
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP A-061
Differential Efficacy and Safety of Antiplatelet Strategies After PCI Across Different BMI
By Kuan-Po Chiu, Zhen Cheng Hwang, Su-Kiat Chua, Donna Shu-Han Lin
Presenter
Kuan-Po Chiu
Authors
Kuan-Po Chiu1, Zhen Cheng Hwang1, Su-Kiat Chua1, Donna Shu-Han Lin1
Affiliation
Shin Kong Wu Ho-Su Memorial Hospital, Taiwan1
View Study Report
TCTAP A-061
Pharmacotherapy (Coronary)
Differential Efficacy and Safety of Antiplatelet Strategies After PCI Across Different BMI
Kuan-Po Chiu1, Zhen Cheng Hwang1, Su-Kiat Chua1, Donna Shu-Han Lin1
Shin Kong Wu Ho-Su Memorial Hospital, Taiwan1
Background
In patients receiving percutaneous coronary intervention (PCI), individualized risk assessment is recommended to guide dual antiplatelet therapy (DAPT) strategies. Subgroup analyses of single randomized controlled trials (RCTs) have demonstrated that patients with lower body mass index (BMI) have a higher risk of adverse clinical outcomes compared to those with higher BMI, but no direct comparison between DAPT strategies in patients with various BMI has been conducted previously. In this study, we aimed to evaluate the BMI-dependent effects of these treatment strategies on clinical outcomes.
Methods
A systematic search of Pubmed, EMBASE and Cochrane databases identified RCTs comparing DAPT strategies in patients receiving PCI that reported subgroup data of different BMI for the following three outcomes: (1) major adverse cardiovascular events (MACE); (2) bleeding; and (3) net adverse clinical events (NACE, a composite of bleeding and MACE). The DAPT strategies of interest included: (1) standard DAPT; (2) short-term DAPT followed by P2Y12 inhibitors; and (3) short-term DAPT followed by aspirin. Outcome comparisons between different DAPT strategies were performed using restricted maximum likelihood multivariate meta-analysis with a random-effects model. (PROSPERO ID: CRD42024559223).
Results
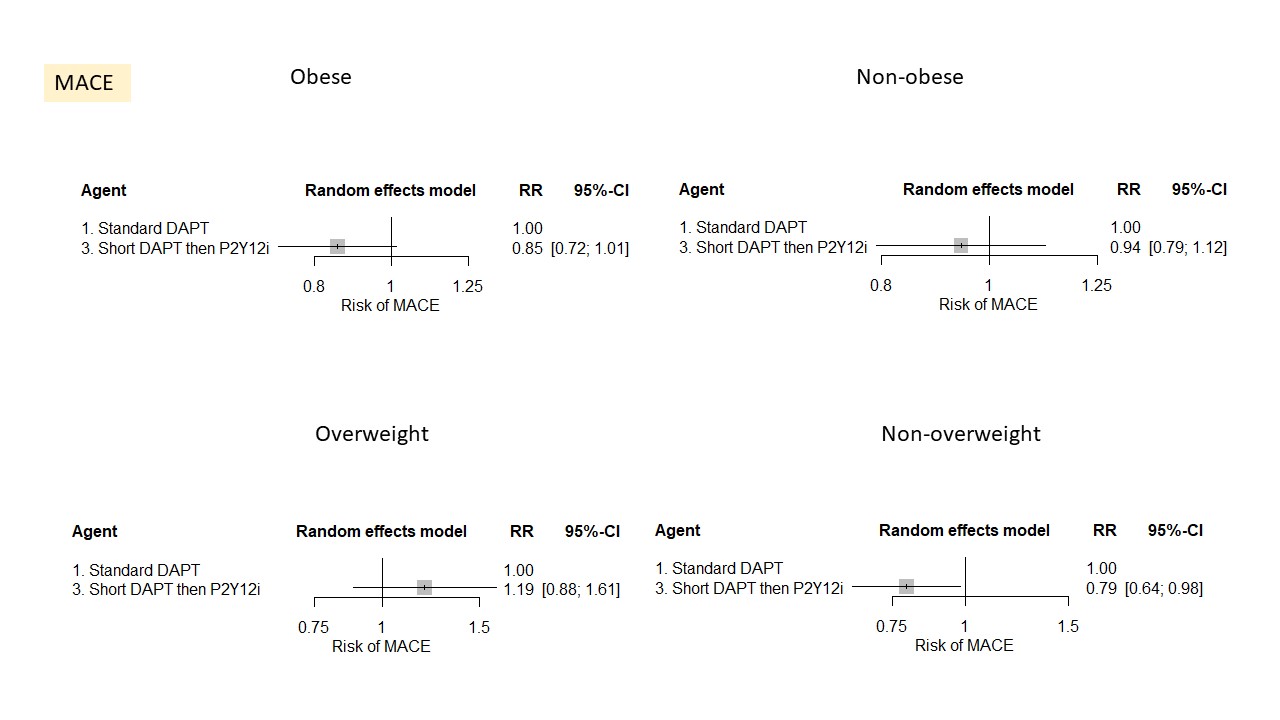
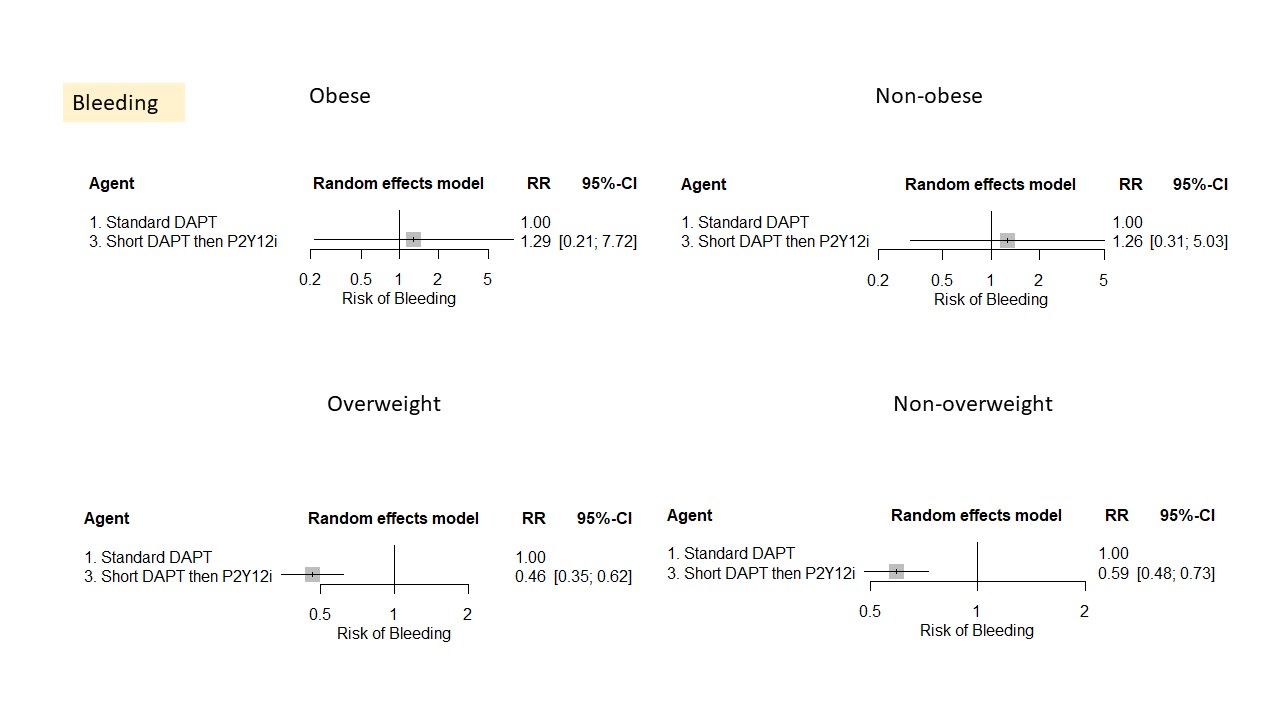
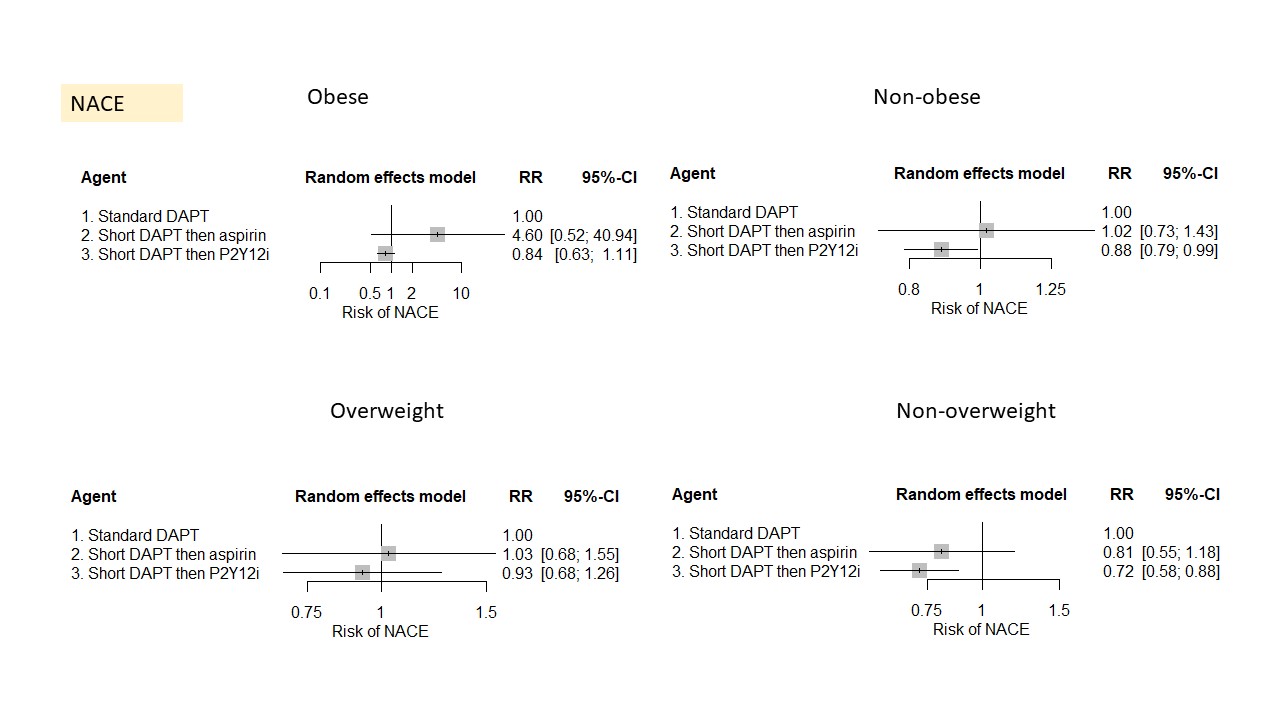
8 eligible RCTs (51,574 patients) were included. In non-overweight patients, the short-term DAPT followed by P2Y12 inhibitor strategy was associated with a statistically significant reduction in the risks of NACE (RR: 0.72; 95% CI: 0.58-0.88), MACE (RR: 0.79; 95% CI: 0.64-0.98), and bleeding (RR: 0.59; 95% CI: 0.48-0.73) compared to standard DAPT. In overweight patients, the short-term DAPT followed by P2Y12 inhibitor strategy was associated with a reduced risk of bleeding (RR: 0.46; 95% CI: 0.35-0.62), but an increased risk of MACE (RR: 1.19; 95% CI: 0.88-1.61). However, in obese patients, the short-term DAPT followed by P2Y12 inhibitor strategy was associated with a reduced risk of MACE (RR: 0.85; 95% CI: 0.72-1.01) and an increased risk of bleeding (RR: 1.29; 95% CI: 0.21-7.72). Regarding NACE, the short-term DAPT followed by P2Y12 inhibitor strategy was favorable across all BMI categories.
Conclusion
Different MACE and bleeding risks were observed across different BMI categories. DAPT strategies should be guided by an individualized risk assessment.