
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-145
More Than Meets the Eye, The Role of Imaging in Calcified Lesion and Drug Coated Balloon
By Puti Sarah Saus
Presenter
Puti Sarah Saus
Authors
Puti Sarah Saus1
Affiliation
Metropolitan Medical Centre, Indonesia1,
View Study Report
TCTAP C-145
Coronary - DES/BRS/DCB
More Than Meets the Eye, The Role of Imaging in Calcified Lesion and Drug Coated Balloon
Puti Sarah Saus1
Metropolitan Medical Centre, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
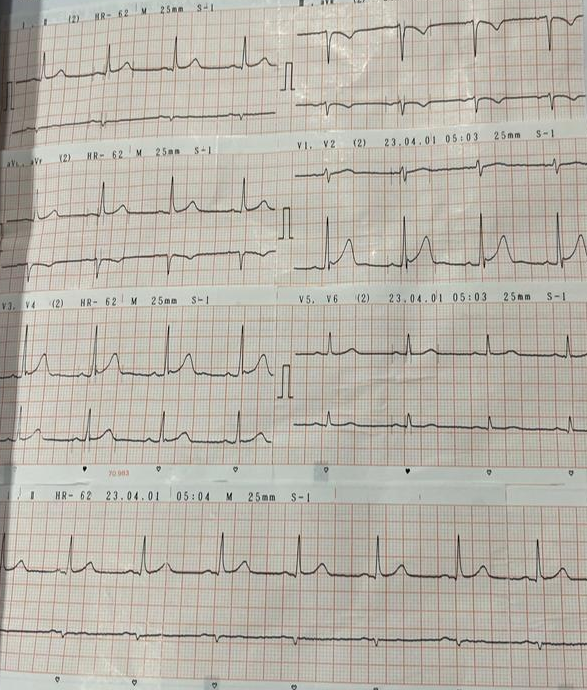
a 53 years old male came to the out patient clinic with a complaint of progressif angina and diaphoresis 1 month prior. His risk factor was uncontrolled hypertension. His physical examination was within normal limits. His Ecg findings was : T inversion in Inferior leads.His Chest X-ray was : NormalHis Laboratory was : CKMB : 15.8 / Hs Trop T 23.57
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
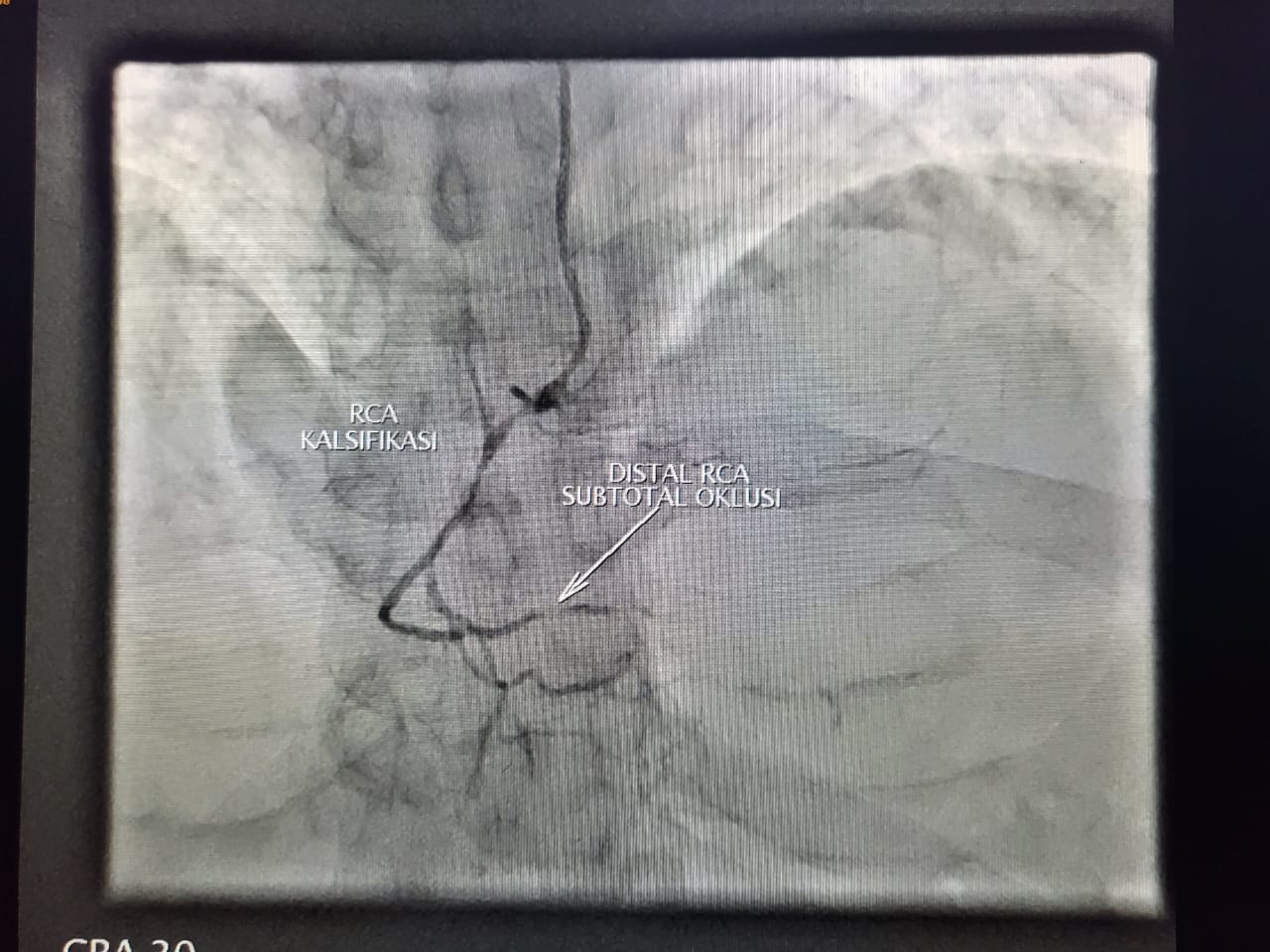
LM : Normal LAD : 50-70% proximal long lesion with Mild- moderate calcification LCX : 50-60% Proximal stenosis and CTO at distalRCA : non dominan, small vessel, moderate - heavy calcification, distal subtotal occlusion ( TIMI 2 flow )


Interventional Management
