Case Summary
Learning points