
Dominick J. Angiolillo
University of Florida College of Medicine, USA
Dominick J. Angiolillo, MD, recently delivered a compelling lecture on the nuances and critical considerations surrounding dual pathway inhibition (DPI).
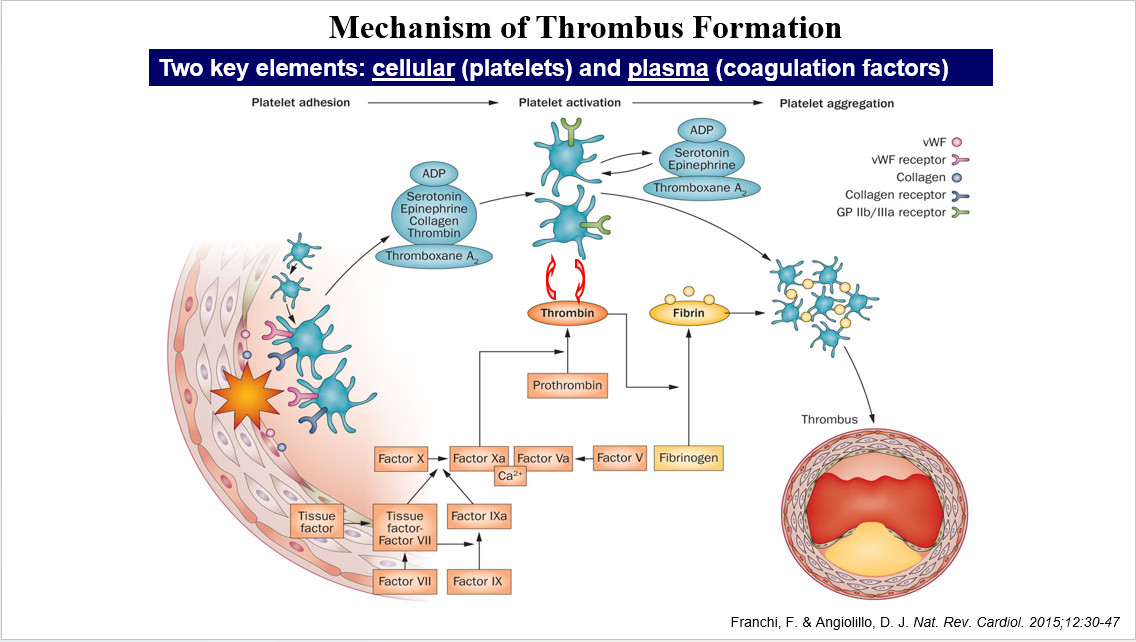
The presentation started by introducing basic concepts of thrombosis formation (Figure 1). In case of an atherosclerotic plaque rupture, two key pathways are activated; the cellular pathway represented by platelets, as well as the plasma component represented by thrombin. The surface of the activated platelets is the main source for generation of thrombin, indicating an interplay between the two mechanisms. Despite