
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP A-064
Comparison of Cerebral Embolic Debris Capture During TAVR in Bicuspid vs. Tricuspid Aortic Valve Stenosis: Impact of Valve Type on Particle Size Distribution
By Amy Jing Ling, Wei-Hsian Yin
Presenter
Amy Jing Ling
Authors
Amy Jing Ling1, Wei-Hsian Yin2
Affiliation
Cheng Hsin General Hospital, Malaysia1, Cheng Hsin General Hospital, Taiwan2
View Study Report
TCTAP A-064
Bicuspid AV
Comparison of Cerebral Embolic Debris Capture During TAVR in Bicuspid vs. Tricuspid Aortic Valve Stenosis: Impact of Valve Type on Particle Size Distribution
Amy Jing Ling1, Wei-Hsian Yin2
Cheng Hsin General Hospital, Malaysia1, Cheng Hsin General Hospital, Taiwan2
Background
Patients with bicuspid aortic valve (BAV) stenosis undergoing transcatheter aortic valve replacement (TAVR) are reported to have higher stroke rates compared to those with tricuspid aortic valve (TAV) stenosis. Cerebral embolic protection (CEP) devices can reduce stroke risk during TAVR by capturing embolic debris. This study aims to assess differences in debris capture by CEP between BAV and TAV patients, with a focus on different valve types.
Methods
This study included 202 consecutive patients who underwent TAVR with the SENTINEL CEP device (Boston Scientific) from April 2022 to October 2024. Of these, 118 patients received a self-expanding Evolut R/PRO valve (SEV) (Medtronic), while 