
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-089
OCT Guided Provisional Stenting Distal Left Main -LAD
By Fani Suslina Hasibuan
Presenter
Fani Suslina Hasibuan
Authors
Fani Suslina Hasibuan1
Affiliation
RSUD Dr R Koesma, Indonesia1,
View Study Report
TCTAP C-089
Coronary - Complex PCI - Left main
OCT Guided Provisional Stenting Distal Left Main -LAD
Fani Suslina Hasibuan1
RSUD Dr R Koesma, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 62-year-old man presented with NSTEMI came to our hospital. His ECG showed slight ST depression on the anterolateral lead. His coronary risk factor was hypertension. His physical examination was unremarkable.

Relevant Test Results Prior to Catheterization
Troponin level was elevated. Echocardiography showed Normal LVEF with a hypokinetic anterior wall. Grace's Score was 111 and his TIMI Risk Score was III.
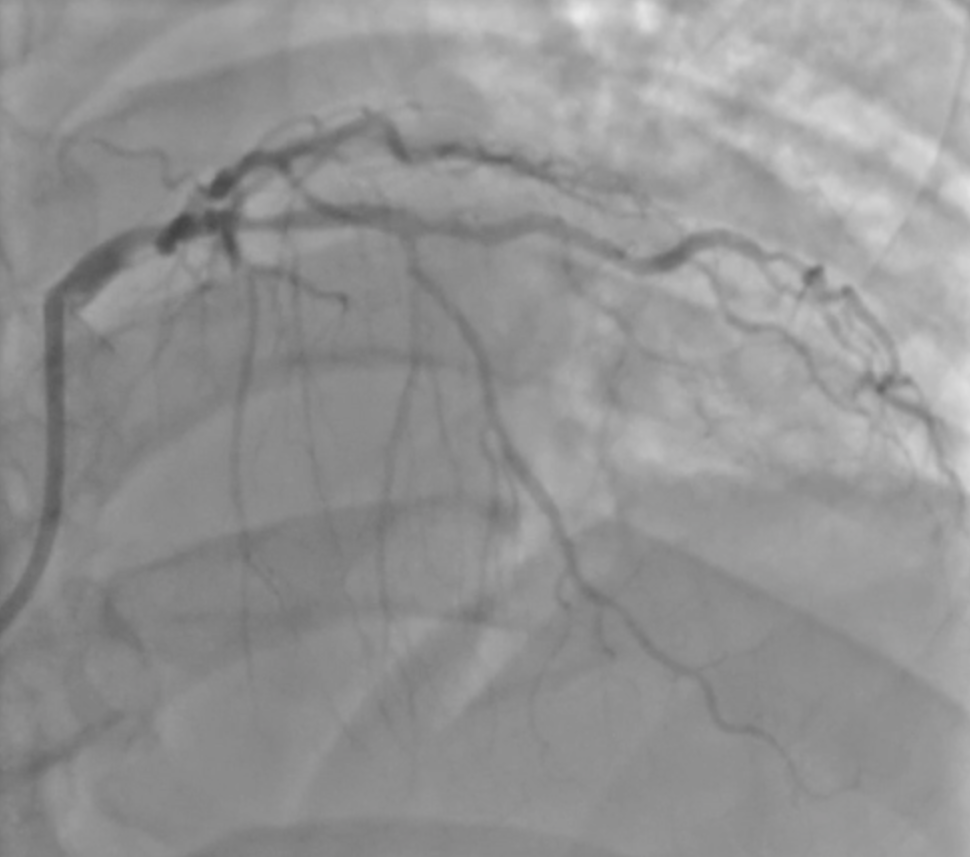
Relevant Catheterization Findings
There was severe stenosis at distal LM, severe stenosis at osteal to proximal LAD, and mild stenosis at mid-LCX. RCA was normal. The syntax score was 18, but the patient refused to do CABG, so we proceeded to PCI.


