
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-033
Dousing the Fire Dragon
By Afrah Yousif Haroon, Shaiful Azmi Yahaya
Presenter
Afrah Yousif Haroon
Authors
Afrah Yousif Haroon1, Shaiful Azmi Yahaya1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-033
Coronary - Complex PCI - Calcified Lesion
Dousing the Fire Dragon
Afrah Yousif Haroon1, Shaiful Azmi Yahaya1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
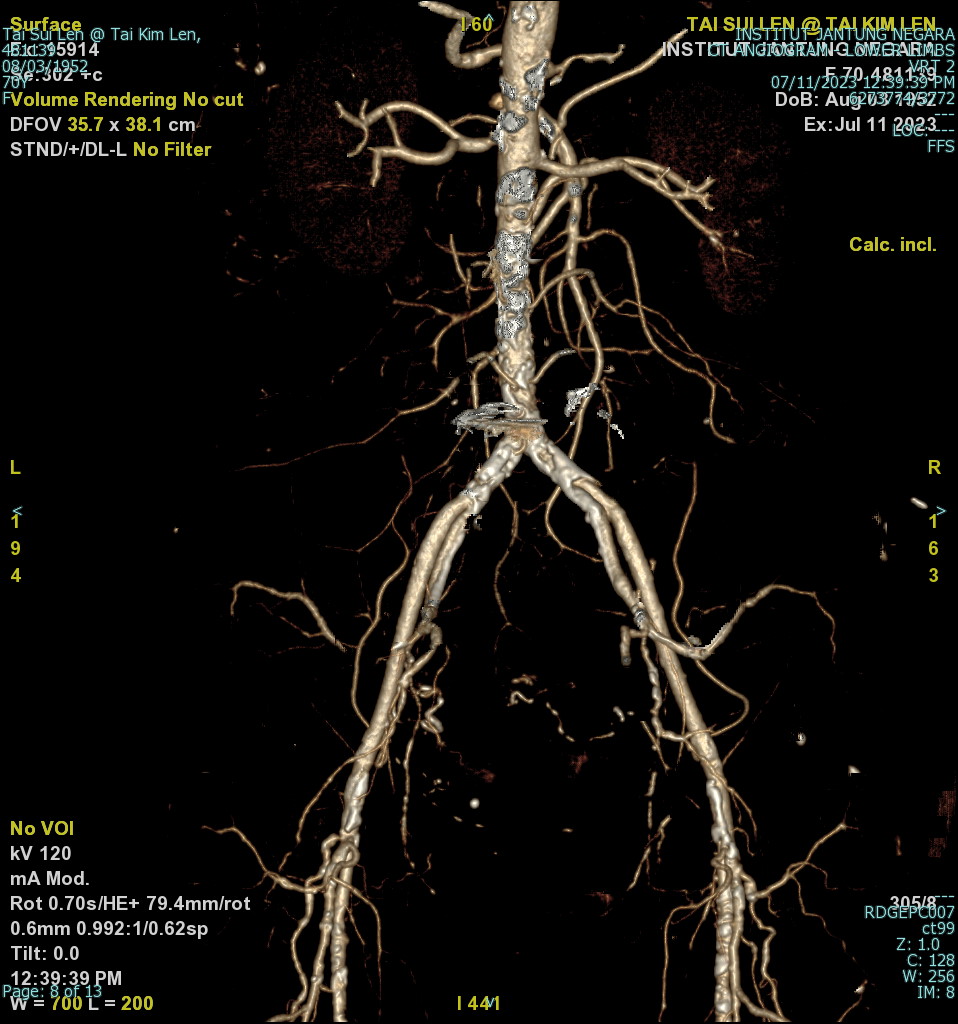