84 received a balloon-expandable Sapien 3 valve (BEV) (Edwards Lifesciences). Twenty-nine patients (14.36%) had BAV. Particles captured by the CEP device were analyzed and compared based on valve type and aortic valve anatomy.
Results
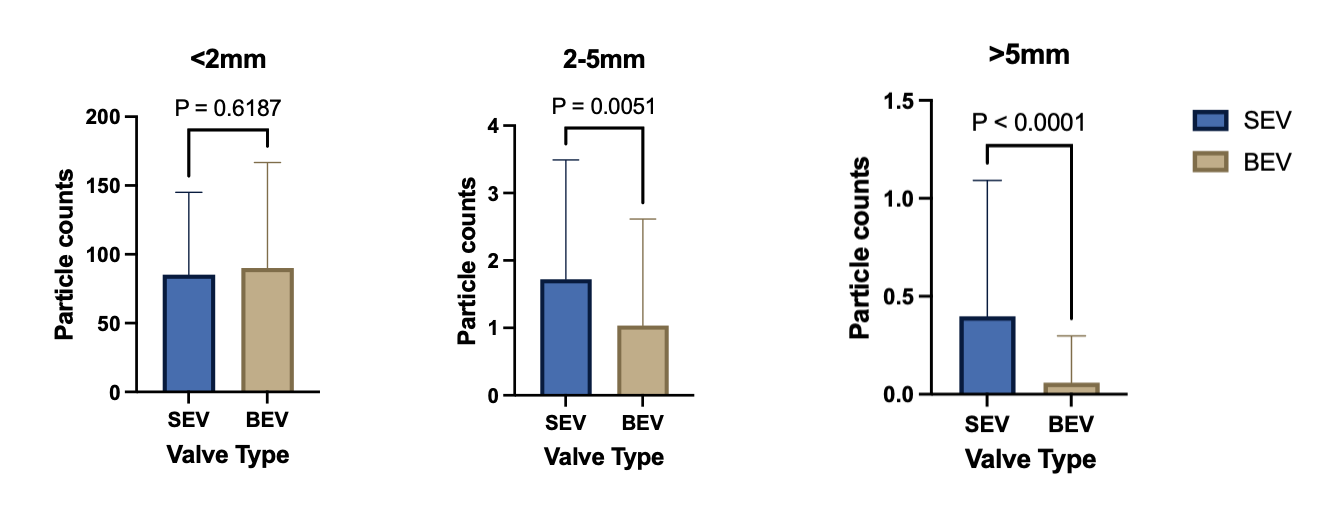
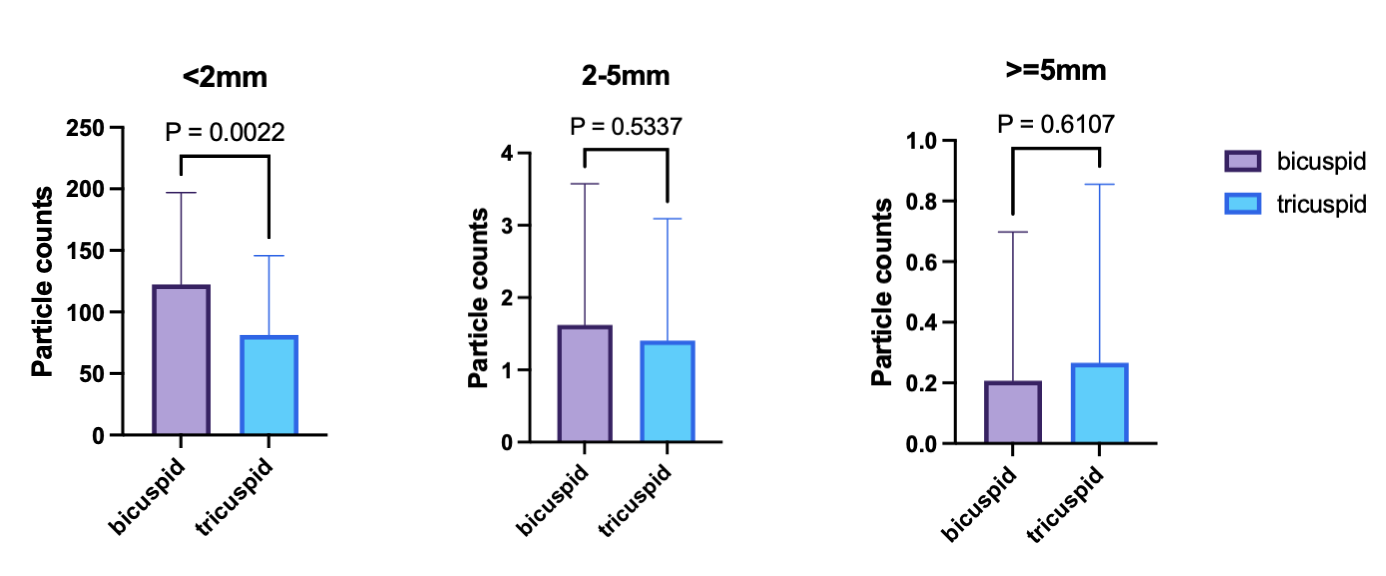
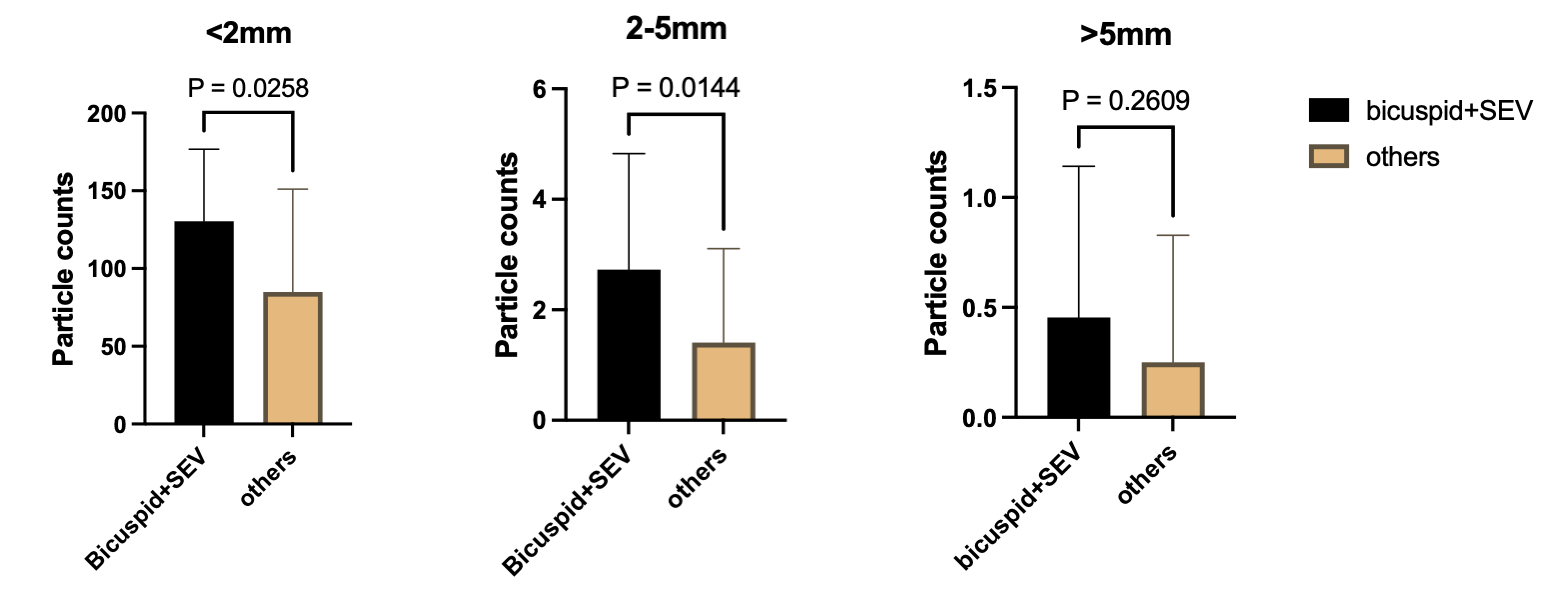
Significantly more particles larger than 2 mm were captured in the SEV group compared to the BEV group (particles 2–5 mm: SEV vs. BEV = 1.720 vs. 1.036; p = 0.005; particles ≥5 mm: SEV vs. BEV = 0.398 vs. 0.060; p < 0.0001). Conversely, significantly more particles smaller than 2 mm were captured in the BAV group compared to the TAV group (BAV vs. TAV = 122.4 vs. 81.39; p = 0.002). Among BAV patients, those who underwent TAVR with SEV had significantly more particles smaller than 5 mm captured compared to the TAV group (particles <2 mm: BAV vs. TAV = 130.5 vs. 84.84; p = 0.026; particles 2–5 mm: BAV vs. TAV = 2.727 vs. 1.406; p = 0.014).
Conclusion
This study demonstrated that significantly more particles smaller than 2 mm were captured by CEP during TAVR in BAV patients. In addition, particles larger than 2 mm were predominantly captured in the SEV group. These findings emphasize the importance of using CEP in BAV patients undergoing TAVR with SEV to reduce the risk of periprocedural stroke and mitigate potential long-term cognitive decline.