
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP A-024
Drug-Coated Balloon Enhanced MOdified JAiled Balloon (DEMOJAB) Technique - A Novel Modification of the Jailed Balloon Technique (A Case Series)
By Eran Sim, Zin Latt Ko, Michael Tanaka, An Shing Ang, Hee Hwa Ho, Jafary Fahim
Presenter
Eran Sim
Authors
Eran Sim1, Zin Latt Ko1, Michael Tanaka1, An Shing Ang2, Hee Hwa Ho1, Jafary Fahim1
Affiliation
Tan Tock Seng Hospital, Singapore1, Woodlands Health Campus, Singapore2
View Study Report
TCTAP A-024
Bifurcation
Drug-Coated Balloon Enhanced MOdified JAiled Balloon (DEMOJAB) Technique - A Novel Modification of the Jailed Balloon Technique (A Case Series)
Eran Sim1, Zin Latt Ko1, Michael Tanaka1, An Shing Ang2, Hee Hwa Ho1, Jafary Fahim1
Tan Tock Seng Hospital, Singapore1, Woodlands Health Campus, Singapore2
Background
Coronary bifurcation lesions present a significant challenge, with side branch (SB)compromise being a major complication during stenting. The jailed-balloon technique (JBT) with several modifications is well described to maintain SB patency during stenting. However, issues such as endothelial injury from SB dilation and carina shift during post-dilation have been inadequately addressed in current protocols. Modifications of JBT have aimed to reduce these risks, but many still fall short in achieving optimal SB protection. We describe a further modification utilizing drug-coated balloons (DCB), precise SB and post-dilation balloon sizing and specific timing of JB deflation to enhance SB patency.
Methods
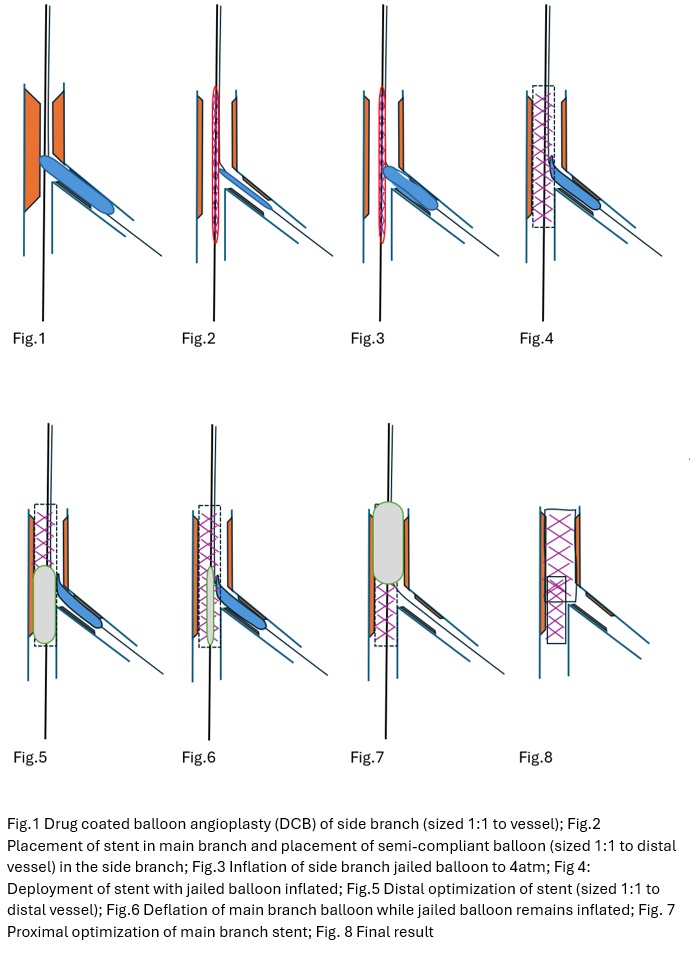
Coronary lesions were classified according to the Medina classification and considered bifurcation lesions if there was at least 50% stenosis involving the ostio-proximal segment of the SB. The novel DEMOJAB technique is as follows : (1)SB was first dilated with conventional balloons and then treated with a DCB, sized 1:1 to the SB. (2) After positioning the stent in the main branch (MB), a new semi-compliant balloon, sized 1:1 to the SB, was advanced and inflated to 4atm across the SB ostium (extending 1 to 2 mm proximally into the MB and not beyond the DCB segment in the SB (3) Stent was deployed at nominal pressure (4)Stent balloon deflated and removed but JB left inflated (5) Distal optimization of the MB stent was performed with high-pressure dilation of a non-compliant (NC)balloon sized 1:1 to the distal vessel, keeping the JB inflated (6) After removing the distal optimization balloon, JB is deflated and removed under fluoroscopic guidance (7) Final proximal optimization of the MB stent was performed with an NC balloon sized to the proximal vessel (8) Jailed SB wire removed under fluoroscopic guidance. The rational behind the described technique involving prolonged side branch jailed balloon inflation was twofold: (1) Maintenance of the carina which would have otherwise been at risk of shifting during main branch stenting. (2) occlusion of the SB with an appropriate sized jailed balloon would reduce the inherent risk of distal plaque embolization from the main branch into the side branch during main branch stenting
Results
Eight patients with coronary bifurcation lesions underwent percutaneous coronary intervention with this novel DEMOJAB technique. Four patients presented with acute coronary syndrome (ACS) while Four patients presented with stable ischemic heart disease with anginal symptoms The guider size was at least a 6Fr guide. Of the lesions intervened, five were left anterior descending (LAD) and diagonal bifurcation lesions, one was a left circumflex (LCx) and obtuse marginal bifurcation lesion, one was a posterior descending (RPD) and right posterior lateral (RPL) bifurcation lesion and one was a complex left main-LAD-LCx bifurcation lesion. SB patency with < 30% residual was maintained with TIMI3 flow in seven patients (87.5%) and no further intervention was required. One patient had a compromised side branch (diagonal) that required rewiring and subsequent kissing balloon inflation. All JBs and wires were successfully removed without damage or entrapment. No major adverse cardiac events (MACE) occurred during the hospital stay or at the one-month follow-up. Additionally, no patients reported anginal symptoms at one-month follow-up.
Conclusion
We describe a novel modification of the JBT with excellent acute and 30-day outcomes. The DEMOJAB technique appears safe, providing satisfactory SB protection during MB stenting by avoiding SB compromise from carina shift during post-dilatation. We demonstrated a high procedural success rate with little need for subsequent rewiring or KBI. Further studies with longer follow-ups are necessary to validate our preliminary findings