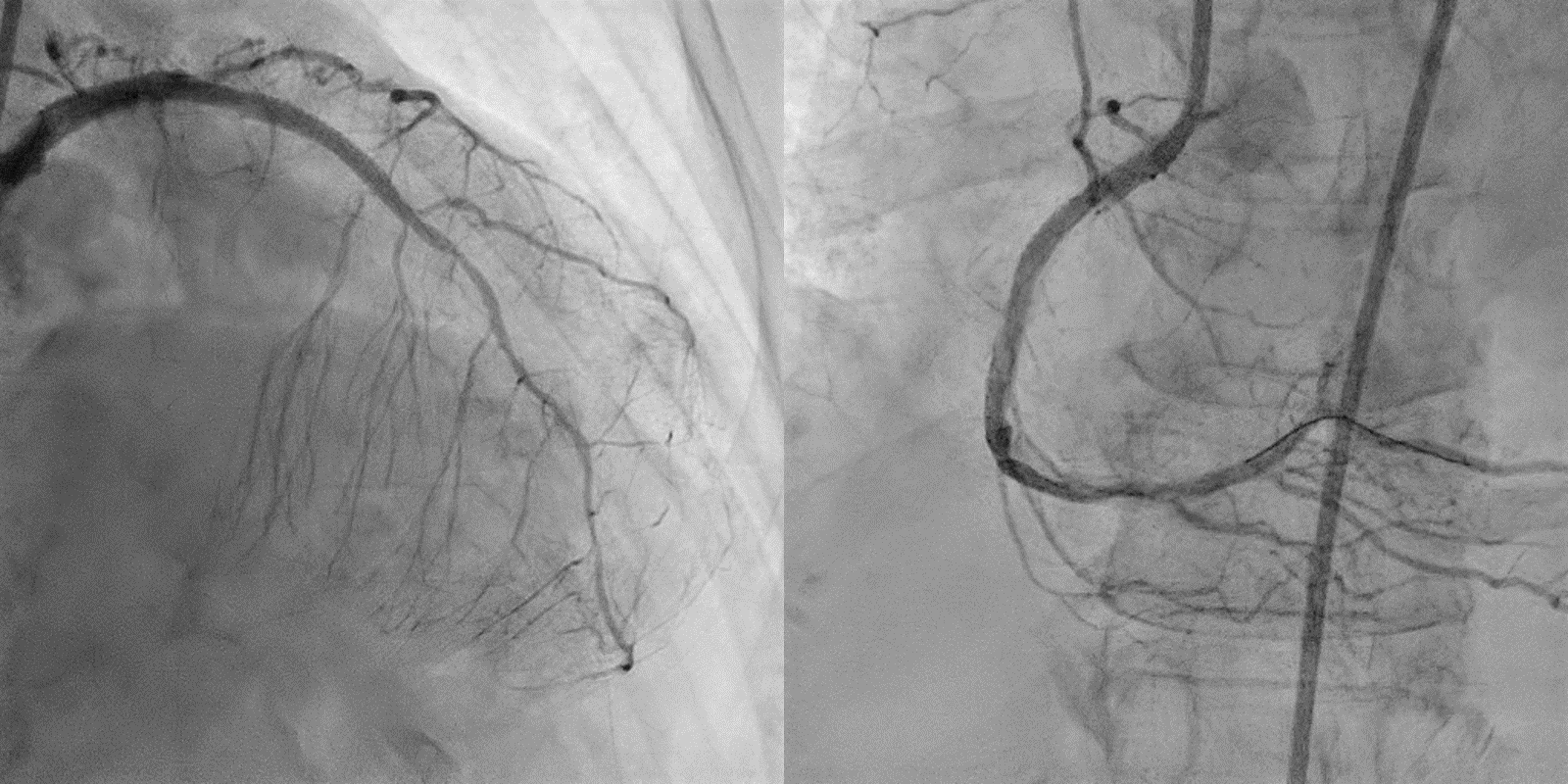
A 71 years female with underlying diabetes, hypertension hyperlipidemia, Presented with STE inferior MI, referred to our center for PPCI. Echo: EF 55% inferior wall hypokinesia. Angiogram: Tight distal LMS stenosis, calcified diffuse LAD disease, calcified with tight lesion proximal and dLAD. Planed for immediate IABP insertion and urgent as in-patient CABG. Before IABP insertion, aortogram showed calcified and bilateral severe aorto-iliac stenosis.

