TCTAP C-205
Endovascular - Thrombus Removal Devices and Techniques
A Challenging Case of Massive Acute on Chronic Bilateral Main Pulmonary Artery Embolism Requiring Mechanical Thrombectomy, Catheter Directed Thrombolysis and ECMO
Ahmad Bakhtiar Md Radzi1, Muhammad Hanis Muhmad Hamidi1, Huzairi Sani2, Raja Ezman Raja Shariff3, Khairul Shafiq Ibrahim1, Rizmy Najme Khir4, Johan Rizwal Ismail5, Abdul Wahab Undok6, Sazzli Kasim1
Universiti Teknologi MARA (UiTM), Malaysia1, Hospital Pantai Klang, Malaysia2, Hospital Universiti Teknologi MARA (UiTM), Malaysia3, Ara Damansara Medical Centre, Malaysia4, Prince Court Medical Centre, Malaysia5, Kpj Rawang Specialist Hospital, Malaysia6,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 35-year-old man presented with worsening breathlessness for 3 days. It was associated with intermittent central chest heaviness with no radiation which occurs at rest with no precipitating factor such as breathing, movement and exertion. He had reduced effort tolerance for the past 1 month with New York Heart Association (NYHA) class 2. He smokes 1 pack years. There was no significant family history of blood disorders. Physical examinations were unremarkable apart of tachycardia of 110/minute.

Relevant Test Results Prior to Catheterization
The HS Troponin I was 62.3 ng/L. Echocardiogram showed left ventricular ejection fraction of 45% with the right ventricle and right atrial were dilated with estimated pulmonary artery systolic pressure (PASP) was least 54mmHg. Coronary angiogram showed normal findings. CT angiography of pulmonary artery revealed large filling defects in the right and left pulmonary arteries extending into segmental and sub-segmental branches.


Relevant Catheterization Findings
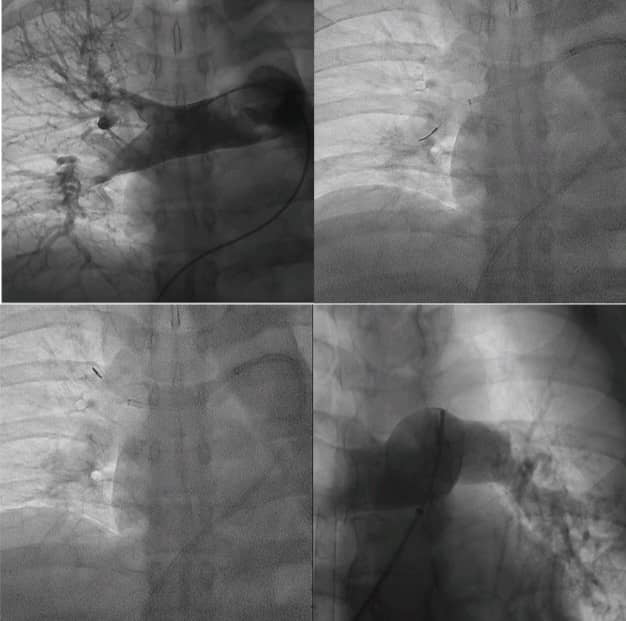
Percutaneous mechanical thrombectomy was performed via right femoral vein approach. Pulmonary angiogram revealed large filling defects in the right and left pulmonary arteries. Multiple attempts to engage and open-up the left upper and middle lobe branches, however were unsuccessful. Subsequently, we proceeded to aspirate the right main pulmonary artery. Patient deteriorate during the procedure needing CPR and maximum inotropic support. Extracorporeal membrane oxygenation was initiated then.
Interventional Management
Procedural Step
Once the hemodynamics and blood pressure of the patient was stabilized, catheter directed thrombolysis using Alteplase to the left main pulmonary was initiated with a bolus dose and subsequently maintenance for 6 hours. After 24-hours post mechanical thrombectomy, we proceeded again with a repeat procedure after clinically stable using Penumbra system to revascularized the occluded pulmonary arteries. We also need to use modified technique using the coronary wires (0.014) with balloon inflation technique to open-up the occluded and calcified pulmonary arteries. The left lower branches were dilated indicating an acute on chronic pulmonary embolism in this case. Unfortunate, the left upper branch was unable to be recanalized. The patient was subsequently managed to be extubated after 7 days on ECMO and medication support. He was discharge well with a high dose of warfarin 7.0 mg daily based on the targeted INR value. Antiphospholipid markers were negative and the hemophilia screening was planned to be taken later.

Case Summary
We encounter a challenging case of massive acute on chronic bilateral pulmonary artery embolism requiring repeated mechanical thrombectomy, catheter directed thrombolysis and ECMO in this case. Adequate knowledge and strategies in the management of acute pulmonary embolism is vital to revascularized the occluded main pulmonary arteries. Option of mechanical thrombectomy, catheter directed thrombolysis or both strategies may be warranted in certain cases as illustrated here. Mechanical support using ECMO is essential in unstable massive pulmonary embolism.
