
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP A-047
A Lower Contrast Volume Cut-Off for Coronary Angiographic Procedures to Reduce CIN Risk in CKD Patients: Is Less Truly More?
By Jessica Anastasia Setiawan, Catherine Jillian Hardi, Jesslyn Natalie Hariyanto, Sunanto Ng
Presenter
Jessica Anastasia Setiawan
Authors
Jessica Anastasia Setiawan1, Catherine Jillian Hardi1, Jesslyn Natalie Hariyanto1, Sunanto Ng2
Affiliation
Pelita Harapan University, Indonesia1, Siloam Hospital Lippo Village, Indonesia2
View Study Report
TCTAP A-047
High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
A Lower Contrast Volume Cut-Off for Coronary Angiographic Procedures to Reduce CIN Risk in CKD Patients: Is Less Truly More?
Jessica Anastasia Setiawan1, Catherine Jillian Hardi1, Jesslyn Natalie Hariyanto1, Sunanto Ng2
Pelita Harapan University, Indonesia1, Siloam Hospital Lippo Village, Indonesia2
Background
Chronic kidney disease (CKD) in coronary artery disease (CAD) is associated with increased risk of procedural complications such as contrast-induced nephropathy (CIN). The Mehran Risk Score (MRS) is a tool used to predict CIN that marks only one point for every 100 mL of contrast used, but some studies suggested an even lower contrast volume cut-off as a risk prevention strategy. This study aims to evaluate whether this lower cut-off for contrast volume is associated with lower events of CIN in CKD patients.
Methods
This cohort retrospective study included grade 3A or above CKD patients that underwent coronary angiography (CAG) and percutaneous coronary intervention (PCI). Patients undergoing hemodialysis, cardiogenic shock, requiring hemodynamic support, and consuming nephrotoxic drugs were excluded. The lower contrast volume cut-off was defined as 30 mL for CAG and 100 mL for PCI. The primary outcome was CIN, defined as post-procedural SrCr (serum creatinine) increase ≥ 0.5 mg/dL within 48 - 72 hours from baseline.
Results
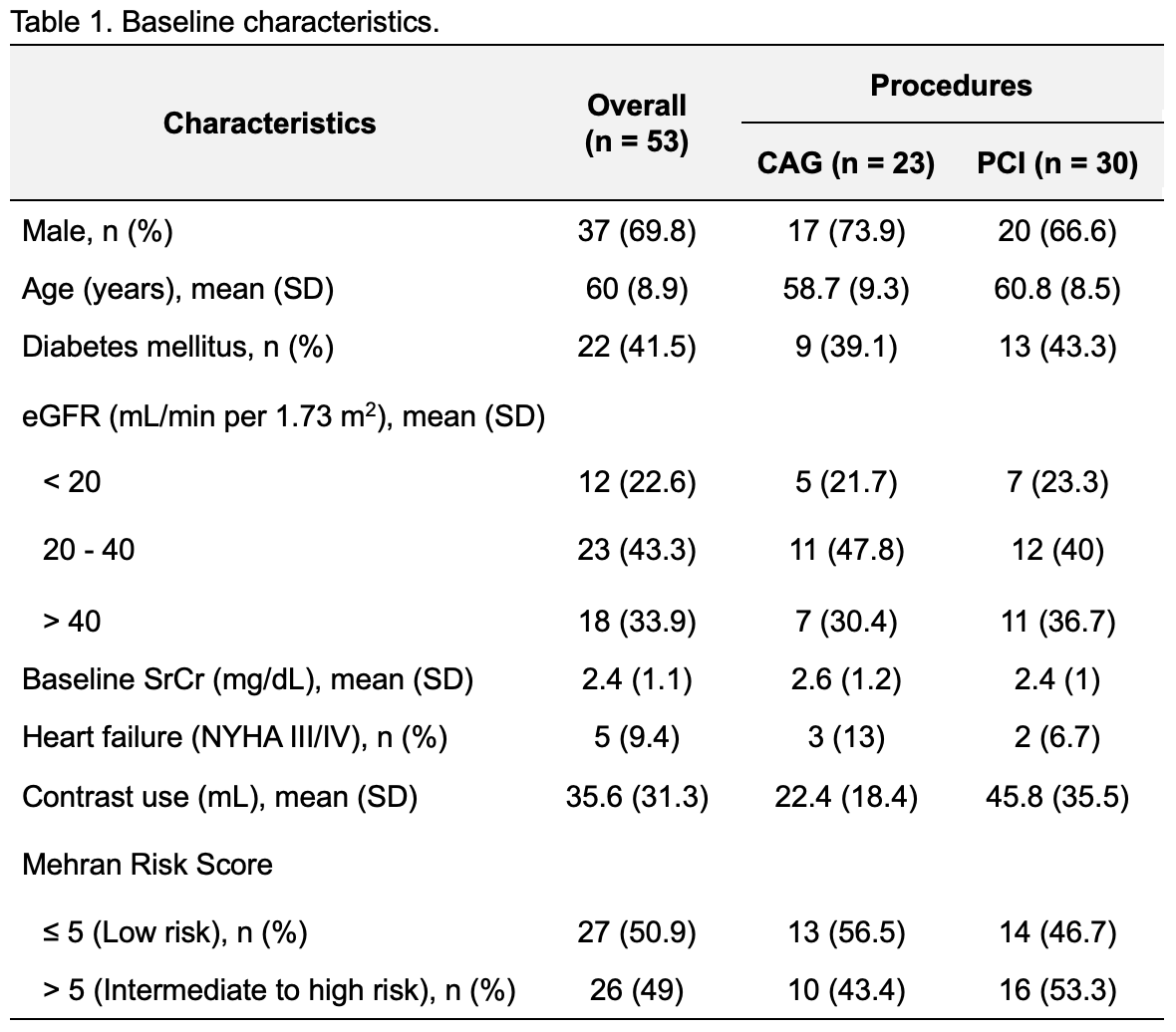
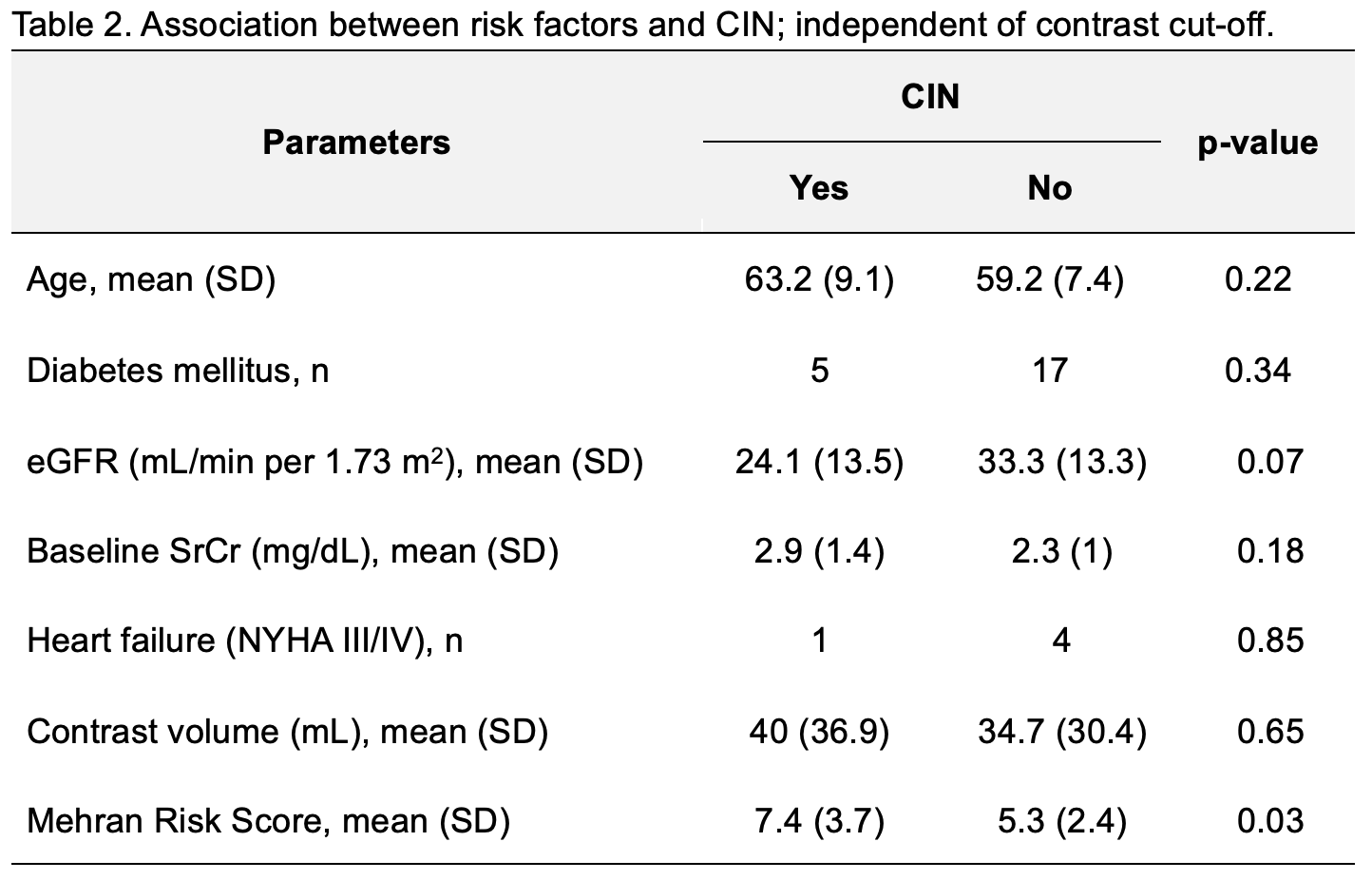
