
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-072
A Challenging Chronic Total Occlusion Case: When the Microcatheter Tip Was Detached at a Tight Lesion
By David TE-WEI Kuan
Presenter
David Kuan
Authors
David TE-WEI Kuan1
Affiliation
National Taiwan University Hospital, Taiwan1,
View Study Report
TCTAP C-072
Coronary - Complex PCI - CTO
A Challenging Chronic Total Occlusion Case: When the Microcatheter Tip Was Detached at a Tight Lesion
David TE-WEI Kuan1
National Taiwan University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 61-year-old man cameto the cardiology outpatient clinic complaining of worseningexertional chest tightness for few months. He underwentpercutaneous coronary intervention two years ago , and had onedrug eluting stent inserted into the left anterior descending arteryand three in the right coronary artery. Chronic totalocclusion of the proximal circumflex artery was also noted during theprocedure but it was not treated. Other past medical history included diabetes mellitus and hypertension.
Relevant Test Results Prior to Catheterization
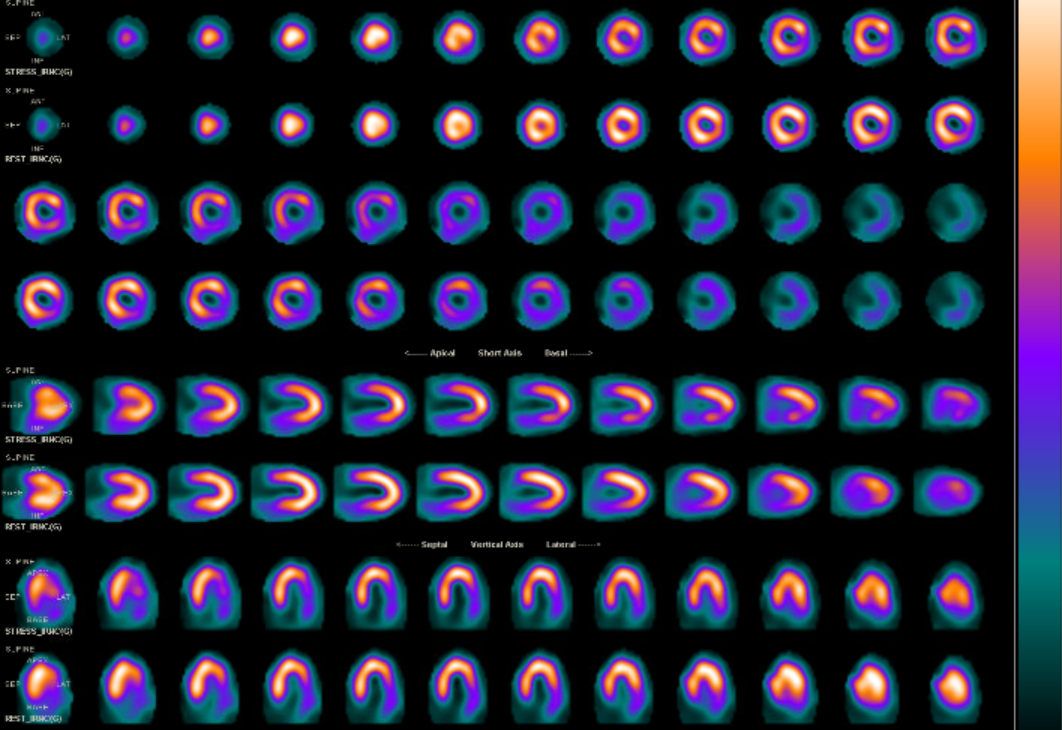
Heart sound wasregular and without any murmur. Breathing sound was clear onauscultation, and there was no peripheral edema. Electrocardiogramrevealed regular sinus rhythm without ischemic changes. Laboratorytest showed hemoglobin of 14.9g/dL, platelet count of 167k/μL andcreatinine of 1.4mg/dL. Myocardial perfusionimaging demonstrated stress induced ischemia at basal anterior,anteroseptal and inferolateral wall which were mixed withsubendocardial scar.
