
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-062
Tango Dance of the Retrograde Microcatheter During CTO PCI
By Yu-Ching Chang, Ying-Hsien Chen
Presenter
Yu-Ching Chang
Authors
Yu-Ching Chang1, Ying-Hsien Chen2
Affiliation
National Taiwan University Hospital Hsin-Chu Branch, Taiwan1, National Taiwan University Hospital, Taiwan2,
View Study Report
TCTAP C-062
Coronary - Complex PCI - CTO
Tango Dance of the Retrograde Microcatheter During CTO PCI
Yu-Ching Chang1, Ying-Hsien Chen2
National Taiwan University Hospital Hsin-Chu Branch, Taiwan1, National Taiwan University Hospital, Taiwan2,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
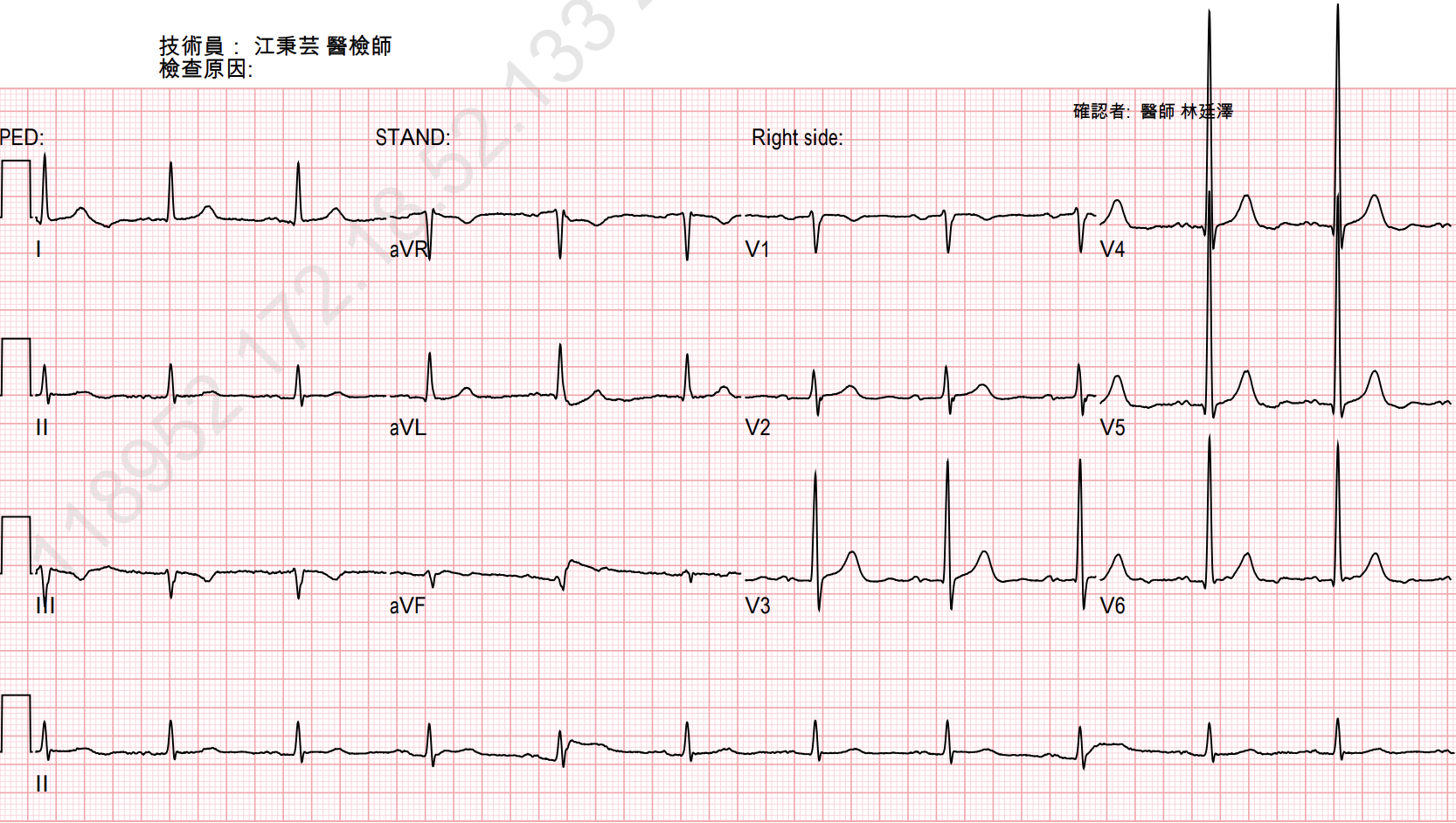
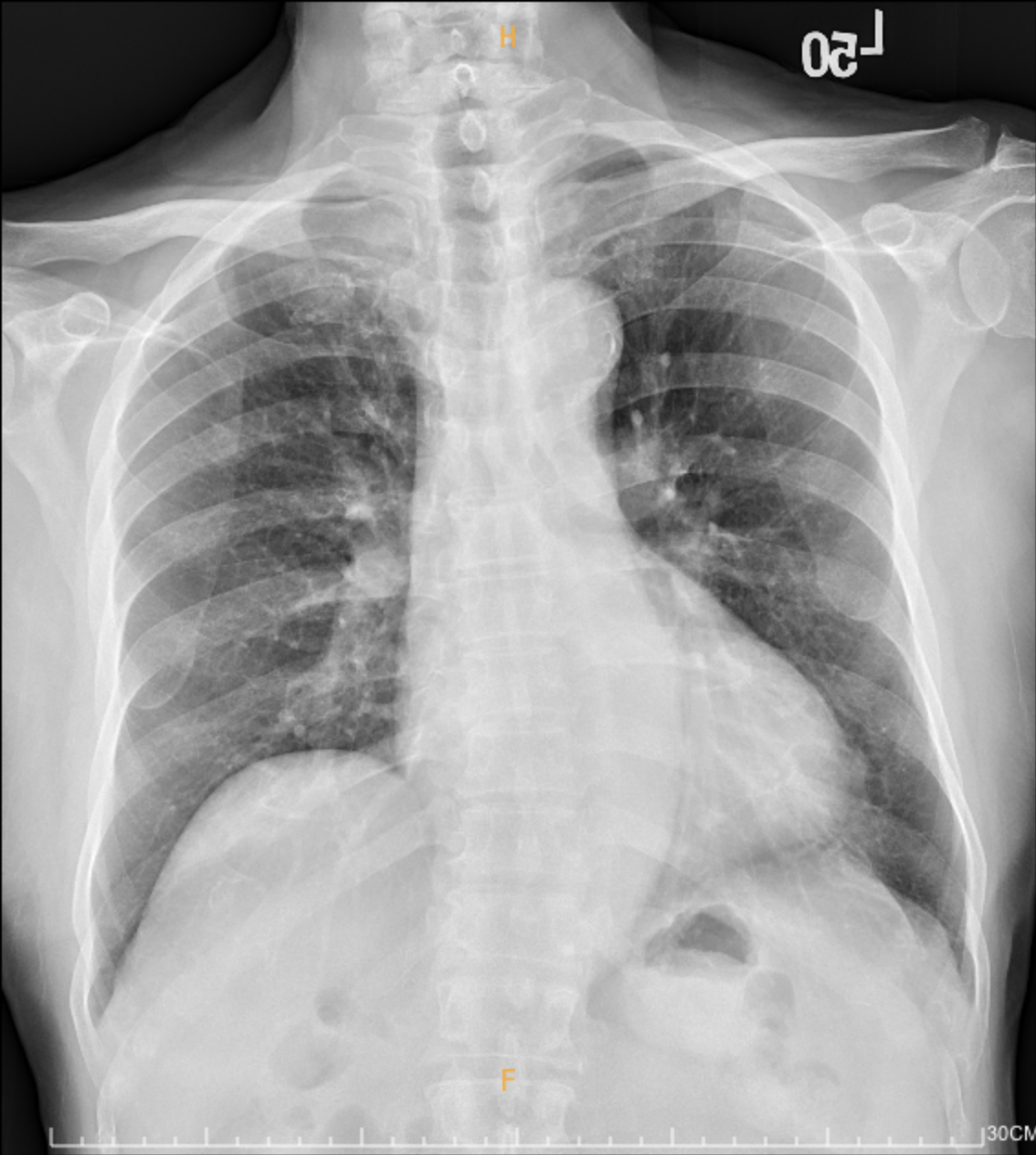
A 71-year-old man has a history of hypertension, dyslipidemia and type 2 diabetes mellitus. Also, he is an ex-smoker. He presented to our outpatient (OPD) clinic owing to intermittent chest tightness for 2 months. 2 years before index admission, the chest radiograph arranged at our OPD clinic revealed progressive cardiomegaly, and the subsequent echocardiogram showed regional wall motion abnormality. Besides, the myocardial perfusion imaging showed relative perfusion defects at the inferior wall.

