
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-041
"Cracking the Calcium Code": Strategies and Outcomes in Angioplasty for Coronary Lesions With High Calcium Burden
By Sharimila Shanmugam, David Yong, Amin Ariff Nuruddin
Presenter
Sharimila Shanmugam
Authors
Sharimila Shanmugam1, David Yong1, Amin Ariff Nuruddin1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-041
Coronary - Complex PCI - Calcified Lesion
"Cracking the Calcium Code": Strategies and Outcomes in Angioplasty for Coronary Lesions With High Calcium Burden
Sharimila Shanmugam1, David Yong1, Amin Ariff Nuruddin1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
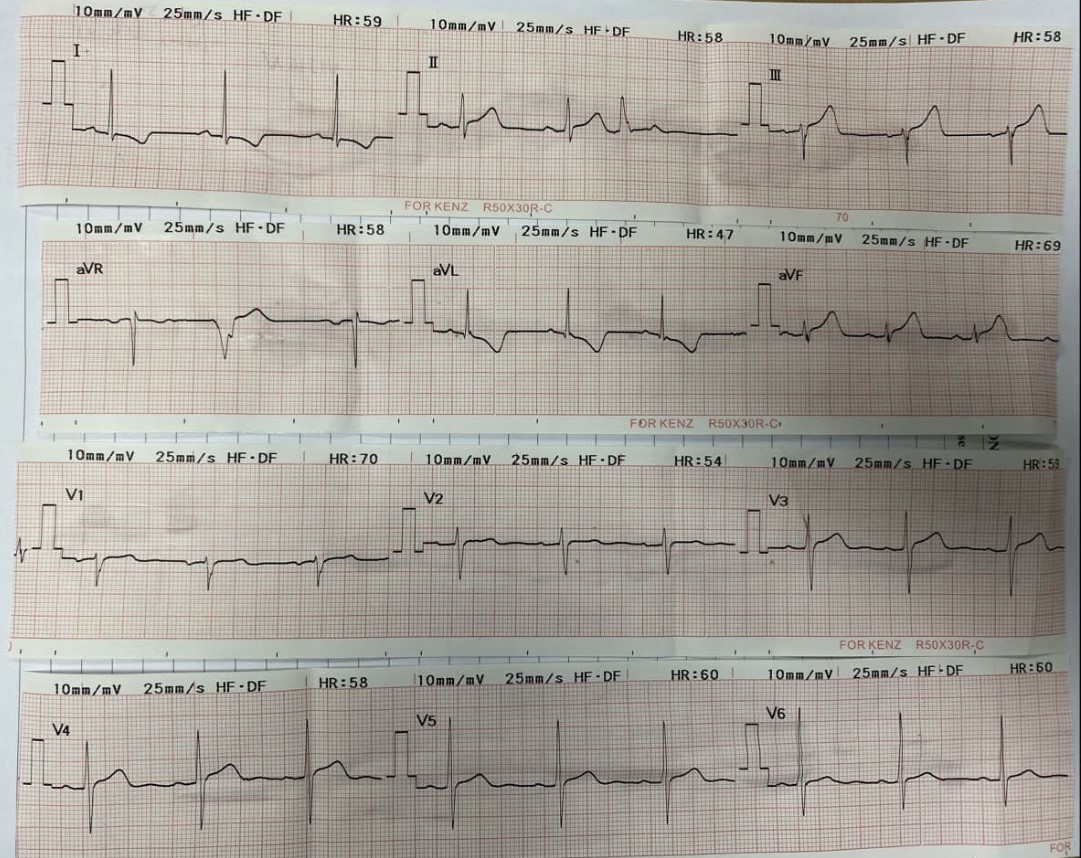
A 67-year-old retired fireman, a smoker with chronic kidney disease, hypertension, and hyperlipidemia, presented to a district hospital with chest pain and diaphoresis. ECG ST elevation in II, III, AvF. Blood pressure measured at 165/96mmHg, Pulse rate 68. Cardiovascular examination revealed no murmurs. He was diagnosed with acute inferior myocardial infarction (Killip I) and was thrombolysed with Intravenous Streptokinase. Subsequently he was transferred to our center for further management.