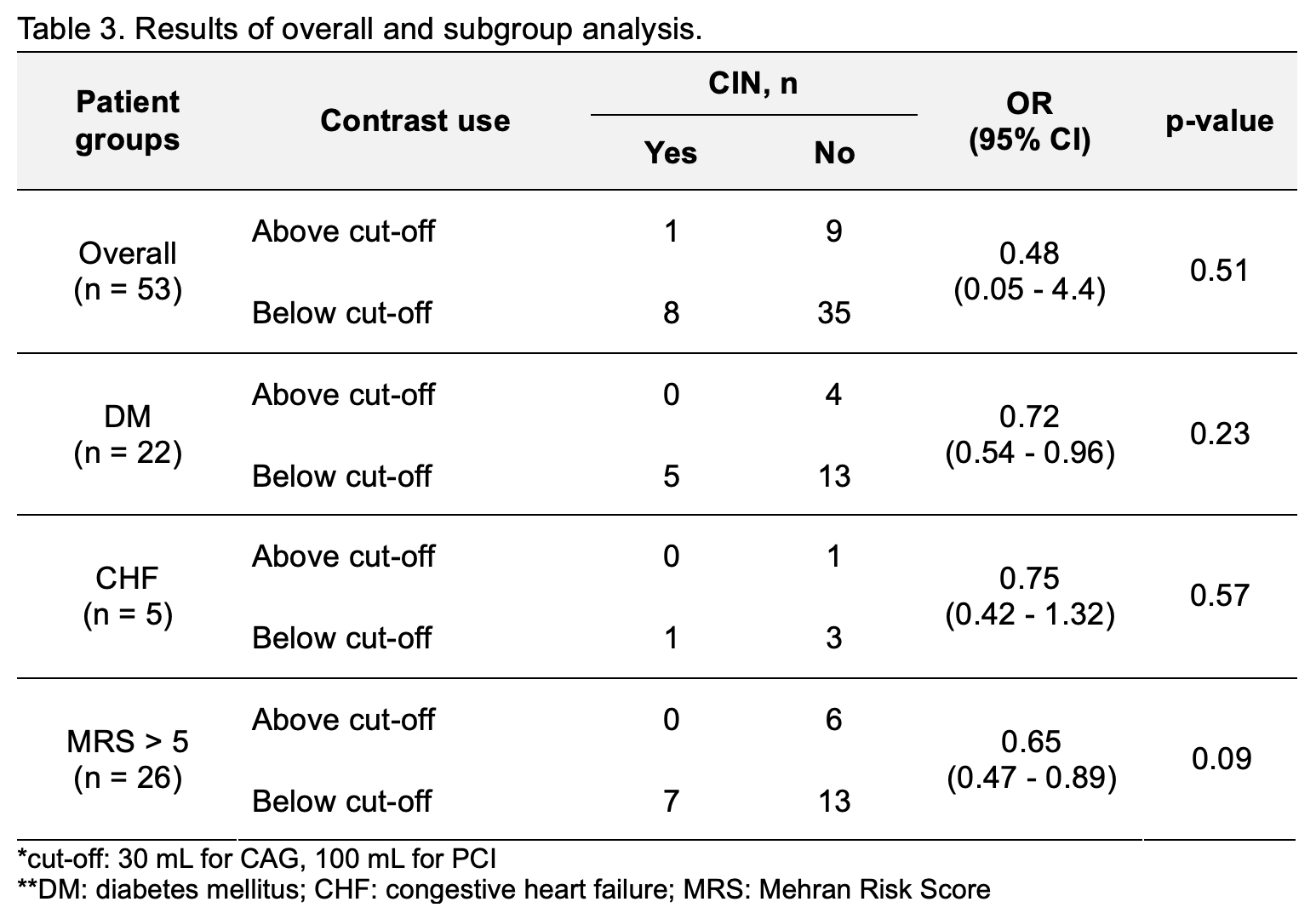
A total of 53 patients were included, of whom 69.8% were male with a mean age of 60 years. Mean contrast volume use in CAG and PCI were 22.4 mL and 45.8 mL, respectively. CIN events were highest in patients with MRS > 5. Lower mean eGFR, higher mean SrCr, and higher contrast volume were observed in patients with CIN. Higher MRS and CIN events had significant association in this study, independent of the lower contrast cut-off (p= 0.03). However, statistical analysis revealed no significant association between the lower contrast volume cut-off and CIN events across the overall population (p = 0.51), as well as in subgroups with DM (p = 0.23), CHF (p = 0.57), and those with MRS > 5 (p = 0.09).
Conclusion
The lower contrast volume cut-off is not associated with lower CIN events in CKD patients. It is more effective to consider multiple risk factors by using the Mehran Risk Score to mitigate the possibilities of CIN, rather than focusing on reducing contrast volume.