Relevant Test Results Prior to Catheterization
Echocardiography: - Left atrial dilation- Left ventricular ejection fraction: 58.1%- Apical hypokinesia- Mild mitral regurgitation- Mild tricuspid regurgitation
Myocardial perfusion imaging: - Stress-induced ischemia at mid to basal inferoseptal and inferior wall- Post-stress LV dysfunction and transient dilatation
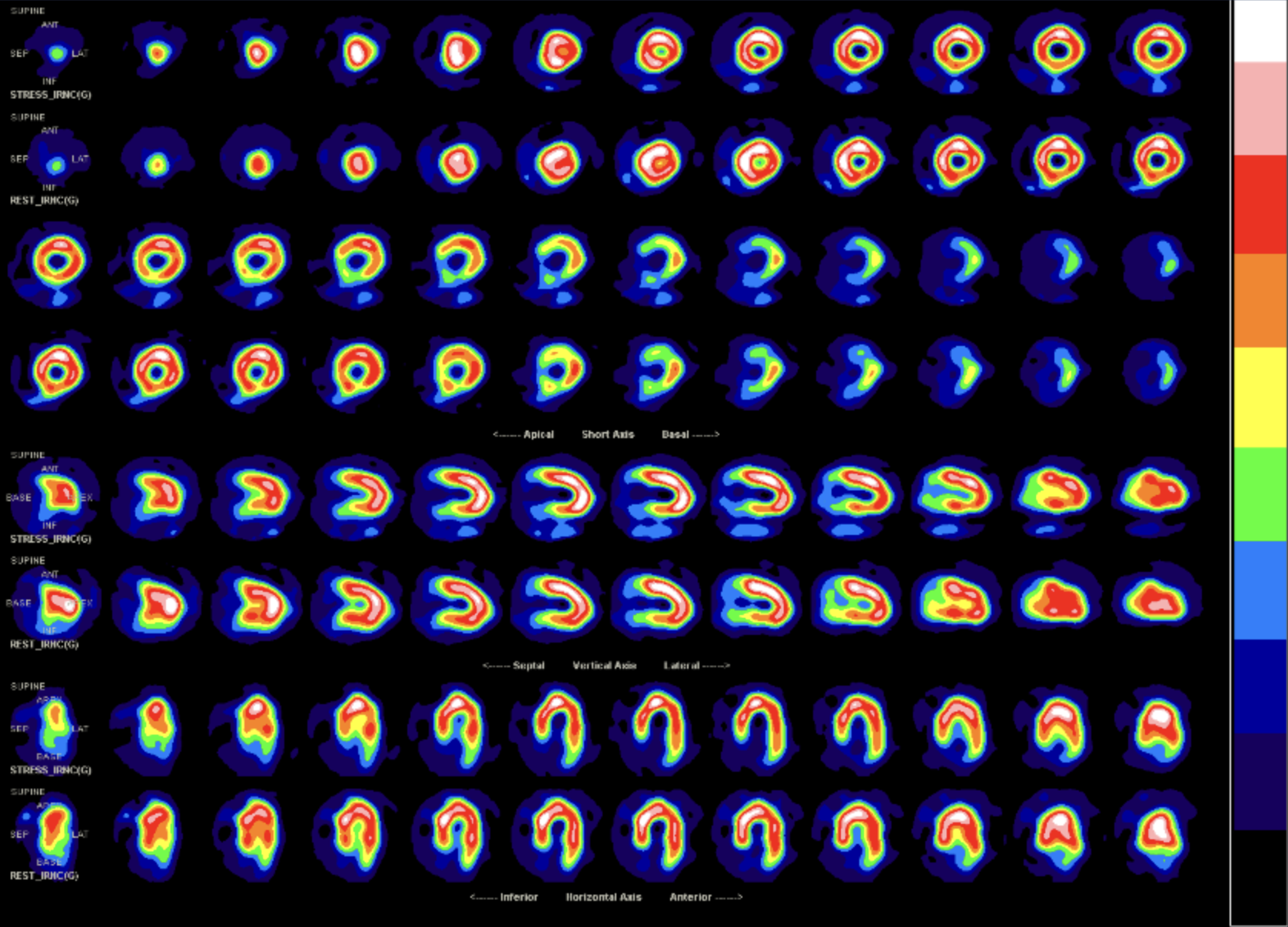
Myocardial perfusion imaging: - Stress-induced ischemia at mid to basal inferoseptal and inferior wall- Post-stress LV dysfunction and transient dilatation
Relevant Catheterization Findings
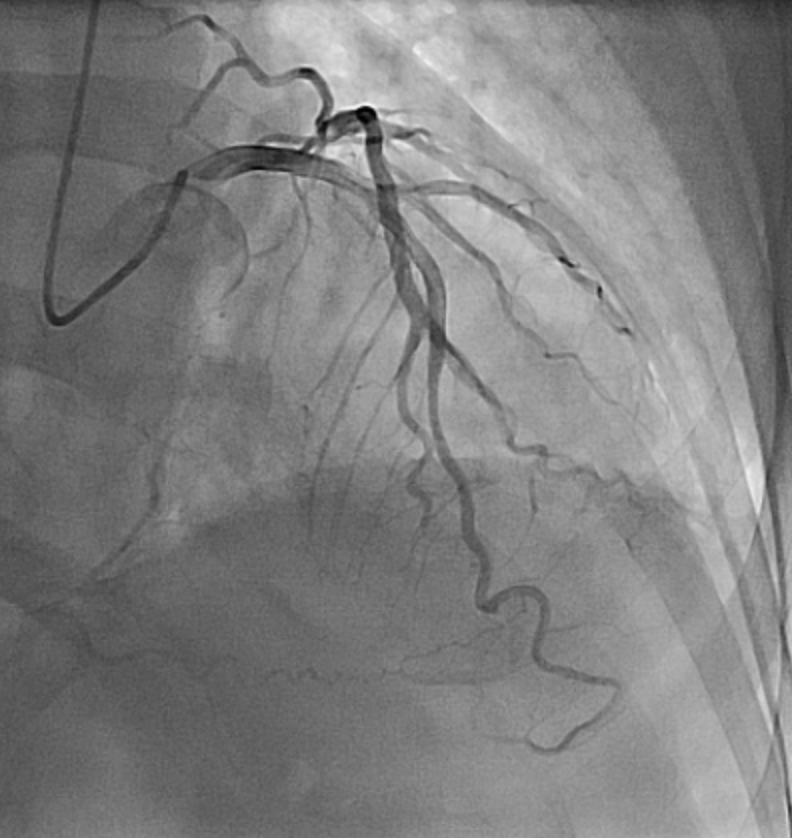
Left main artery: patent Left anterior descending artery: distal stenosis 40%, distal collateral to posterior descending artery (PDA), diagonal branch collateral to right