
Jinho Lee
Kyung Hee University Hospital, Republic of Korea
A recent post-hoc analysis of the BEST extended follow-up study shed new light on the efficacy of intravascular ultrasonography (IVUS) guided percutaneous coronary intervention (PCI) with everolimus-eluting stents (EESs) compared to bypass surgery for patients with multivessel coronary artery disease (CAD). Previous research (IVUS-XPL, ULTIMATE, and RENOVATE-COMPLEX-PCI trials) has shown that intravascular imaging-guided PCI improves clinical outcomes compared to coronary angiography (CAG)-guided PCI for cases of complex CAD. While both the American and European guidelines recommend IVUS-guided PCI as a class IIa intervention, coronary artery bypass grafting (CABG) remains the preferred option for patients with multivessel CAD, due to its perceived survival advantage. To address the question of whether the improved outcomes associated with IVUS-guided PCI could challenge the status of CABG in multivessel CAD, the researchers conducted an analysis of patient data from the BEST extended trial.
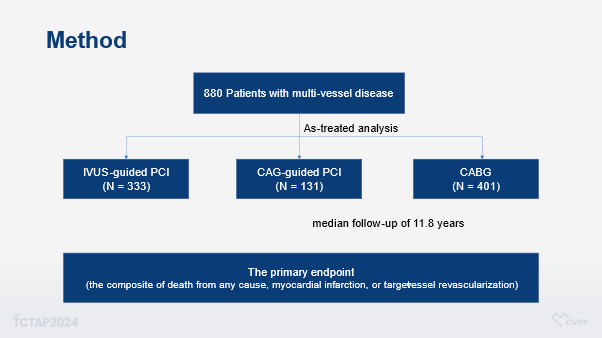
This prospective, open-label, multicenter, randomized trial enrolled a total of 880 patients with multivessel disease over a 5-year period, randomly assigning them to either PCI with EESs or CABG. The median follow-up period was 11.8 years. The total patient population was categorized according to their treatment modalities into 3 groups: IVUS-guided PCI, CAG-guided PCI, and CABG (Figure 1). The primary endpoint was a composite of death from any cause, myocardial infarction, or target-vessel revascularization.
Notably, the CABG group had a higher rate of three-vessel disease, while the IVUS-guided PCI group had a higher incidence of two-vessel disease. Procedural characteristics varied across the groups, with complete revascularization more frequently achieved in the CABG group. However, the IVUS-guided PCI group had a longer total stent length and a larger stent diameter compared to the angiography-guided PCI group.
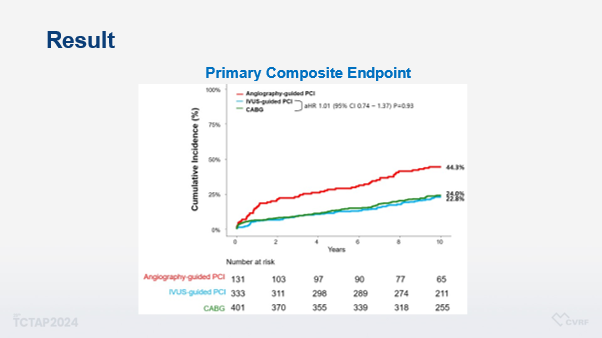
Analyses of the primary composite endpoint and other key outcomes revealed that the IVUS-guided PCI group and the CABG group had similar event rates, both lower than the angiography-guided PCI group (Figure 2). Multivariable analysis adjusted for baseline imbalances confirmed these findings, indicating that IVUS-guided PCI is a safe and effective alternative to CABG for patients with multivessel disease.
In conclusion, the study advocates a routine use of intravascular imaging during PCI for multivessel CAD, suggesting that IVUS-guided PCI offers comparable outcomes to CABG.
Clinical Science
All About New Data from Asan Medical Center
Saturday, April 27, 10:05 AM ~ 11:25 AM
Presentation Room 1, Level 1
Edited by
Jinho Lee, MD
Kyung Hee University Medical Center, Korea (Republic of)