Relevant Test Results Prior to Catheterization
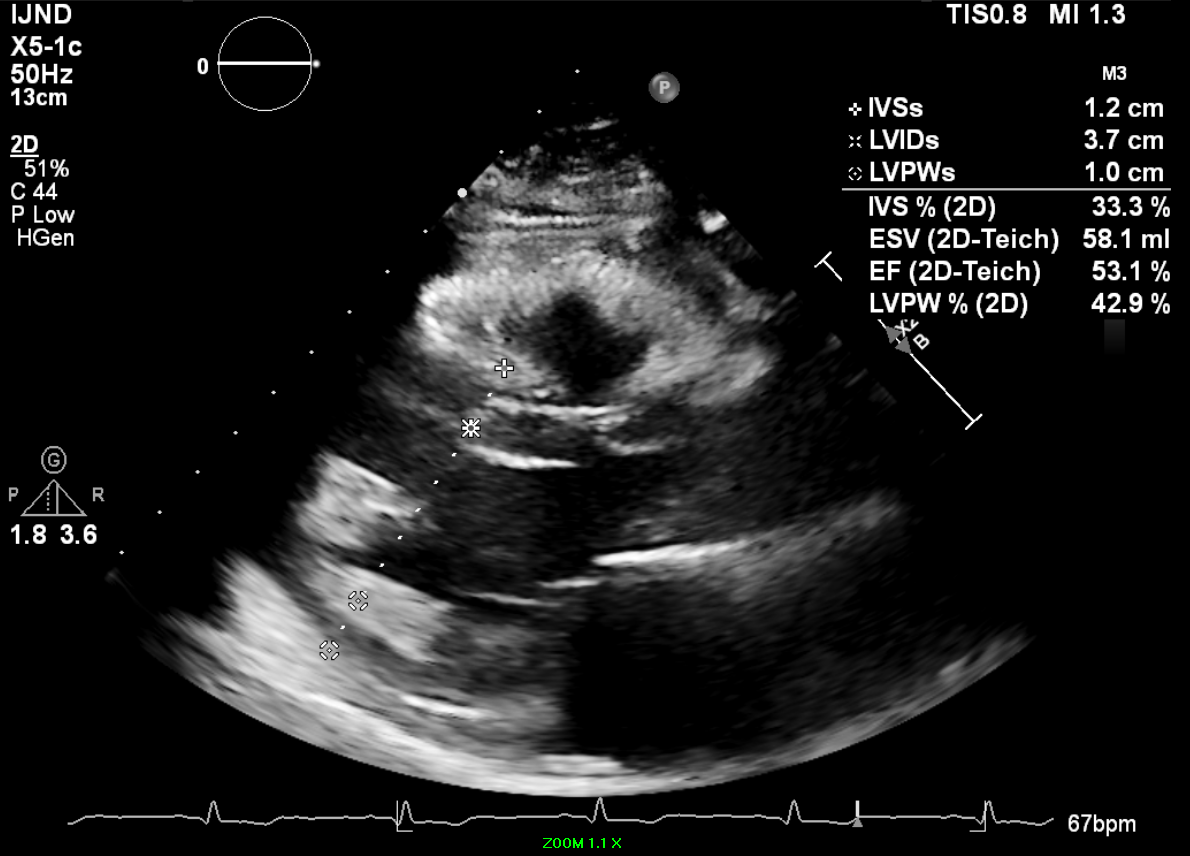
Troponin I elevated at 890 Total cholesterol 3.9 LDL 2.3 HDL 0.96 Triglycerides 1.42 Hbaic 5.9%Creatinine 118 eGFR 55ml/min/1.73m2Echocardiogram shows Ejection fraction 40-45% with regional wall motion abnormalities at basal and mid inferior lateral wall, basal septal, mid anterior and basal anterior wall. TAPSE 2.1cm Normal Left and right atrium.