Interventional Management
Procedural Step
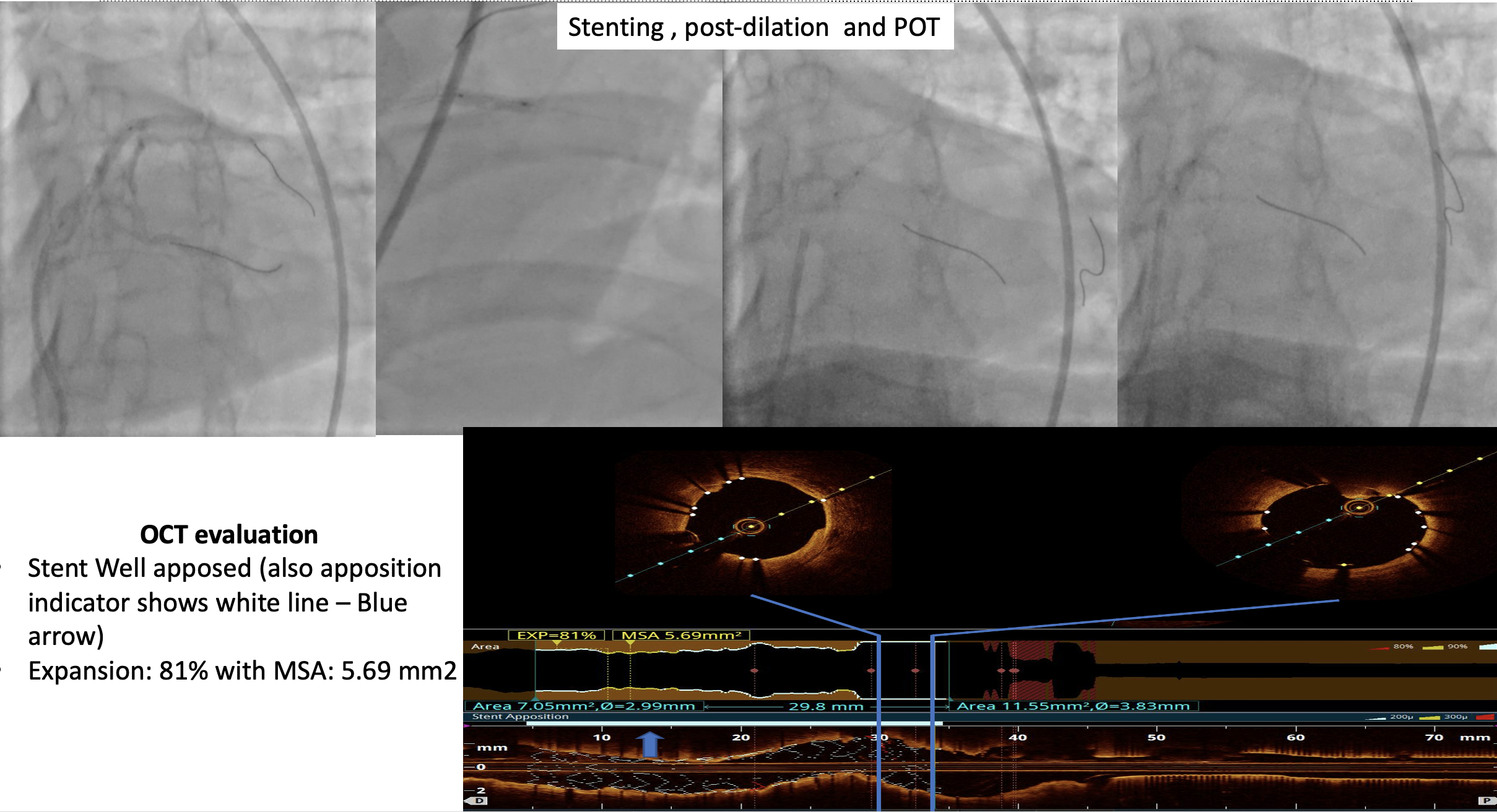
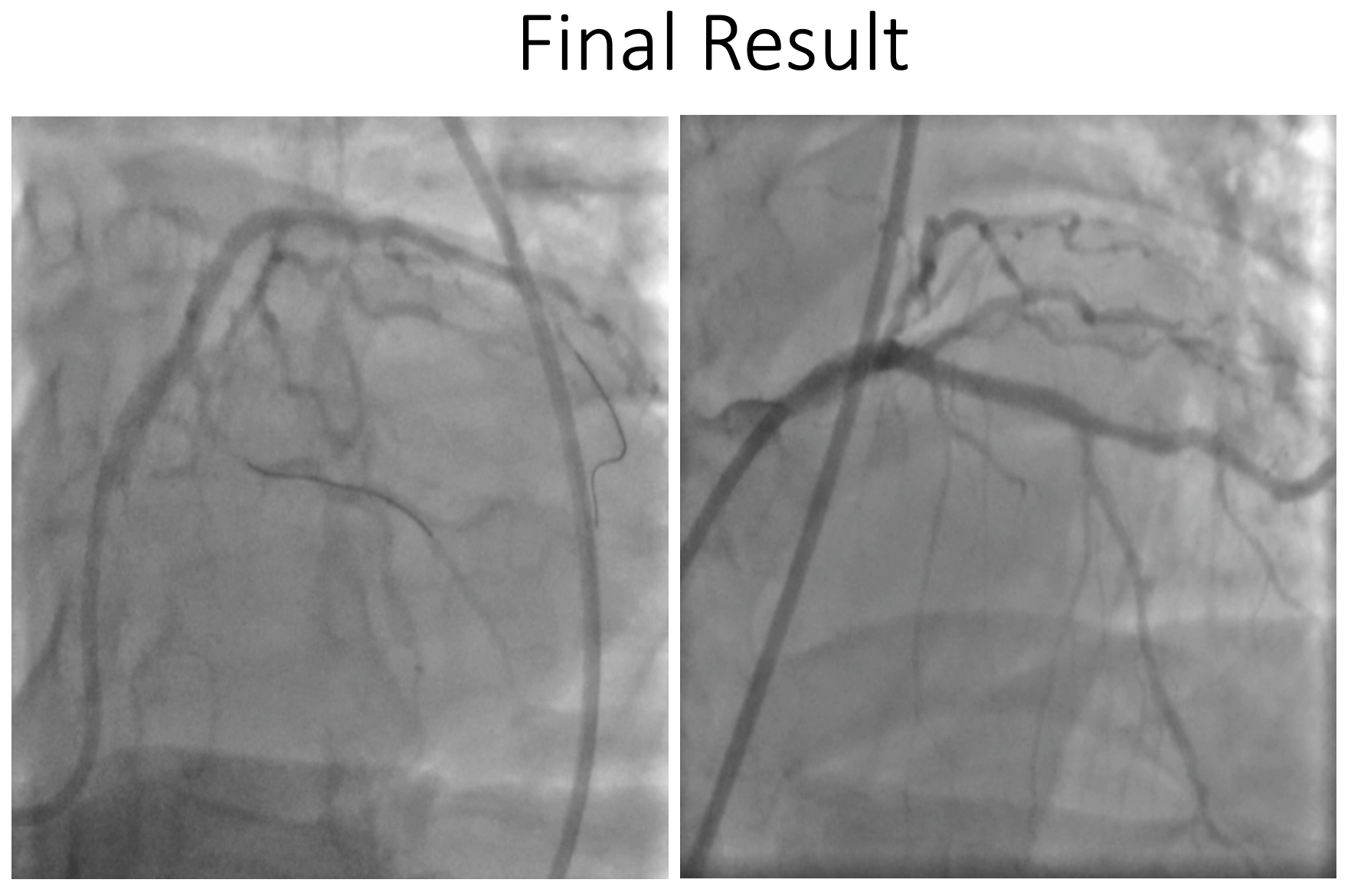
A 7 Fr CLS 3.5 guiding catheter was engaged into LCA ostium through the right femoral artery, after successfully inserting floppy wire to distal LAD. OCT evaluation showed fibro lipidic plaque, MLA 2.3 mm at LAD lesion and 4.0 mm at distal LM, distal reference 3.08 mm. Predilation was done using a 2.5 x 15 mm semi-compliance balloon (SCB) in LAD. We performed professional stenting LM-LAD to settle the bifurcation lesion. A 3.0 x 33 mm EES was placed at distal LM to proximal LAD and deployed 18 atm. After that post-dilation and POT was done using NC Balloon 3.5/15mm and NC Balloon 4.0/8 mm. Final OCT evaluation showed well-apposed and expanded stents without stent edge dissections. The Final angiogram showed TIMI 3 flow, and, the flow in LCx was also good.

Case Summary
Intracoronary imaging facilitates angiographic interpretation and may guide treatment in acute coronary syndrome, guidance of stent selection, and optimization of deployment. OCT-guided PCI in non-ostial LM coronary artery is feasible.