
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-031
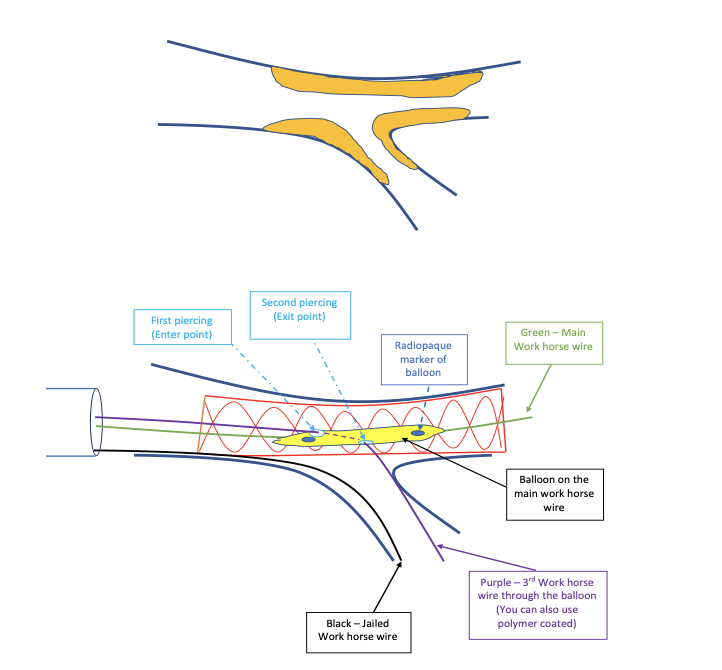
Home-Made Dual Lumen ‘Microcatheter’ – Pierced Balloon Assist Technique for Bifurcation and CTO Lesions
By Najmiddin Makhkamov, Javokhir Anvarov, Rustem Dautov
Presenter
Najmiddin Makhkamov
Authors
Najmiddin Makhkamov1, Javokhir Anvarov1, Rustem Dautov2
Affiliation
Fedorovich Klinikasi LLC, Uzbekistan1, The Prince Charles Hospital, Australia2,
View Study Report
TCTAP C-031
Coronary - Complex PCI - Bifurcation
Home-Made Dual Lumen ‘Microcatheter’ – Pierced Balloon Assist Technique for Bifurcation and CTO Lesions
Najmiddin Makhkamov1, Javokhir Anvarov1, Rustem Dautov2
Fedorovich Klinikasi LLC, Uzbekistan1, The Prince Charles Hospital, Australia2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Patient history: 49 years old male with history of previous PCI of left anterior descending (LAD), left circumflex (LCX) and right coronary artery (RCA), hypertension, dyslipidemia was admitted to our hospital with unstable angina.


Relevant Test Results Prior to Catheterization
Echo: mild left ventricular (LV) wall hypertrophy with hypokinesis in the lateral wall and decreased longitudinal strain. LV ejection fraction was 41%.
Relevant Catheterization Findings
Coronary angio: severe bifurcation stenosis (Medina 1:1:1) of left main (LM), LAD and LCX arteries.
Interventional Management
Procedural Step
Considering the angle of origin of the LCx, we reached a consensus to do PCI utilizing TAP technique. Two Sion Blue guidewires (Asahi Intecc, Japan) were placed to LAD and to LCx. After preparation of the arteries with predilatation, 3.0x24 mm Stent - LM to LAD was implanted. The next step must be the proximal optimization technique (POT) to prevent inadvertent crossing with the 3rd guidewire under malapposed stent struts. At the same time, the distal strut crossing is also very important in TAP bifurcation technique to achieve a better neocarina result. However, sometimes we observe a plaque shift after provisional stent implantation and even POT may not resolve the situation. After the stent implantation, we decided to change our strategy and the next step was to cross the distal strut with 3rd guidewire. A DLMC is not available in our country. At that time, we thought that the “sidecar technique” could be useful, but unfortunately, there would be no support after taking out the guidewire from the co-transporter (balloon). So, we created a home-made ‘microcatheter’ with dual piercing of regular 2.0x15mm SC balloon catheter which was successfully used to pass the 3rd guide wire from the true lumen of malapposed stent in LM to cross LCx from the distal strut with a better support, similar to one from a dual-lumen microcatheter.

Case Summary
1. This technique allows (as an alternative to dual-lumen microcatheters) successful wiring of distal struts or side branches with better support of guidewire, while at the same time reducing the wire twisting.2. For variety of reasons, DLMCs are not available in every geography. Our home-made technique of utilizing a standard pierced balloon, as a substitute to DLMC in bifurcations and CTO PCI represents a cheap alternative that operators may easily try in complex PCI cases.3. Dual-lumen microcatheters are useful, and sometimes essential, in certain situations encountered in complex coronary interventions. We have described modification of recently.