
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-173
IVUS-Guided Wire Tracking Strategy in Extensive Hematoma From Sub-Intimal Wiring in STEMI
By Rachel Ann Wong Denila, Jhoanna Marcelo
Presenter
Rachel Ann Wong Denila
Authors
Rachel Ann Wong Denila1, Jhoanna Marcelo1
Affiliation
Philippine Heart Center, Philippines1,
View Study Report
TCTAP C-173
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
IVUS-Guided Wire Tracking Strategy in Extensive Hematoma From Sub-Intimal Wiring in STEMI
Rachel Ann Wong Denila1, Jhoanna Marcelo1
Philippine Heart Center, Philippines1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
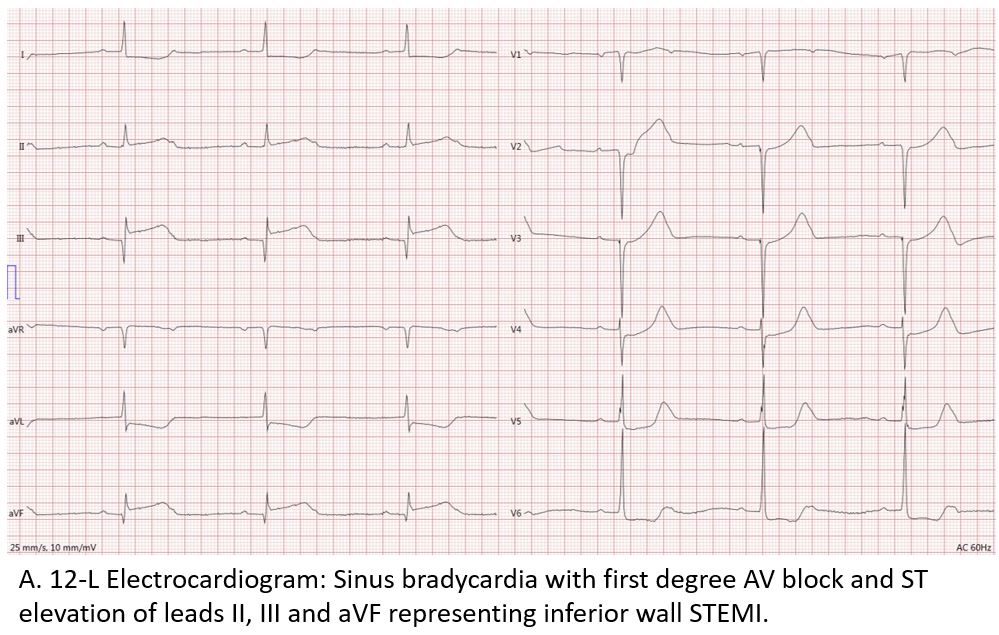
A 66- year old female, hypertensive and diabetic, was seen at the emergency room twenty-four hours from index chest pain. She was examined with ongoing chest pain and bradycardic. No murmur was appreciated. 12-lead electrocardiogram showed sinus bradycardia with first degree AV block and ST elevation in leads II-III and AVF. Baseline HS-troponin level was high (39,100 ng/L). The patient was then referred to the cardiac catheterization laboratory for primary percutaneous coronary intervention.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
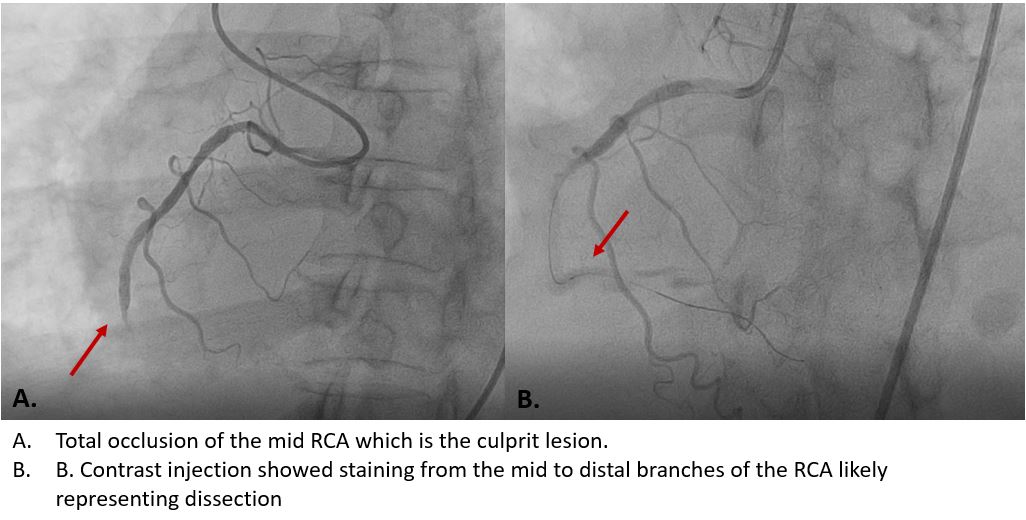
Coronary angiogram showed 3-vessel disease involving the proximal LAD, distal LCX and RCA. The RCA which was the culprit lesion was totally occluded at the midsegment. Initial wiring was done using Sion Blue. There was difficulty in wiring the RCA and wire was changed to Sion, Whisper, and eventually Fielder XT-R which was distalized to the level of the crux. However, there was note of staining from the mid to distal branches during wire manipulation which probably represents dissection.