efforts to block platelet activation, thrombosis continues to occur, leading to the concept of DPI of both platelets and coagulation.
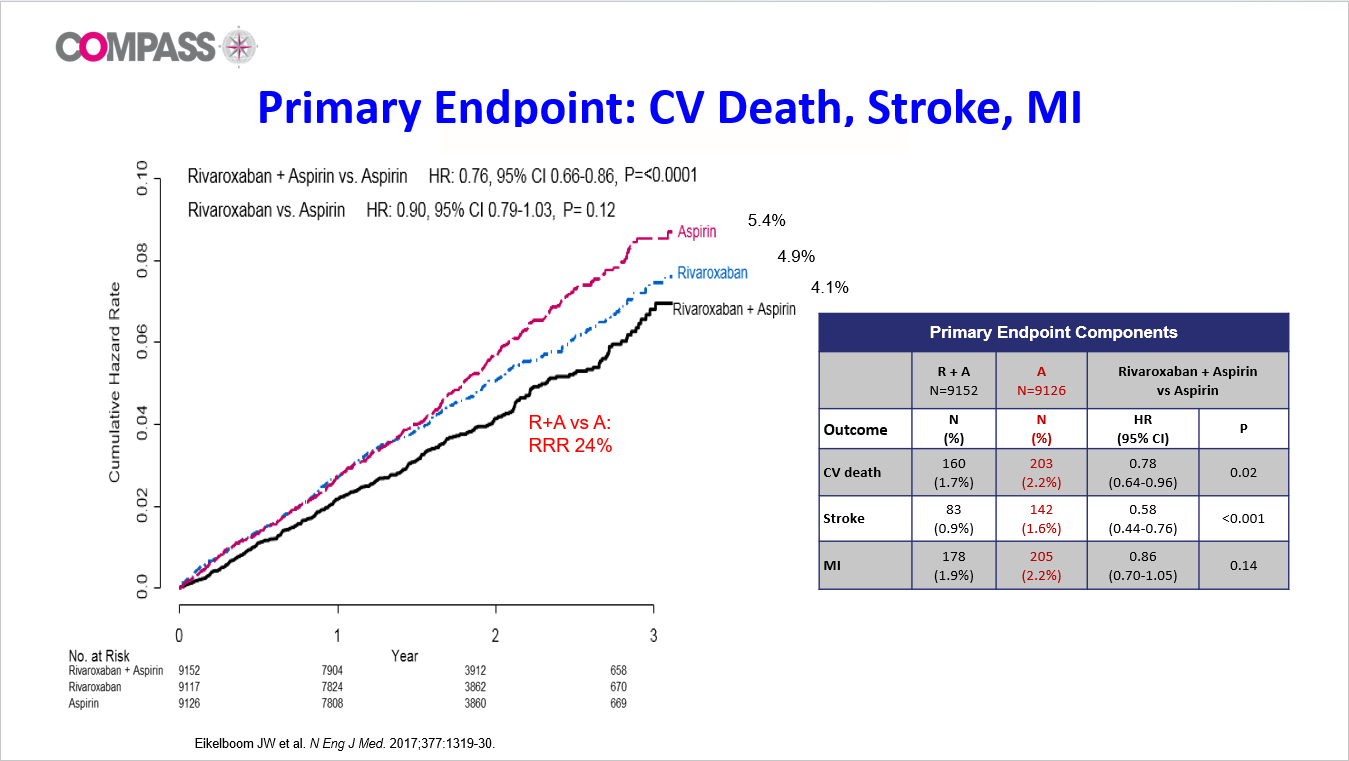
Ischemic events continue to occur even during aspirin monotherapy, and there have been some disappointments with the strategies of using alternative antiplatelet therapies. This led to a question of whether a very low-dose rivaroxaban (2.5 mg bid) in adjunct to aspirin can reduce ischemic events, which was tested in the COMPASS trial (Figure 2). The landmark COMPASS trial examined nearly 30,000 patients to determine the efficacy of adding low-dose rivaroxaban to aspirin therapy. Results from this trial indicated