
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-080
A Challenging Case Report: Retrograde Approach to Overcome Long CTO
By ChaoWen Hsueh
Presenter
ChaoWen Hsueh
Authors
ChaoWen Hsueh1
Affiliation
China Medical University Hsinchu Hospital, Taiwan1,
View Study Report
TCTAP C-080
Coronary - Complex PCI - CTO
A Challenging Case Report: Retrograde Approach to Overcome Long CTO
ChaoWen Hsueh1
China Medical University Hsinchu Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 65 year-old male came to our hospital due to chest tightness on exertion for weeks. His two older brothers also had coronary artery and took PCI before.
Past history :
Coronary artery disease s/p PCI years ago
Dyslipidemia
Cath history
2008/11
LCx M/3-D/3: Taxus Liberte' 3.0/28, 2.75/28mm
OM1: Taxus Literte' 3.0/16mm
LAD P/3-M/3: Taxus Liberte' 2.75/28, 2.5/16mm
RCA D/3 to PDA: Taxus Literte' 2.75/32mm
2013/8
Diffuse ISR: POBA

Relevant Test Results Prior to Catheterization
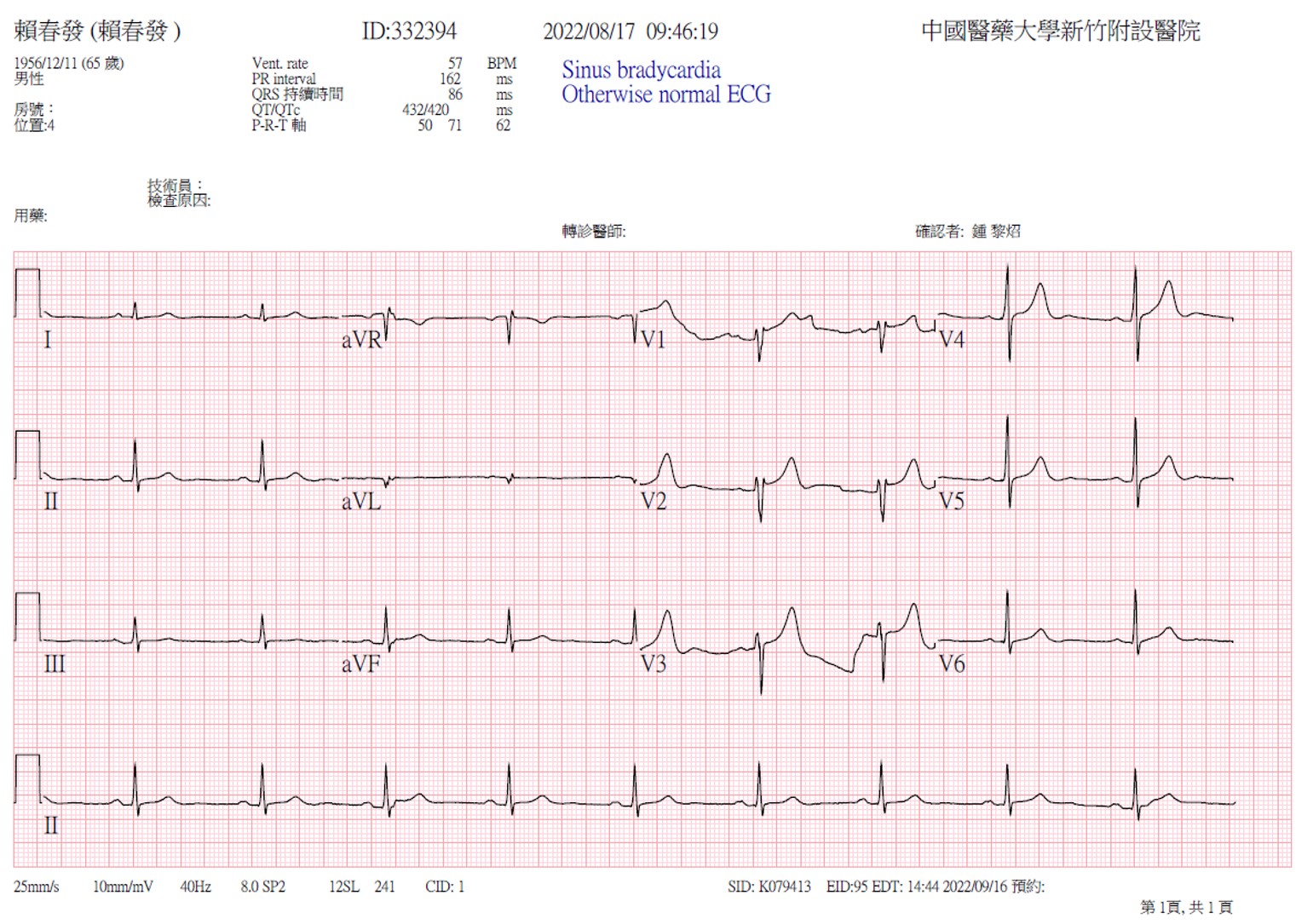
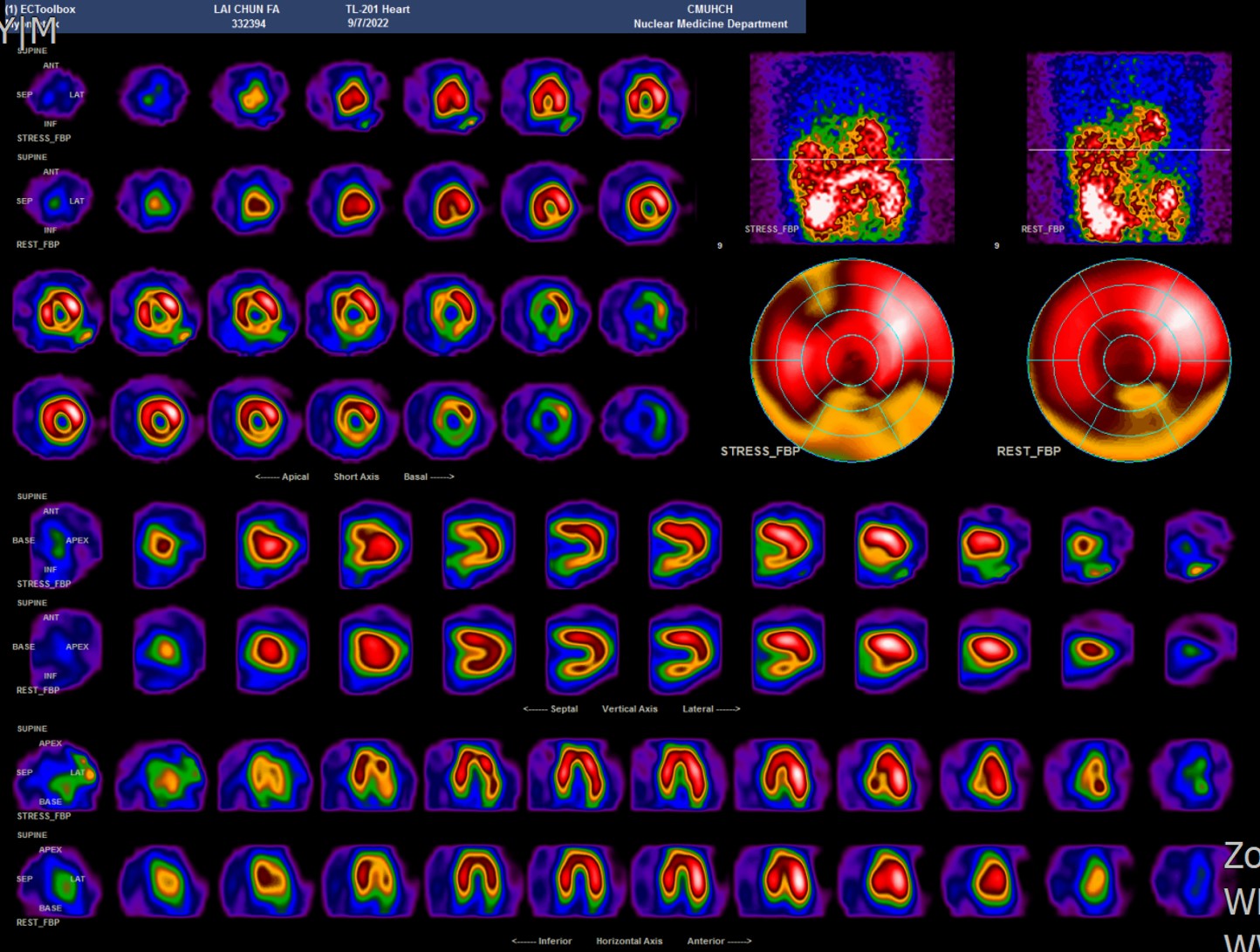
Thallium 201 scan was arrange and the result showed strong positive.ECG showed no specific findings