Relevant Catheterization Findings
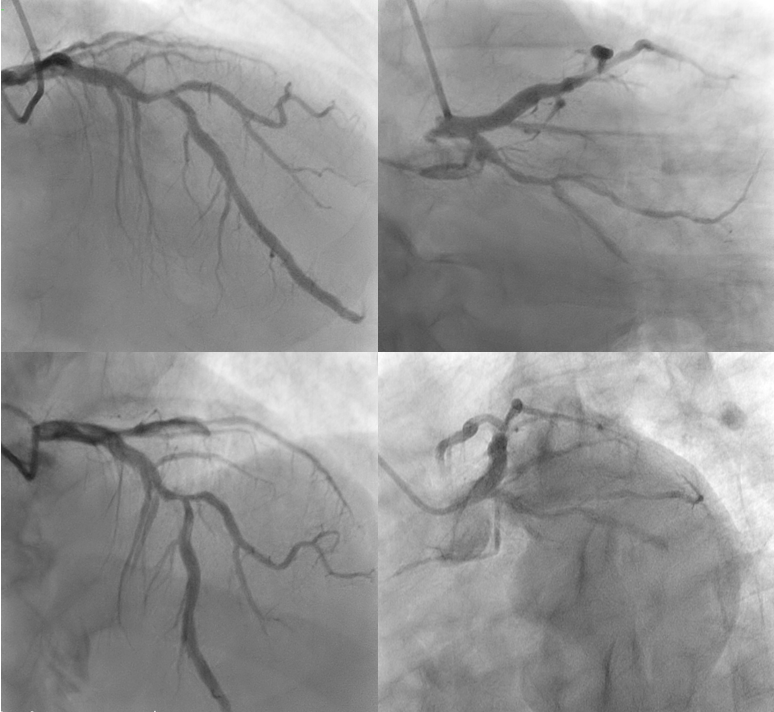
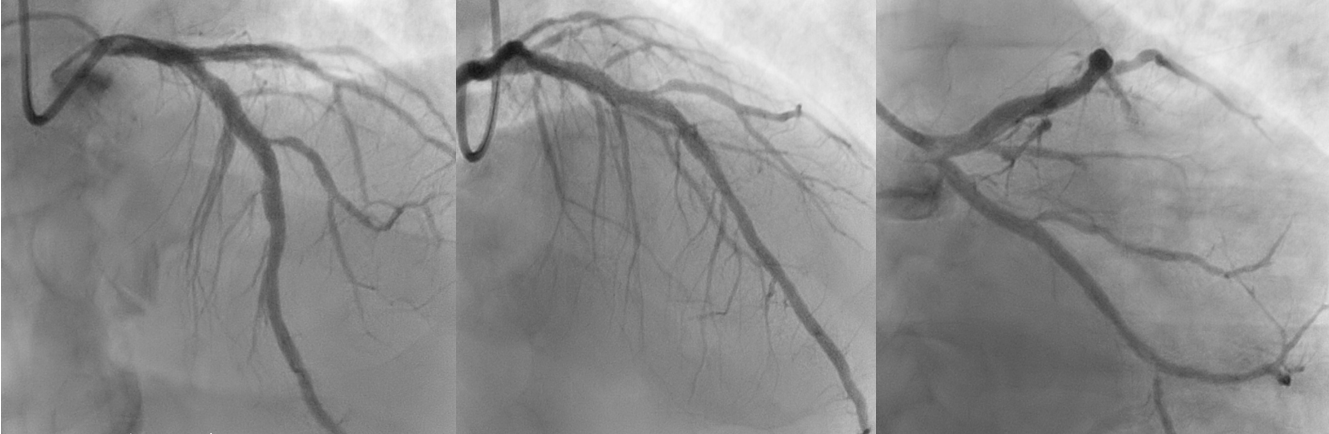
Diagnostic coronary angiogram via right radial artery was performed with Terumo 6 Fr sheath and Opti-torque 5fr catheter. The findings revealed a normal Left Main Stem, severe proximal to mid calcified disease in the Left Anterior Descending artery, subtotal occlusion in the mid Left Circumflex Artery, and mild to moderate stenosis in the mid Right Coronary Artery, with moderate to severe disease in the Right Posterior Descending Artery.