Relevant Catheterization Findings
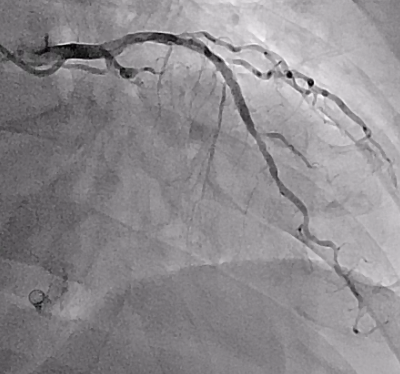
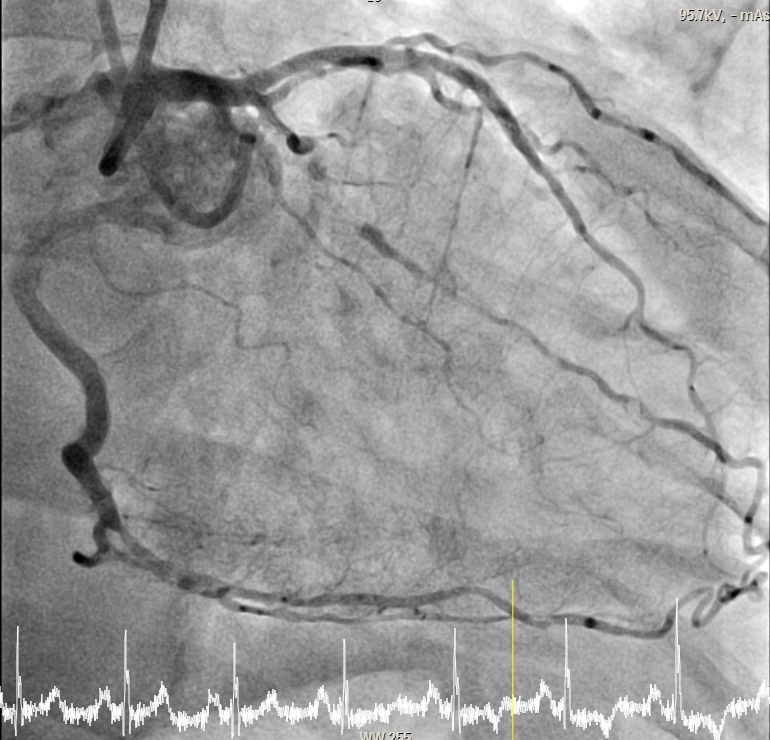
Right coronary artery, left main and left anterior descending artery were all patent. Chronic totalocclusion of the proximal circumflex coronary artery with collateralcirculation from the right coronary artery via the posteriordescending artery was confirmed. . Dual injection angiography using biradial access was performed. A blunt stump could be identified.
Interventional Management
Procedural Step
Wedecided to tackle the chronic total occlusion lesion using antegradeapproach. A Gaia third wire was used to penetrate the proximal cap ofthe chronic total occlusion with the support from Guidezilla.However, the lesion was uncrossable by 1.0mm coronary balloon.Several methods including using FineCross and Corsair microcatheter,using Guidezilla, performing grenadoplasty were attempted withoutsuccess. Thus we had to use subintimal technique with support fromCaravel microcatheter to pass the lesion. Balloon dilatation wasperformed using 1.0mm compliant coronary balloon. Angiogram showedthe wire was likely not in the true lumen. Parallel wiring techniquewas used to reach the distal Circumflex artery with Conquest Pro.Left obtuse marginal artery was protected. We switched Conquest Prowire to Sioh blue and confirmed it was within the true lumenangiographically. Balloon dilatation was performed using 1.0mm and1.5mm compliant coronary balloon from distal to proximal segment.Following the retrieval of the Caravelmicrocatheter, a radiopaque spot was noted at the vessel wall on theangiogram which was suspected to be the detached tip of the Caravelmicrocatheter. The flow of the Circumflex artery didn’t seem to beimpaired and the patient remained hemodynamic stable. Therefore, wedecided to continue the procedure without retrieving the detachedCaravel tip. Intravascular ultrasound reassured the wire was in the intraplaque location. Durg eluting stents were placed.



Case Summary
There are several methods for balloon uncrossable lesion including using small balloons and other techniques that increase support including using microcatheter, guide extension and extra supportive wire. We used subintimal technique as other methods were unsuccessful. Caravel microcatheter is good for crossing long narrow channels.and tortuous vessels. There are case reports on Caravel microcatheter tip detachment when attempting to cross severely calcified lesion. The mechanism is probably due to its lower profile tip and hydrophilic-coated thin wall structure. Based on the case reports, the detached tip is retrievable. However, we decided not to retrieve it as it didn't compromise the flow.