a significant decrease in ischemic events when using the combined DPI strategy versus aspirin alone, reshaping long-term secondary prevention tactics for patients with stable coronary and peripheral artery disease (CAD and PAD).
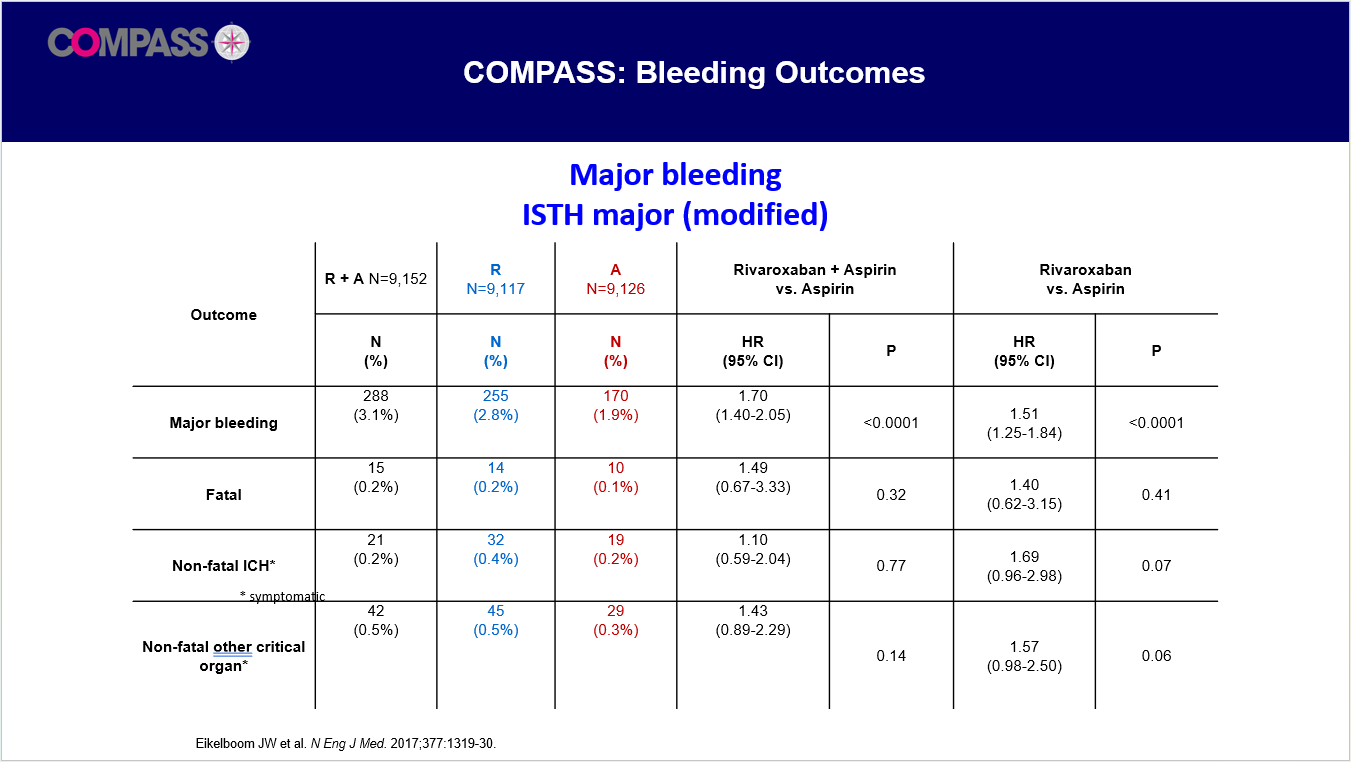
Despite these promising outcomes, the inherent risks associated with DPI were also addressed, which is an increased incidence of major bleeding events (Figure 3). This aspect remains a crucial consideration in clinical decision-making, emphasizing the need for careful patient selection based on individual risk profiles.
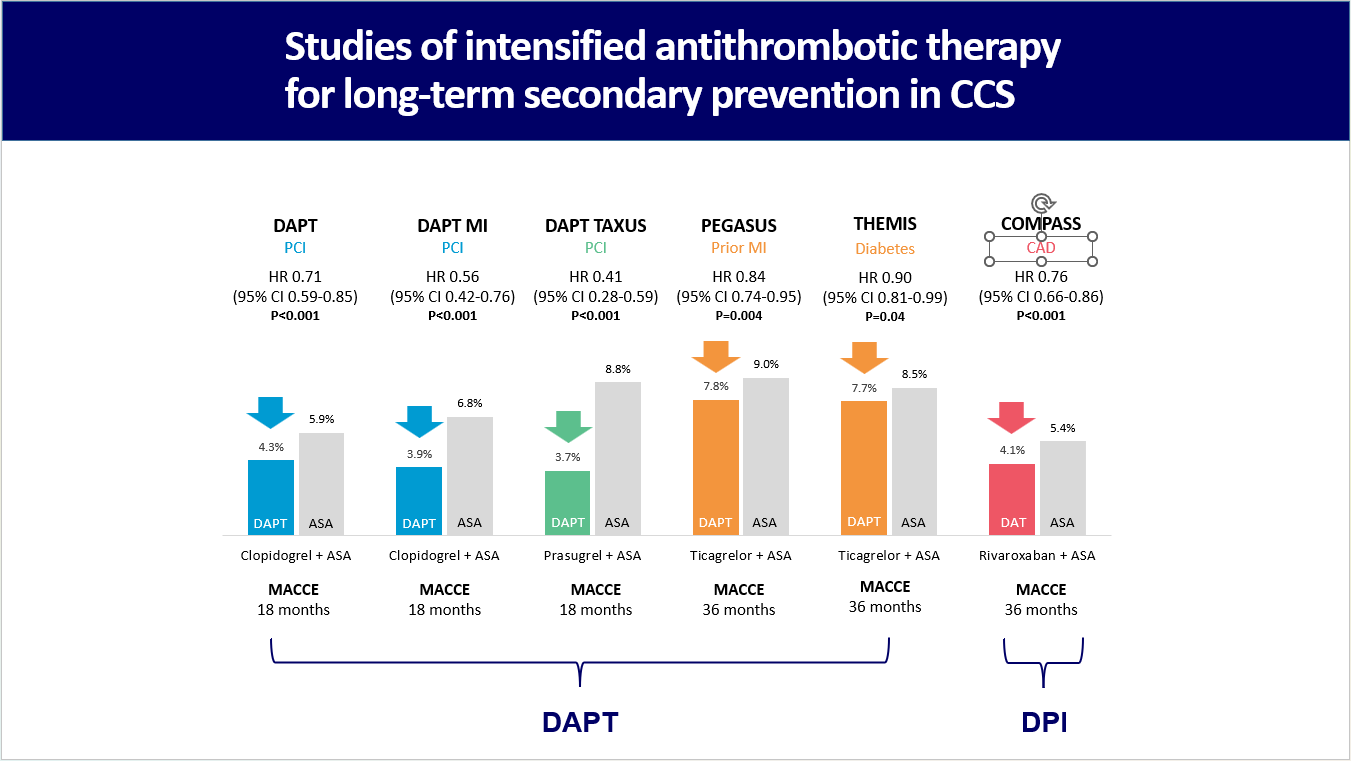
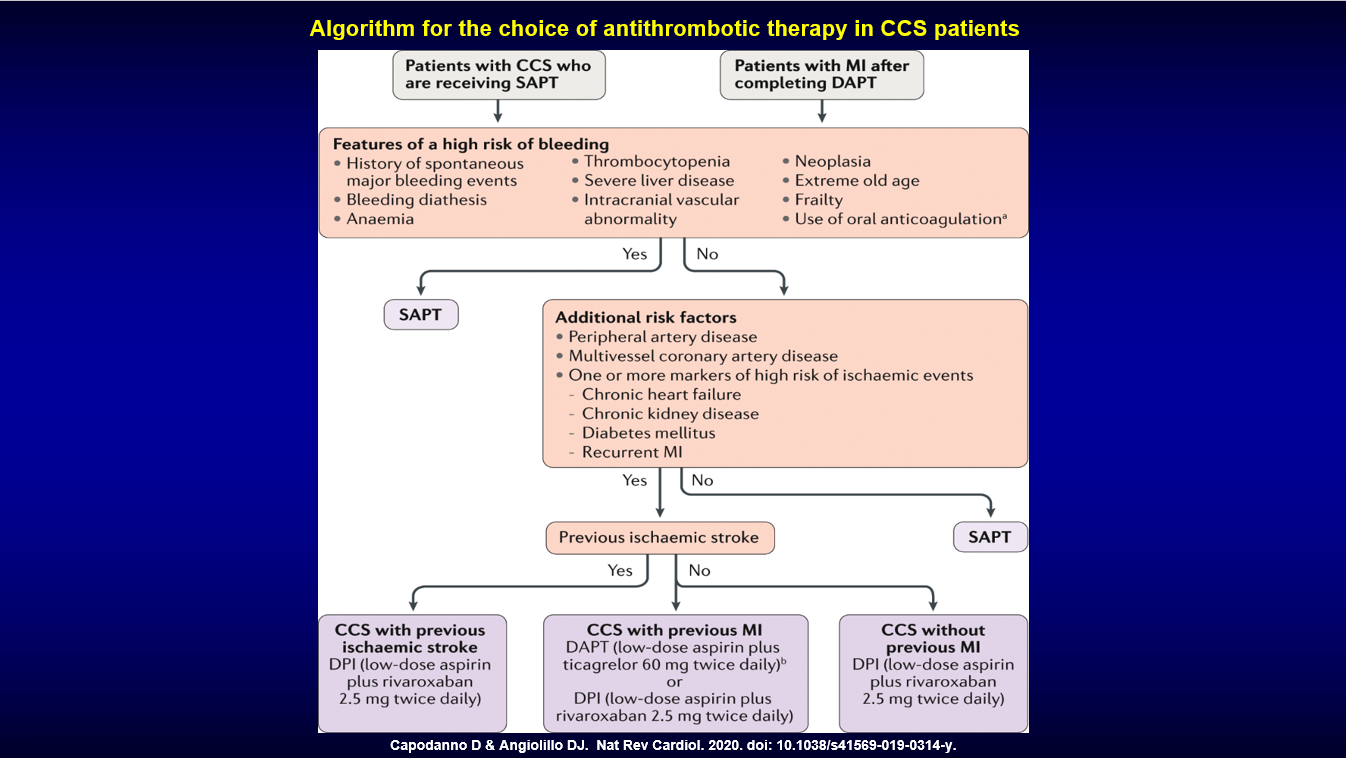
Studies on intensified antithrombotic therapy for long-term secondary prevention in patients with chronic coronary syndrome were highlighted (Figure 4), and the lecture concluded with a detailed algorithm to aid physicians in selecting the appropriate therapeutic strategy, considering factors such as high-risk features of both bleeding and ischemic events, including multivessel coronary disease, chronic kidney disease, diabetes, recurrent myocardial infarctions, and history of prior ischemic stroke (Figure 5).
Hot Topics
All About New Data of Antithrombotics
Friday, April 26, 4:40 PM ~ 6:06 PM
Presentation Room 1, Level 1
Edited by

Hoyun Kim, MD
Bucheon Sejong Hospital, Korea (Republic of)