Interventional Management
Procedural Step
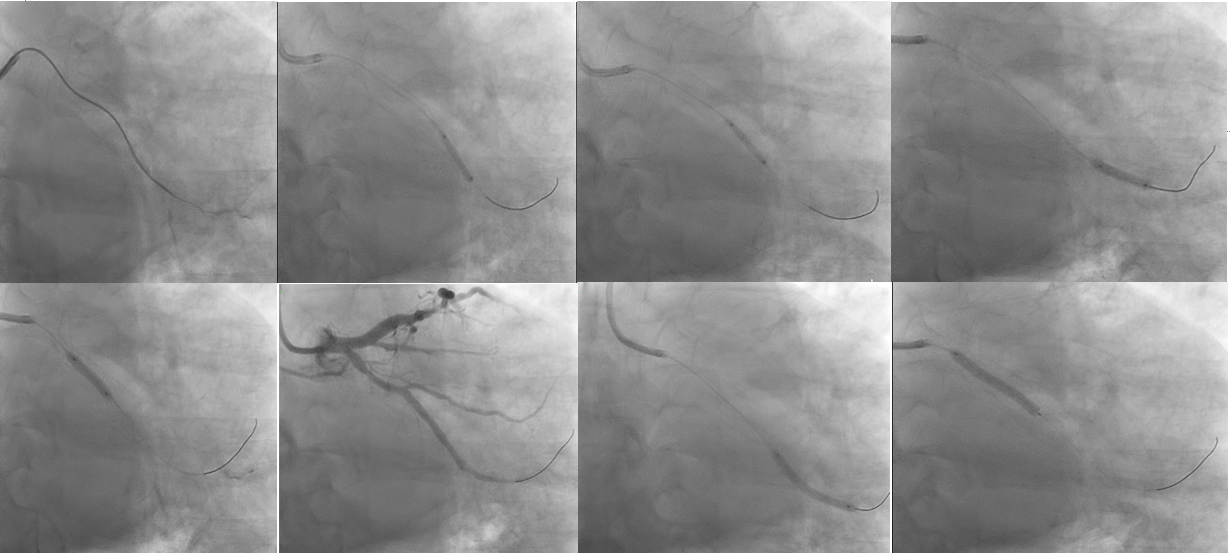
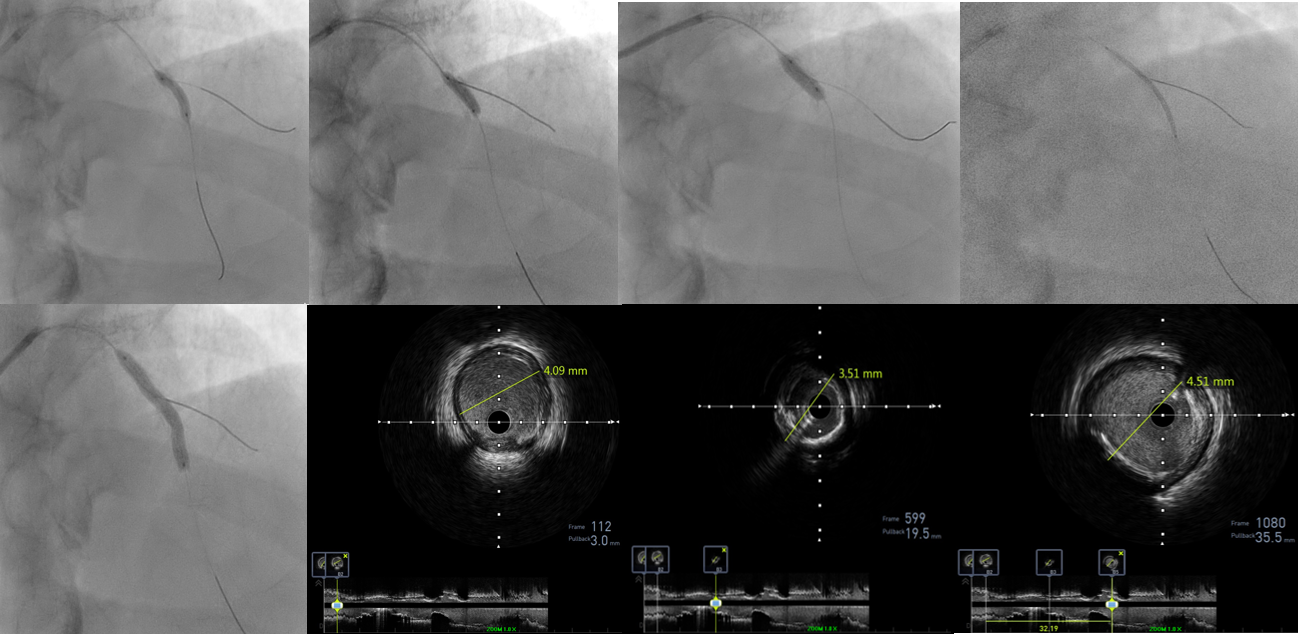
Coronary angioplasty to the left system using an EBU 3.5/6Fr guiding catheter. Left circumflex artery stenosis was addressed using microcatheter Asahi Corsair135cm and Fielder XT wire then after exchanged to Run-through floppy. Intravascular Ultrasound (IVUS) was done.
Case Summary
The case involved the successful application of Intravascular Lithotripsy (IVL) in treating calcified lesions during coronary angioplasty. Intravascular Lithotripsy (IVL) is crucial for treating calcified lesions in coronary angioplasty, where calcium deposits in the arteries pose challenges to effective intervention. Calcium in the arteries can lead to vessel narrowing, reducing compliance and complicating stent deployment. IVL is important in such cases as it utilizes sonic pressure waves to fracture and modify calcified plaques, allowing for improved vessel compliance and enhancing the success of angioplasty procedures.