Relevant Test Results Prior to Catheterization
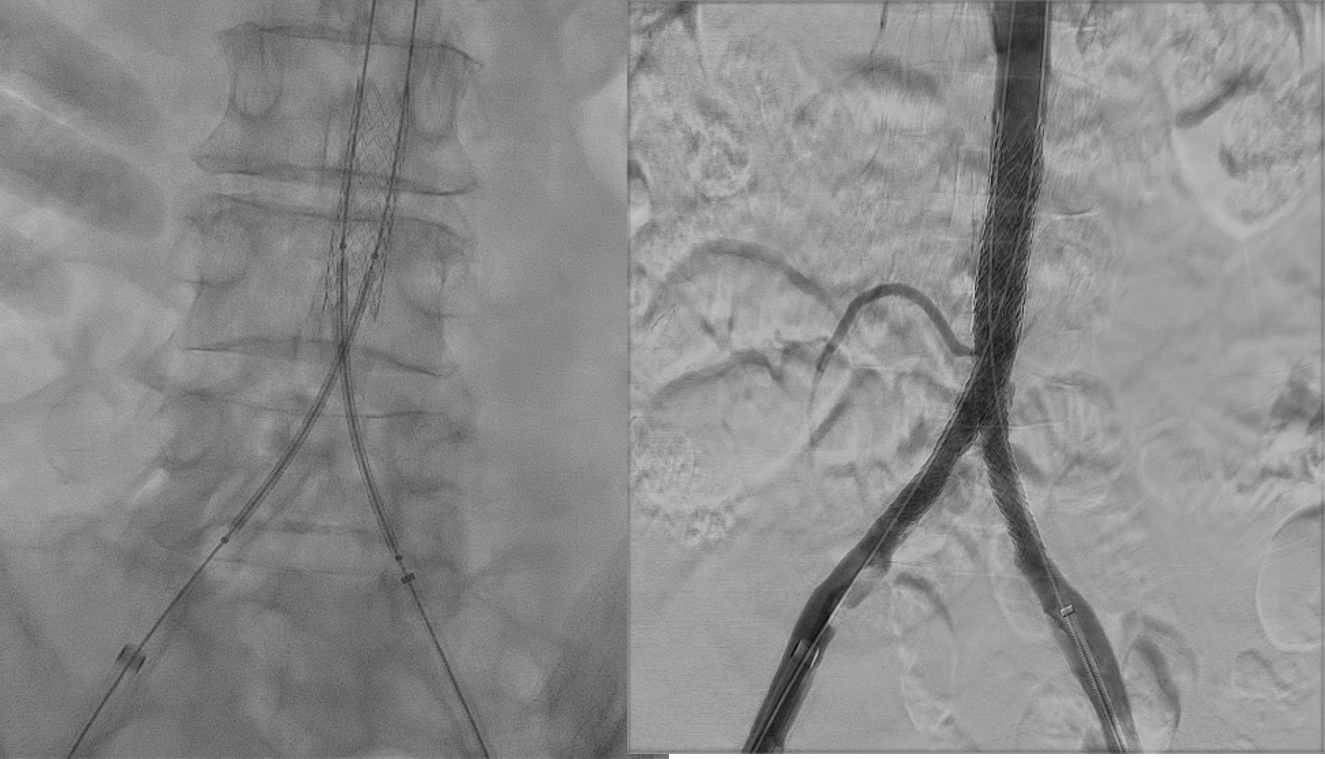
Surgical team advised to fix her PVD. PTA aortoiliac done prior to CABGstented Aorta & both Iliac arteries
Relevant Catheterization Findings
, but 2 days later developed UTI, surgery was postponed waiting infection to clear. while waiting for CABG,, she developed STE posterior-inferior MI with pulmonary edema and pneumonia (HAP). Urgent CABG was postponed waiting chest infection to clear. She continued to have chest pain, BP dropped & required Inotrope support, trop T went up 5000 Patient she was counselled for high risk PCI vs waiting CABG
Interventional Management
Procedural Step
patient was brought for urgent high risk angioplasty via LFA for IABP insertion & RFA for PCI using EBU 3.0/7F. decided for upfront Rotablator because IVUS cath couldn't pass across the pLAD lesion. Rotapro 1.5 Burr at 80000rpm/ 5runs from LMS to mLAD. Then predilated with Predilated with scorflex 2.5/15 & 3.0/ 15.Stented mLAD to pLAD, DES 2.5/28, Up sized with NC 3.0/15, Stented pLAD to ostial LMS ,DES 3.5/28,Upzised at LAD with NC 3.5/12, And POT LMS NC 4.0/8. PCI to RCAJR catheter 6F , upfront Rota burr 1.5 @180rpm/4 runs to proximal to mid RCA. Then predilated with scoreflex 2.5/15. Stented pRCA up to ostium with DES 3.0/28, Upsized with 3.5/15.DCB mRCA with 3.0/30.
Case Summary
Post procedure was pain free, discharged home well after 2 days.
take home massage
take home massage
Managed to fix Aorto-iliac stenosis and the severe coronary lesion.
Right timing and correct decision to intervene.
The use of upfront Rota for proper and fast lesion preparation.
Angioplasty and be a good option and bailout procedure for LMS/LAD disease when surgery is impossible.