Procedural Step
Guiding cath XB 7F/3.5 to LCA, wire SION inserted to distal LCX, the wire could penetrate the lesion. we continued to predilate with EUPHORA ballon 2.0 x 15 mm, inflated at 12 atm. we did IVUS run pre PCI:MLA distal : 2.06 mm with fibro calcification and 81% plaqueMLA prox : 4.0 mm with fibro calcificationafterward we did ballooning with Magic TOUCH DEB 2,5 x 30 mm inflated at 6 atm for 1.34 minute at distal LCX and did predilatation with SCOREFLEX NC 3.0 X 15 mm inflate it at 16-18 atm and double wire with SION to OM1 and did stenting with SYNERGY 3,5 X 32 mm at proximal LCX inflate at 12- 14 atm.
IVUS run MSA prox : 7.82 ( 2.79- 3.45 mm ) stent well apposed, no stent edge dissection, no residual trombus.
PCI to LM-LAD : did wiring to distal LAD did IVUS run to LAD : MLA 1.6 mm superfisial concentric calcified plaque > 270 degree
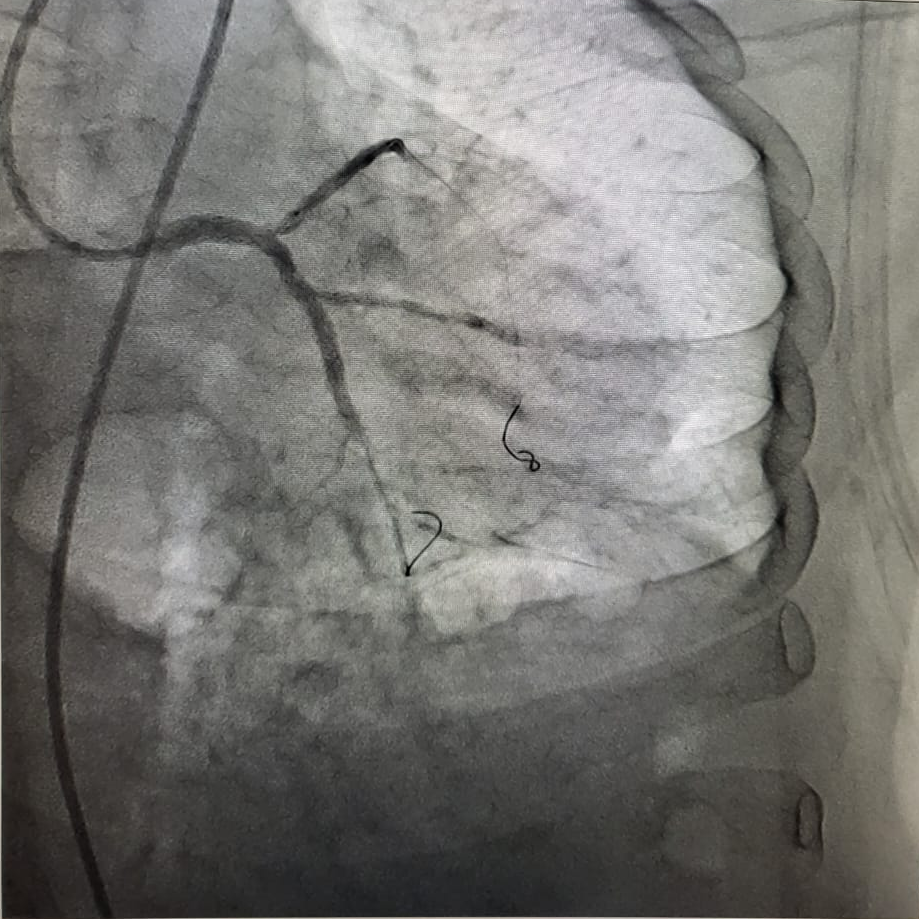
We did predilatation with SCOREFLEX NC 3.0 x 15 mm, inflate at 16-18 atm, continue ballooning with WOLVERINE 3,5 X 15 mm, inflated 10-14 atm at LM-LAD , and then stenting with SYNERYGY 3.0 x 28 mm inflated at 11- 20 atm proximal LAD and SYNERGY 4.0 X 24 mm at 12- 20 atm overlapping. we did POT with NC EUPHORA 5.0 X 12 atm inflate at 14-16 atm.