Relevant Catheterization Findings
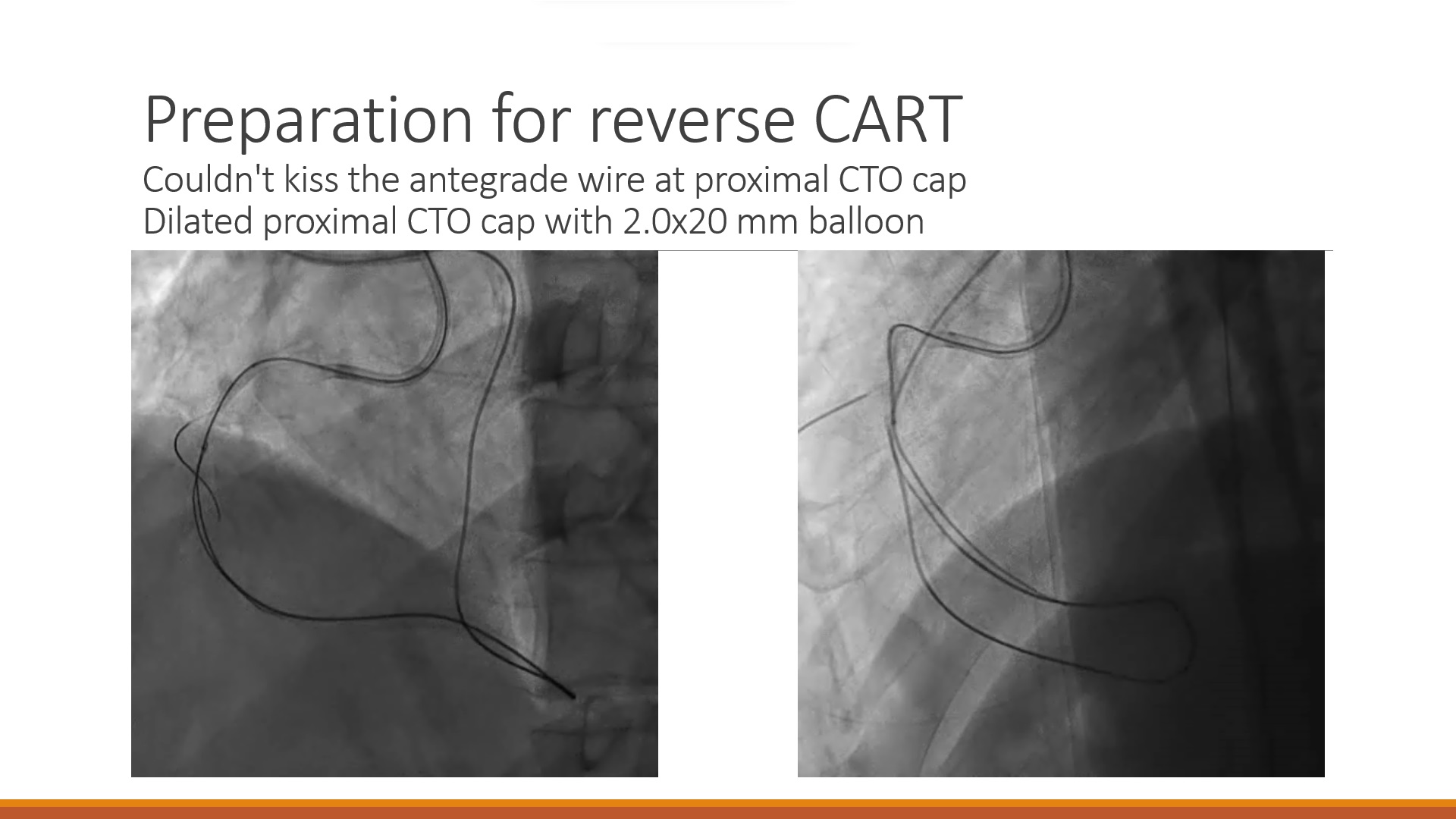
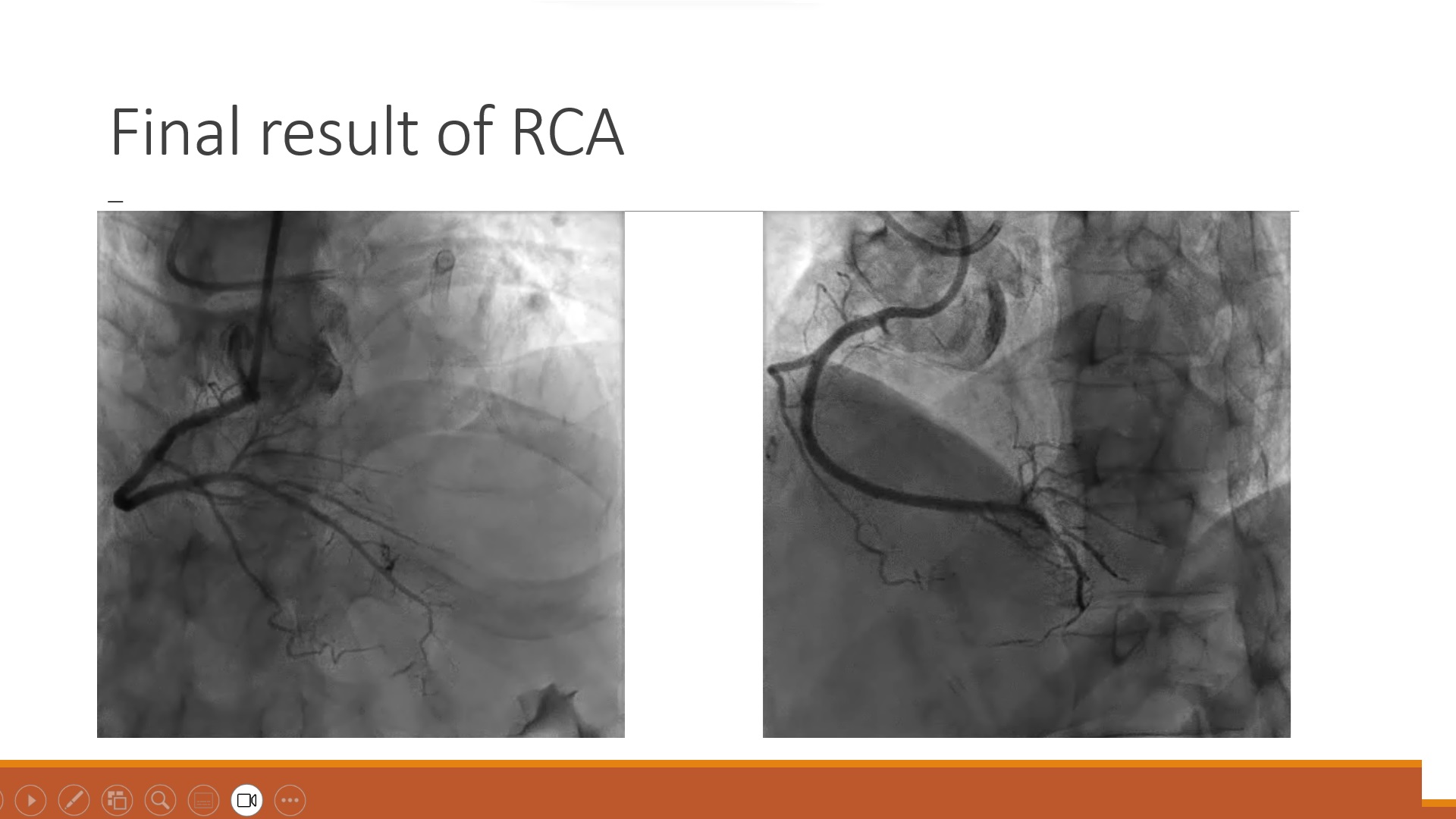
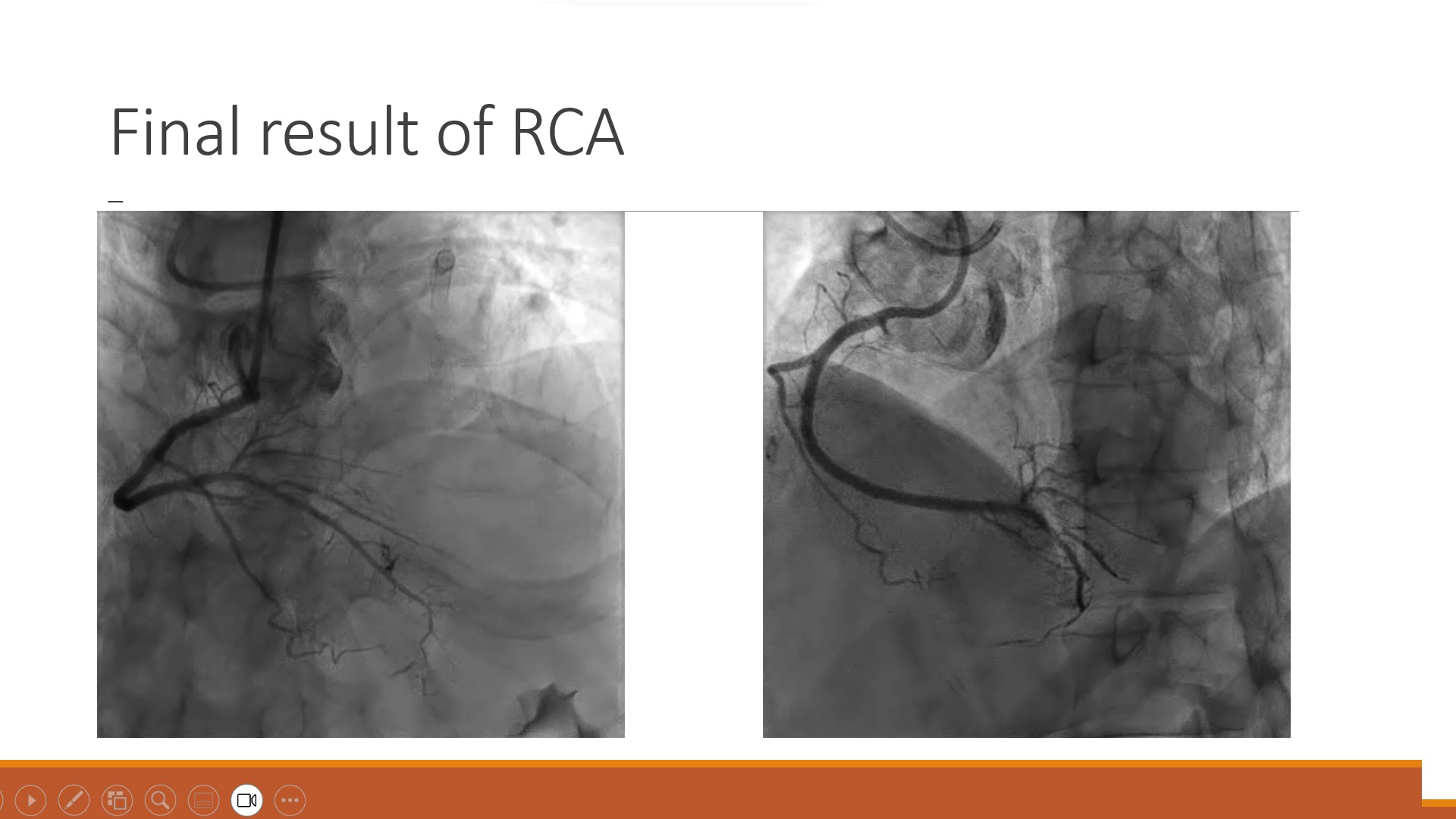
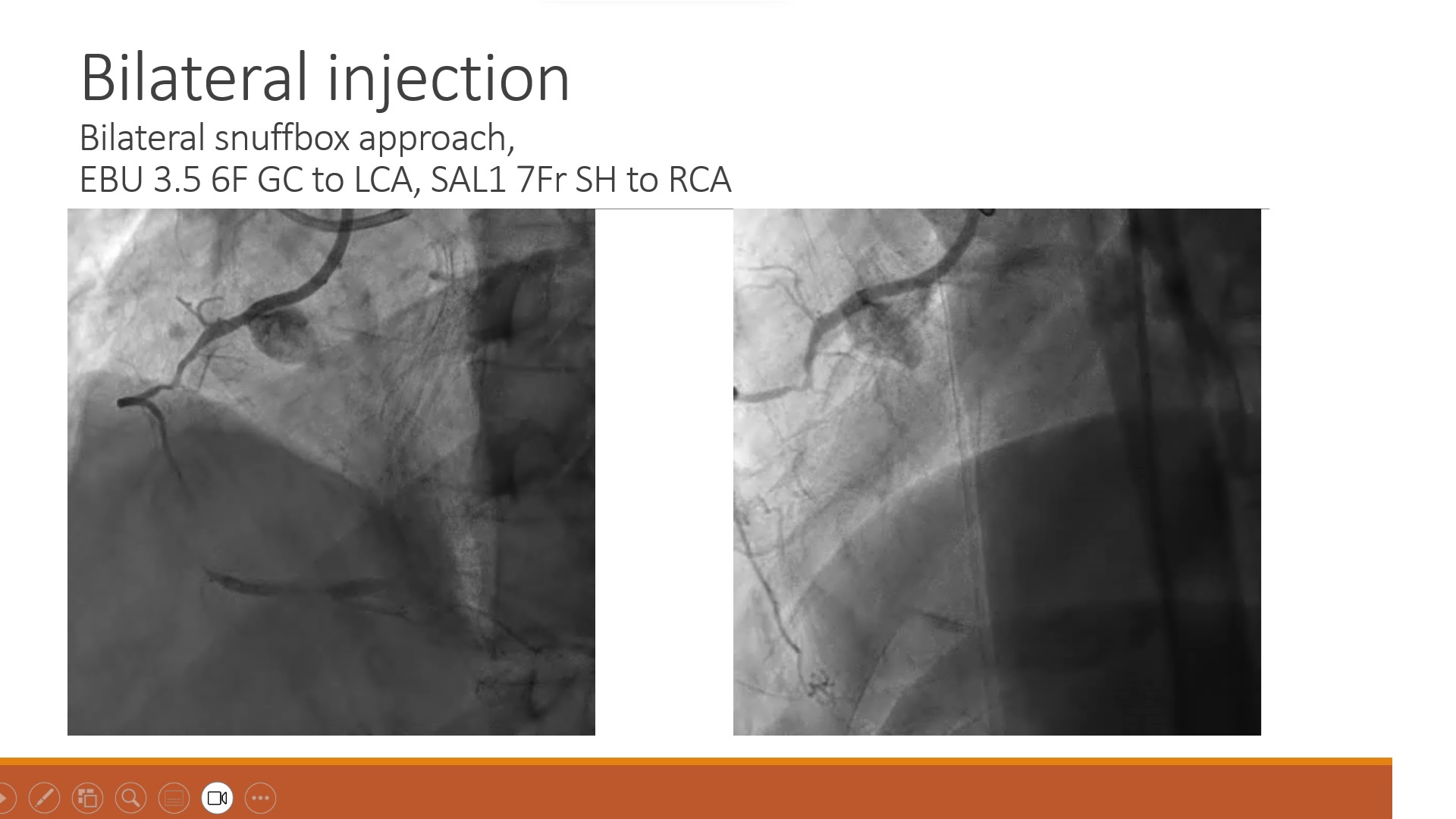
Retrograde approach:Sion wire with broken-tip, loaded in Corsair Pro MC 150cm, was advanced into the 4th septal branch. Suoh03 wire reached PDA and m-RCA. Gaia II wire entered CTO body. Reverse CART proximal CTO cap was dilated. Retrograde Gaia II wire successfully crossed CTO, proximal RCA and reached aorta. Guideliner extension catheter was not used after successfully advancing retrograde Gaia II wire into antegrade. RG3 300cm Wire externalization was achieved.

Interventional Management
Procedural Step
2. Retrograde approach:

Case Summary
Septals in retrograde PCI is the most frequently used in retrograde PCI for CTO’s of LAD or RCA. In most cases, the septal is much straight forward course than epicardial channels. Variable channel size & diameter is often obtained. However the septals could be very tortuous too. Dry tamponade could be happened.