
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-097
The Story of Left Main
By Mohsin Ahmed, Shohely Binte Mostafa
Presenter
Shohely Binte Mostafa
Authors
Mohsin Ahmed1, Shohely Binte Mostafa2
Affiliation
National Institute of Cardiovascular Diseases, Bangladesh1, Rangpur Medical College and Hospital, Bangladesh2,
View Study Report
TCTAP C-097
Coronary - Complex PCI - Left main
The Story of Left Main
Mohsin Ahmed1, Shohely Binte Mostafa2
National Institute of Cardiovascular Diseases, Bangladesh1, Rangpur Medical College and Hospital, Bangladesh2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Patient Profile45-year-oldMaleHypertensiveDyslipidemia
Chief ComplaintsExertional chest discomfort, CCS Class III
S/P-PCI to RCA (2014)Re-look CAG done in 2018 showing Mild LM disease with mild LAD ostial diseaseOn Antiplatelet & anti-ischemic medications
Physical ExaminationsPulse: 80/min Blood Pressure: 130/70 mm-HgRespiratory Rate: 15/minSPO2 : >96% in room air

Chief ComplaintsExertional chest discomfort, CCS Class III
S/P-PCI to RCA (2014)Re-look CAG done in 2018 showing Mild LM disease with mild LAD ostial diseaseOn Antiplatelet & anti-ischemic medications
Physical ExaminationsPulse: 80/min Blood Pressure: 130/70 mm-HgRespiratory Rate: 15/minSPO2 : >96% in room air
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
Interventional Management
Procedural Step
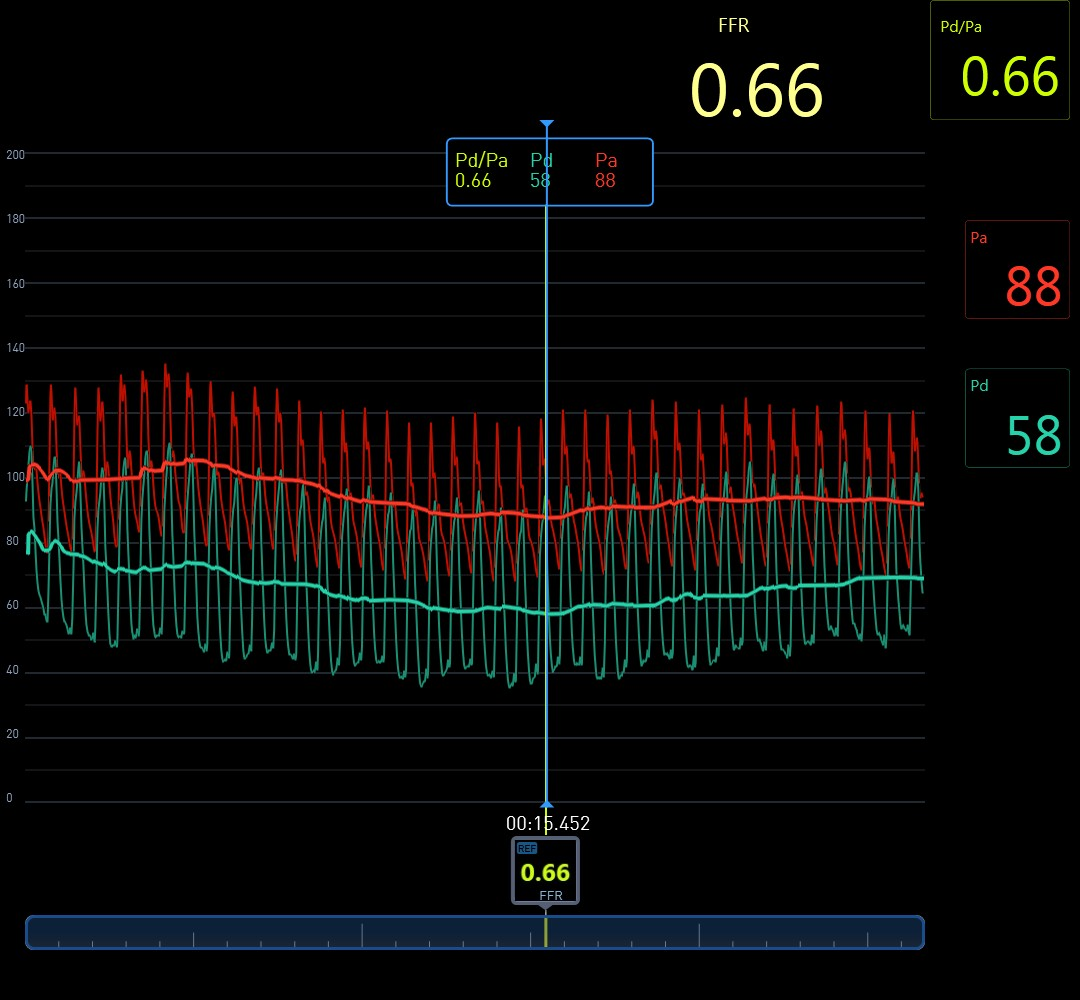
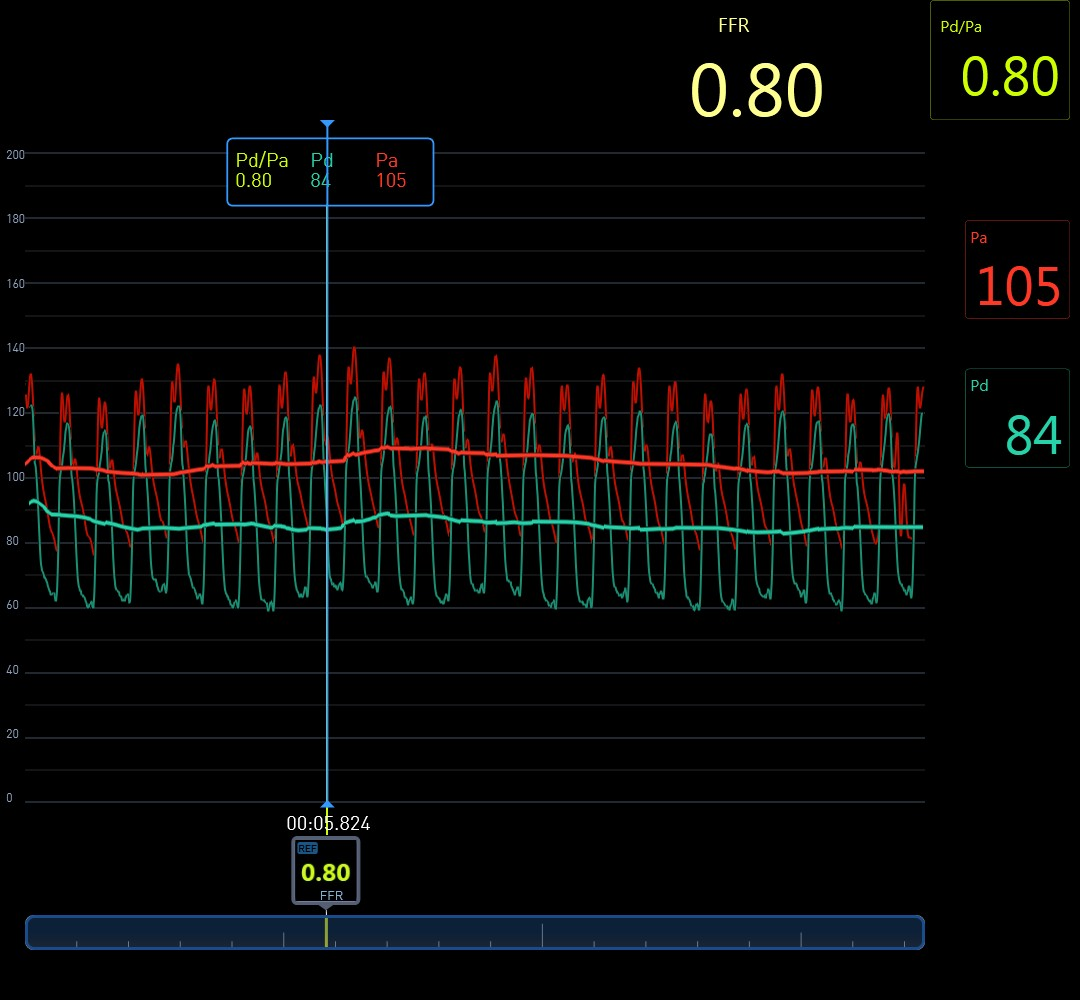
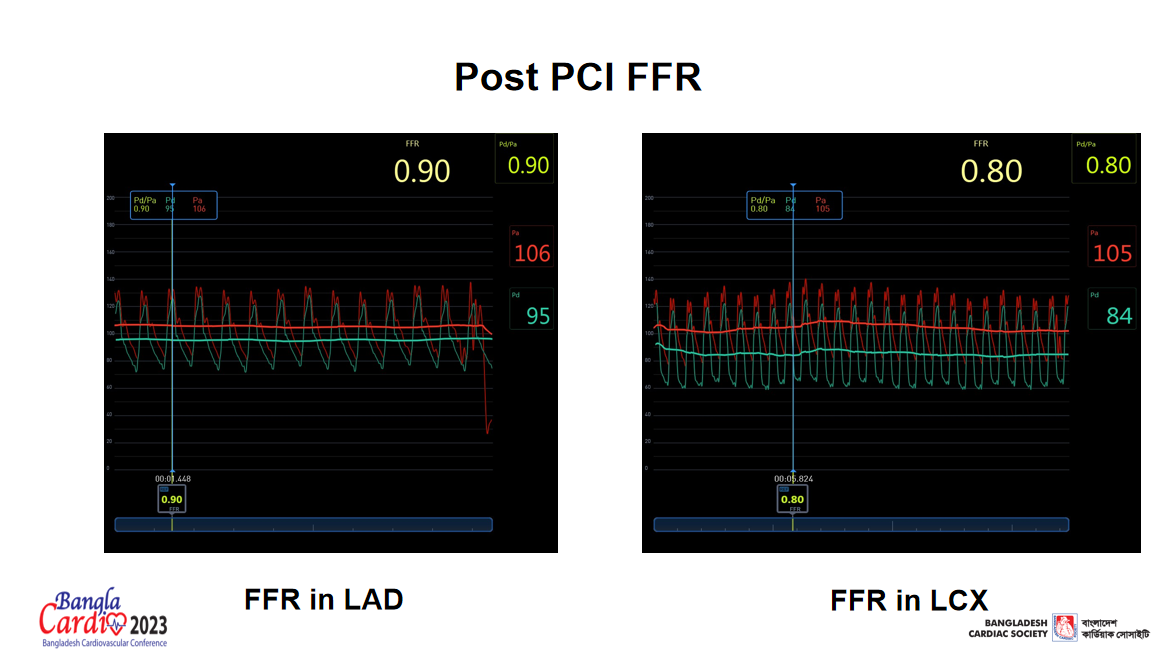
LAD engaged with XB-3.5 (7F). Wiring of both LAD & LCX done.Pre-dilatation (2.5x15 mm NC Balloon) at 10-12 atm.After Pre Dilatation.Left Main-LAD: 3.5x23 mm DES, 12-16 atm.Left Main-LAD: 3.5x23 mm DES, 12-16 atmLeft Main-LAD: 3.5x23 mm DES, 12-16 atmPost Dilatation (4x10 mm NC Balloon) At 12-18 ATM.POT.Final Cine.Post PCI FFR.Patient symptomatic on optimal medical therapy.Re-look CAG shows Intermediate lesion.FFR in proximal LAD.FFR in proximal LCX.Physiology Guided PCI: Current Status.
Case Summary
When invasively assessing intermediate coronary disease, there is more to it than meets the eye.
Visual interpretation of the coronary angiogram is insufficient
Determining FFR provides information regarding the contribution of epicardial coronary disease to myocardial ischemia
Both anatomic & physiologic assessment will guide to optimal management.