
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-160
Double-Edged Sword Situation in a Post-PCI Patient: A Case Report
By Abeeda Tasnim Reza, Kazi Atiqur Rahman, Shahab Uddin Talukder, A. Q. M. Reza, AHM Waliul Islam, Aparajita Karim, Poppy Bala, Azfar Hossain Bhuiyan, Sadeed Araf Reza
Presenter
Abeeda Tasnim Reza
Authors
Abeeda Tasnim Reza1, Kazi Atiqur Rahman1, Shahab Uddin Talukder1, A. Q. M. Reza1, AHM Waliul Islam1, Aparajita Karim1, Poppy Bala1, Azfar Hossain Bhuiyan1, Sadeed Araf Reza2
Affiliation
Evercare Hospital Dhaka, Bangladesh1, Sir Salimullah Medical College, Bangladesh2,
View Study Report
TCTAP C-160
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Double-Edged Sword Situation in a Post-PCI Patient: A Case Report
Abeeda Tasnim Reza1, Kazi Atiqur Rahman1, Shahab Uddin Talukder1, A. Q. M. Reza1, AHM Waliul Islam1, Aparajita Karim1, Poppy Bala1, Azfar Hossain Bhuiyan1, Sadeed Araf Reza2
Evercare Hospital Dhaka, Bangladesh1, Sir Salimullah Medical College, Bangladesh2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 51-year-old lady, a known case of diabetes, hypertension, hypothyroidism & end stage renal disease on maintenance hemodialysis, presented with the complaints of shortness of breath and exertional chest discomfort for 8 hours. She was a renal transplant candidate. On physical examination, her heart rate was 96 beats per minute, blood pressure 170/80 mm of Hg. On auscultation, there was bilateral basal crepitations in her both lung fields.

Relevant Test Results Prior to Catheterization
Her high sensitivity-troponin I was raised, serum creatinine was 7.21 mg/dl, serum urea 130 mg/dl, hemoglobin 9.7 gm/dl & calculated e-GFR was 6 ml/min/1.73 m2.
Relevant Catheterization Findings
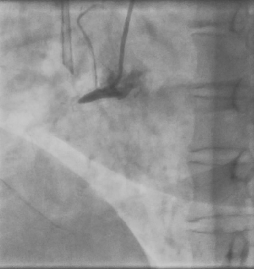
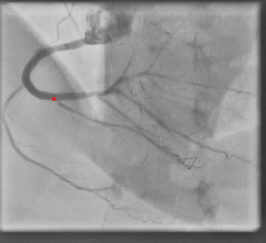
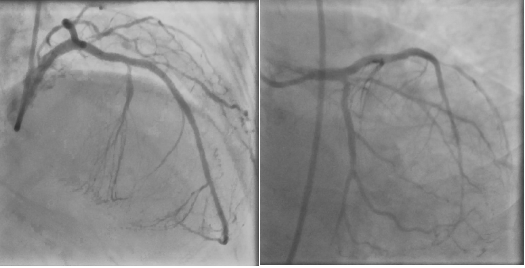
She underwent coronary angiogram which showed triple vessel coronary artery disease with 90% lesion in left anterior descending artery, significant stenosis of proximal segment of diagonal branch & 70-80% lesion in left circumflex artery. Her right coronary artery was 100% occluded form its proximal segment with collaterals arising from the left coronary.


Interventional Management
Procedural Step
We took a heart team approach. After counselling with the patient and a discussion with a nephrologist, we decided to go for PCI. First, we took a cine of RCA by contralateral dual injection. J-CTO score was 2. Then RCA was wired by antegrade wire escalation. A run-through intermediate wire crossed the lesion with the help of a microcatheter. After adequate pre-dilatation, a 2.75X38 mm DES was deployed in distal RCA & another 3.5X32 mm DES was deployed in proximal to mid RCA. After adequate post dilatation, RCA showed TIMI-III flow. Subsequently, a 3X48 mm DES was deployed in proximal to mid LAD & another 2.5X28 mm DES was deployed in LCX. Her in-hospital stay was uneventful, and she was discharged on 4th day on dual antiplatelet (Aspirin and Clopidogrel). She was doing well on her follow-up after 2 weeks. But on 28th day of her PCI, she again got admitted through ER with fever, gum bleeding and multiple bruises all over the body for 4 days. She was diagnosed as a case of Dengue fever with severe thrombocytopenia. That was a double-edged sword situation. Her platelet count was 40,000/micro liter, which decreased up to 20,000/micro liter. Dual Antiplatelets were stopped immediately after hospitalization. Fresh frozen plasma and apheresis platelet were transfused. We monitored her platelet count regularly. After 7 days, when her count was increased to 1,00,000/micro liters, we first started clopidogrel and after 2 days, aspirin. She had been doing well since then.

Case Summary
An end stage renal disease patient with high bleeding risk along with dengue fever and recent angioplasty was a difficult scenario for an interventional cardiologist. Proper counselling, assurance, diagnosis and treatment of underlying cause along with proper drug treatment are required to tackle such double-edged sword situation.