
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-069
Conquered Unattainable to Attainable Lipton R-III Right Coronary Artery Chronic Total Occlusion to Reprieve My Patient
By Ankit Gupta, Bhushan Shah, Sreenivas Reddy S.
Presenter
Ankit Gupta
Authors
Ankit Gupta1, Bhushan Shah2, Sreenivas Reddy S.3
Affiliation
All India Institute of Medical Sciences, India1, All India Institute Of Medical Sciences Bhopal, India2, Post Graduate Institute of Medical Education and Research, India3,
View Study Report
TCTAP C-069
Coronary - Complex PCI - CTO
Conquered Unattainable to Attainable Lipton R-III Right Coronary Artery Chronic Total Occlusion to Reprieve My Patient
Ankit Gupta1, Bhushan Shah2, Sreenivas Reddy S.3
All India Institute of Medical Sciences, India1, All India Institute Of Medical Sciences Bhopal, India2, Post Graduate Institute of Medical Education and Research, India3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 64-year-old hypertensive and chronic smoker male was presented at our tertiary care center with chief complains of Canadian Cardiovascular Society (CCS) II angina. He was haemodynamically stable during the admission
Relevant Test Results Prior to Catheterization
Patient was investigated thoroughly his blood counts and renal function tests were normal , his echocardiography showed Mild Inferior wall hypokinesia , LVDD -I , LVEF 55%
Relevant Catheterization Findings
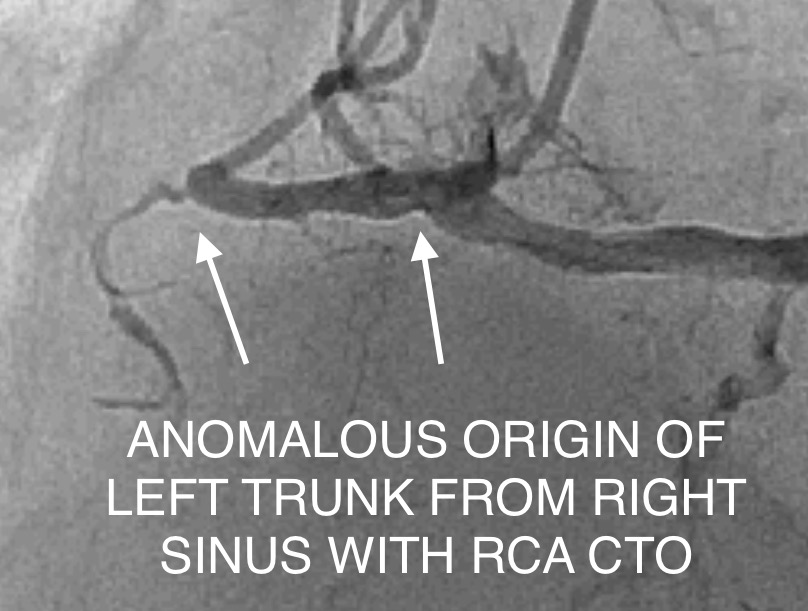