Interventional Management
Procedural Step
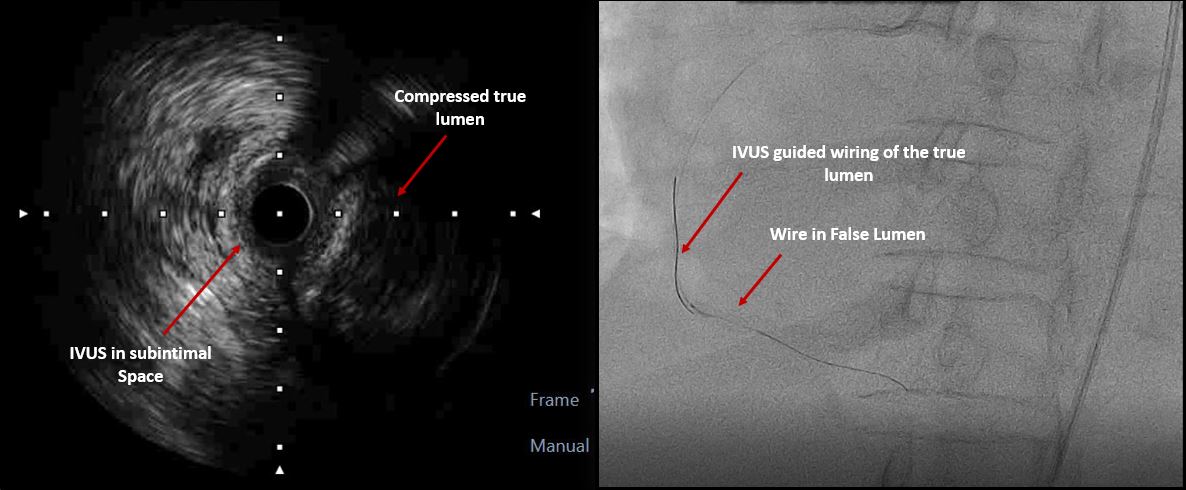
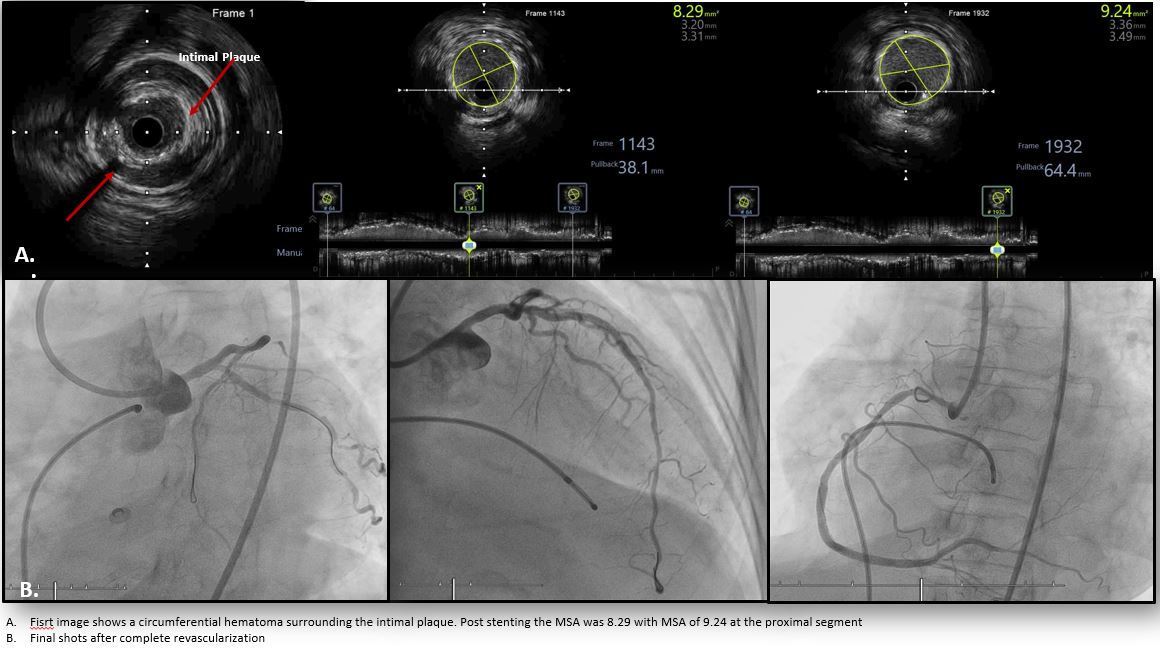
Intravascular ultrasound (IVUS) showed the wire at the sub-intimal space with dissection from the mid RCA with extensive hematoma compressing the true lumen. The first wire was left in place with the IVUS tip at the false lumen. A second wire (GAIA Next First) was then advanced and used to puncture the true lumen using IVUS guidance. Another IVUS run showed the first wire at the sub-intimal space with the second wire now at the true lumen. The IVUS catheter was able to advance up to the distal segment. Balloon inflation was done and the distal vessels were visualized during contrast injection. Another IVUS run showed an extensive circular hematoma at the distal segment. Stents were then deployed at the mid to distal segments with optimization of deployment done with IVUS guidance. Contrast injection showed TIMI 3 flow and final IVUS run showed well expanded and apposed stents with no edge dissection. Complete revascularization was done prior to discharge.

Case Summary
IVUS enhances the ability to identify the exact location of guidewires within an artery and discriminates between the true and false lumen and identifies the intimal and medial layers. Extensive hematoma can compress the true lumen which cannot be observed by angiography. In cases of extensive dissection and hematoma, IVUS guided wiring can facilitate penetration of the true lumen leading to a favorable outcome especially in emergency cases and as bail-out for complications.