ventricular branchLeft circumflex artery: distal luminal irregularities, collateral to posterolateral artery Right coronary artery (RCA): proximal diffuse stenosis 70%, middle chronic total occlusion, distal diffuse stenosis 60%, PDA diffuse stenosis 30%, ipsilateral bridging collateral to distal RCA


Interventional Management
Procedural Step
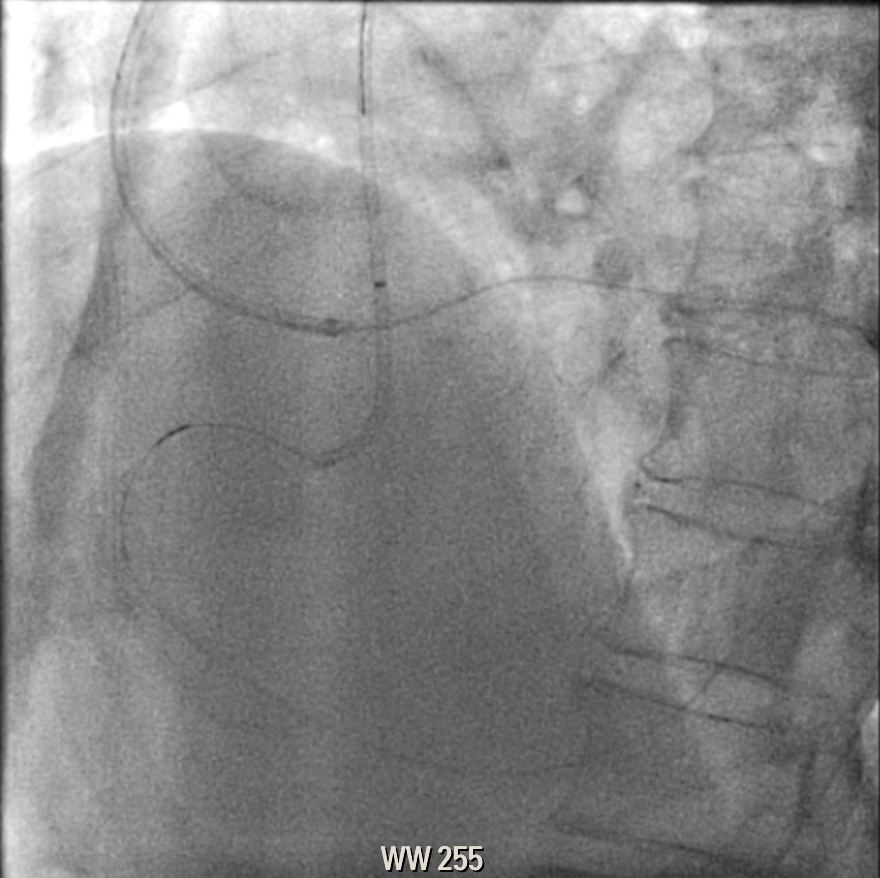
The coronary angiography showed chronic total occlusion at the mid-right coronary artery (RCA). Collateral vessels to posterolateral artery were from the branch of left circumflex artery. Our team tried antegrade approach first, but failed. We then performed retrograde wiring, with success. However, we hardly advanced the retrograde microcatheter into the antegrade guiding catheter, which the retrograde microcatheter retracted back to the lesion site during manipulation. Externalization was finally established by advancing the RG3 wire into the antegrade guiding catheter alone without microcatheter. We pre-dilated from proximal to distal RCA, and deployed 2 drug-eluting stents from proximal to distal RCA. The final flow of RCA reached TIMI 3 flow.


Case Summary
Performing percutaneous coronary intervention for chronic total occlusion (CTO) needs accurate strategy planning and skillful techniques. Troubleshooting for crossing the CTO lesion always plays a pivotal role. In addition, the interventional cardiologists should realize how to solve the obstacle problems during externalization. In summary, with these well-planned strategies and skillful techniques, crossing CTO lesions is no longer a dream but a routine practice.