Patient coronary angiogram revealed anomalous left and right coronary arising from single sinus, normal long left main running straight in right anterior oblique view suggesting running between pulmonary artery and aorta with diffuse plaque in left anterior descending artery (LAD), plaque in left circumflex artery (LCX), and ostial plaque in major OM1 branch. The right coronary artery (RCA) was dominant representing CTO of proximal segment was retrogradely filling from left system
Interventional Management
Procedural Step
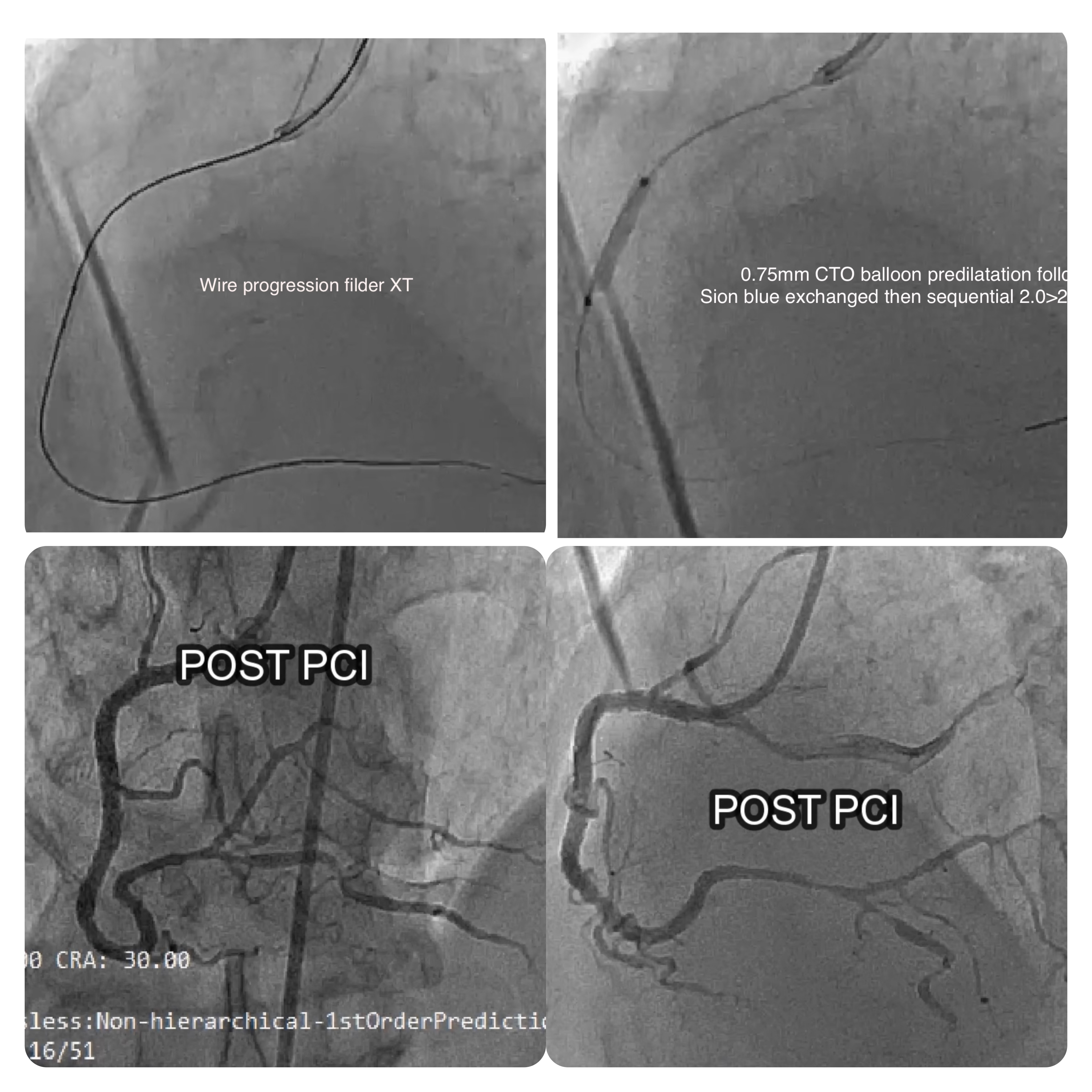
Procedure: PCI TO RCA CTO (VIVO ISAR 3.00 x 48 mm)RCA hooked with JR 3.5/6F Guiding Catheter With Support Of Micro-Catheter Sion Blue wire was used to cross the lesion but attempt failed later Fielder XT wire crossed the lesion and kept in PDA, another wire placed in aorta, Pre dilated with ALVEO HP 0.75x08 mm at 10-12 atm pressure F/B Pre dilated with MINI TREK 1.2× 12 mm at 8-10 atm pressure Later Fielder XT exchanged with Sion Blue wire. Pre dilated with MINI TREK 1.50 × 15 mm at 6-8 atm pressure F/B Pre dilated with TREK 2.50×15mm at 6-8 atm pressure. Stent VIVO ISAR 3.00 x 48 mm deployed in Prox-Mid RCA at 12 atm pressure. Stent post dilated with PIPIT NC balloon 3.25 x 12 mm balloon at 14-18atm distally and at 18-20 atm pressure proximally.
Case Summary
- Coronary angiography remains the gold standard for diagnosis and classification of single coronary artery
- Treatment options include conservative medical management, percutaneous coronary intervention (PCI) with stent placement, and surgical correction. Treatment options include conservative medical management, percutaneous coronary intervention (PCI) with stent placement, and surgical correction.