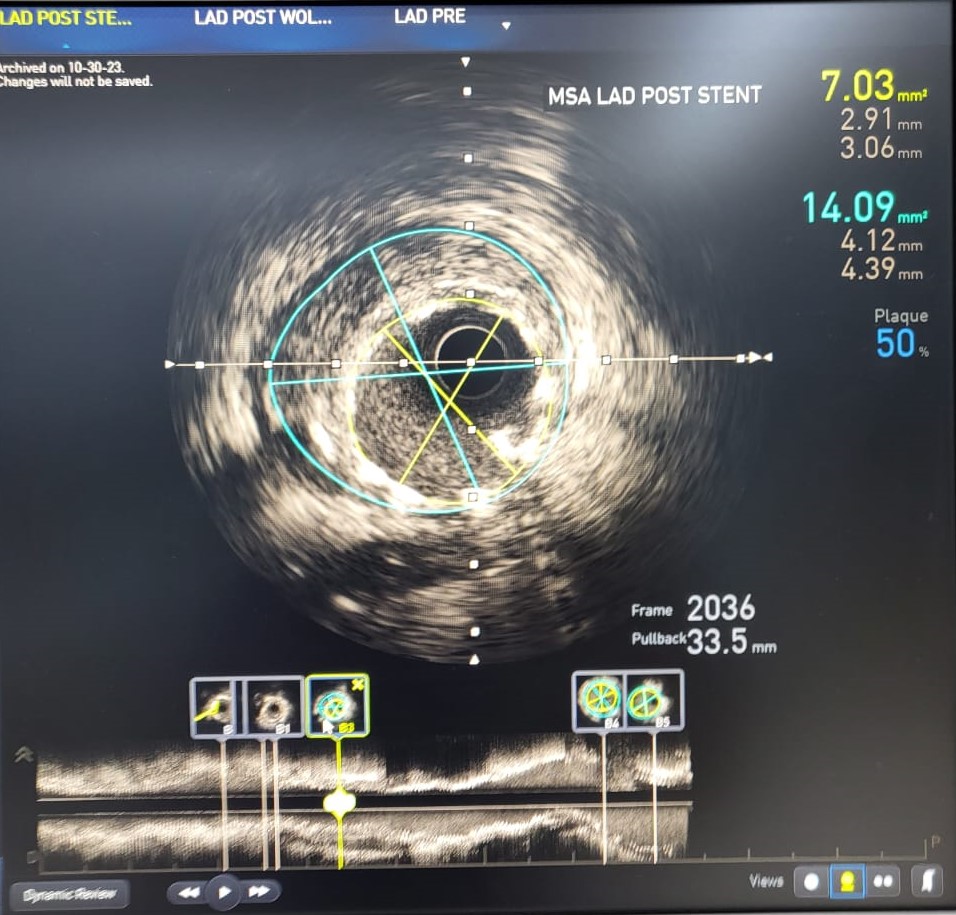
IVUS run post PCI : MSA LAD : 7.03- 14.09 mm ( 2.91- 4.39 mm)MSA distal LM : 16.81 - 26.60 mm MSA proximal LM : 16.26 - 22.62 mmStent well apposed, no stent edge dissection, no residual trombusresidual stenosis < 20% distal LCX

IVUS run MSA prox : 7.82 ( 2.79- 3.45 mm ) stent well apposed, no stent edge dissection, no residual trombus.
PCI to LM-LAD : did wiring to distal LAD did IVUS run to LAD : MLA 1.6 mm superfisial concentric calcified plaque > 270 degree
We did predilatation with SCOREFLEX NC 3.0 x 15 mm, inflate at 16-18 atm, continue ballooning with WOLVERINE 3,5 X 15 mm, inflated 10-14 atm at LM-LAD , and then stenting with SYNERYGY 3.0 x 28 mm inflated at 11- 20 atm proximal LAD and SYNERGY 4.0 X 24 mm at 12- 20 atm overlapping. we did POT with NC EUPHORA 5.0 X 12 atm inflate at 14-16 atm.
IVUS run post PCI : MSA LAD : 7.03- 14.09 mm ( 2.91- 4.39 mm)MSA distal LM : 16.81 - 26.60 mm MSA proximal LM : 16.26 - 22.62 mmStent well apposed, no stent edge dissection, no residual trombusresidual stenosis < 20% distal LCX
Case Summary
Dealing with calcified lesion, lesion preparation is very important. Imaging modalities is one of the standard requirement to have in pursuing such lesion whether to hinder under deployment of stent, dissection or preventing trombus formation. Other than imaging, debulking calcified lesion or plaque modification is a must. Nowadays the use of Drug Coated Balloon increases with great result, and imaging play an important role to deliver great results.