
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP A-035
Integrating Telescope and Plaque Modification Technique to Retrieve a Balloon Fragment Fracture in a Long Diffuse Calcified Lad Lesion
By Shadtharcharan Maniam, Seng Hsiung Toh, Jhi Hui Foo, Houng Bang Liew
Presenter
Shadtharcharan Maniam
Authors
Shadtharcharan Maniam1, Seng Hsiung Toh1, Jhi Hui Foo1, Houng Bang Liew1
Affiliation
Queen Elizabeth Hospital 2, Malaysia1
View Study Report
TCTAP A-035
Complication Management
Integrating Telescope and Plaque Modification Technique to Retrieve a Balloon Fragment Fracture in a Long Diffuse Calcified Lad Lesion
Shadtharcharan Maniam1, Seng Hsiung Toh1, Jhi Hui Foo1, Houng Bang Liew1
Queen Elizabeth Hospital 2, Malaysia1
Background
Calcified lesions are associated with higher rates of complications during percutaneous coronary intervention (PCI). Balloon fragment fracture and entrapment is a rare, but potentially severe complication of PCI. The resulting debris might lead to vessel occlusion and/or form a prothrombotic nidus, potentially leading to distal embolization, acute myocardial infarction, ventricular dysrhythmia, and even death. This is a 58 year old, gentleman, underlying hypertension, and dyslipidemia. An ADL independent gentleman, presented to us in May 2023 for NSTEMI. His LV function is around 55-60%. A coronary angiography was done, findings was in keeping with TVD. Patient was referred to cardiothoracic team for Coronary artery Graft bypass surgery, unfortunately he refused and opted for high risk multistage PCI. After having internal discussion among our team, we decided to re-vascularise the LAD first then followed by the RCA.
Methods
After the diagnostic angiography, we proceeded with stage PCI to the LAD.A 6Fr EBU was used to engage the LCA, PILOT 50 was used to advance to distal LAD. NC SAPPHIRE 2.0mmx10mm is used for dottering, but unable to pass the mid lesion. A TELESCOPE guide extension was used, still unable to advance, hence balloon is changed to SC BALLOON 0.85x10mm. Sequential pre-dilatation was done till it burst. Followed by further pre-dilatation with NC SAPPHIRE 2.25mmx15mm up-to 22 atm. However, lesion was still under prepared, hence decided for NCEMERGE 2.25mmx12mm. After post dilatation we were unable to pull out the balloon to the guiding catheter, noted the marker elongated and we realized the balloon fragment is entrapped.
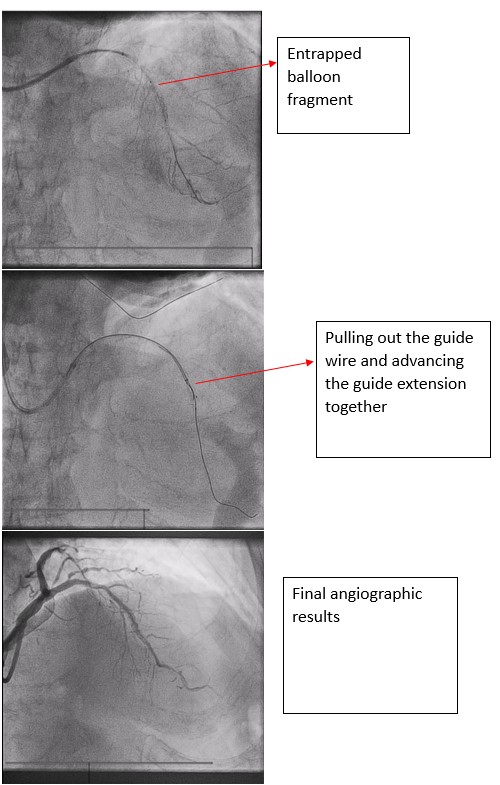
Results
However, flow remains TIMI 3. Decided for plaque modification technique using parallel wire to remove the remaining fragment, a FIELDER XTA was used to pass down to distal LAD. Sequential pre-dilatation done with SC SAPPHIRE 0.85x10mm, SC SAPPHIRE 1.0x10mm and SC SAPPHIRE 2.25x10mm at nominal pressure. A Guide extension was advance with 2 guidewires, as advancing the guide extension and pulling out the wire, we were able to pull out the balloon segment. After that a 7Fr EBU was used to re-engage the LCA. Sequential pre-dilatation was done with SCOREFLEX TRIO 3.0mmx30mm and 3 DCBs was delivered to the lesions. Final angiographic result was good.
Conclusion
In conclusion, balloon fragment fracture is a possible complication during lesion preparation in PCI especially in a long diffuse, calcified lesion. Being aware of and mastering the telescope and plaque modification technique, might be useful in bailing out in such critical situations.