
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-065
LMT True Bifurcation Lesion and Reocclusion in Mid LAD After DES Removal due to DCA Catheter
By Mayu Sakuma, Yuji Oikawa, Koichiro Hori, Mikio Kishi, Hiroto Kano, Shunsuke Matsuno, Junji Yajima
Presenter
Mayu Sakuma
Authors
Mayu Sakuma1, Yuji Oikawa1, Koichiro Hori1, Mikio Kishi1, Hiroto Kano1, Shunsuke Matsuno1, Junji Yajima1
Affiliation
The Cardiovascular Institute, Japan1,
View Study Report
TCTAP C-065
Coronary - Complex PCI - CTO
LMT True Bifurcation Lesion and Reocclusion in Mid LAD After DES Removal due to DCA Catheter
Mayu Sakuma1, Yuji Oikawa1, Koichiro Hori1, Mikio Kishi1, Hiroto Kano1, Shunsuke Matsuno1, Junji Yajima1
The Cardiovascular Institute, Japan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
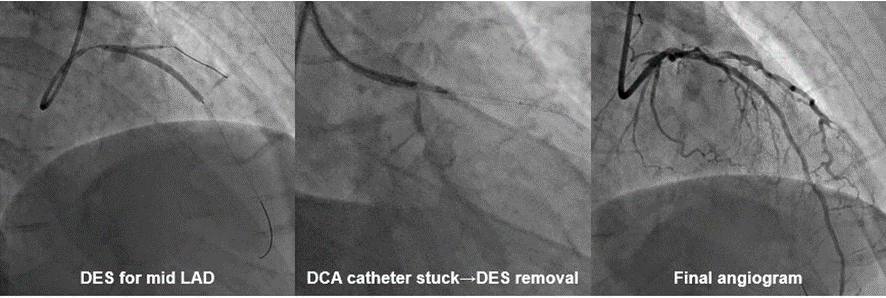
A 50's male developed a STEMI eight months ago. An Emergency CAG revealed total occlusion of mid LAD and moderate stenosis of LMT to proximal LAD. At that time, DES was implanted for mid LAD. One month later, staged PCI was attempted for LMT-LAD. However, a DCA catheter got stuck with the implanted stent, and the stent was removed together with the DCA catheter. Due to luminal enlargement without significant vessel injuries, the procedure was terminated after the application of DCB for LMT-LAD.
Relevant Test Results Prior to Catheterization
Electrocardiogram revealed QS pattern and terminal T inversion in V1-4 leads. Echocardiography showed LV ejection fraction was 44% with anterior wall hypokinesis. Renal function was normal limits on laboratory data.
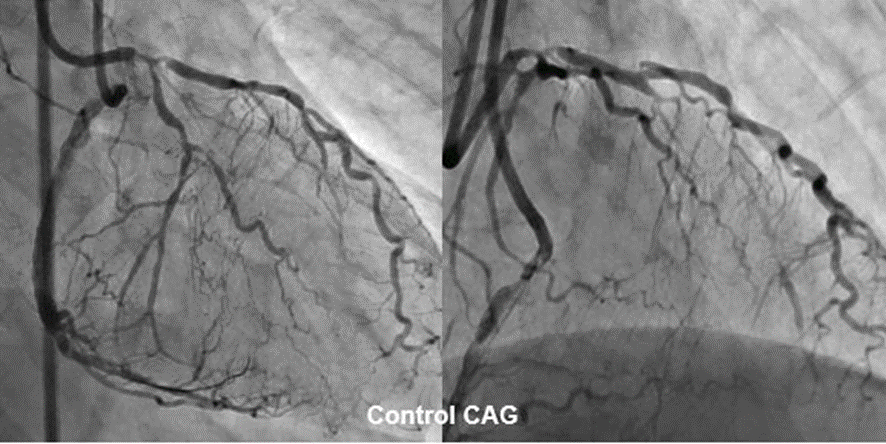
Relevant Catheterization Findings
Seven months later, a follow-up coronary angiogram was performed. The angiogram revealed no significant stenosis in the RCA, severe stenosis lesion at the true bifurcation of LMT, and reocclusion in mid LAD. The CTO entry is shown to be tapered type, and septal collaterals from PDA to LAD.

Interventional Management
Procedural Step
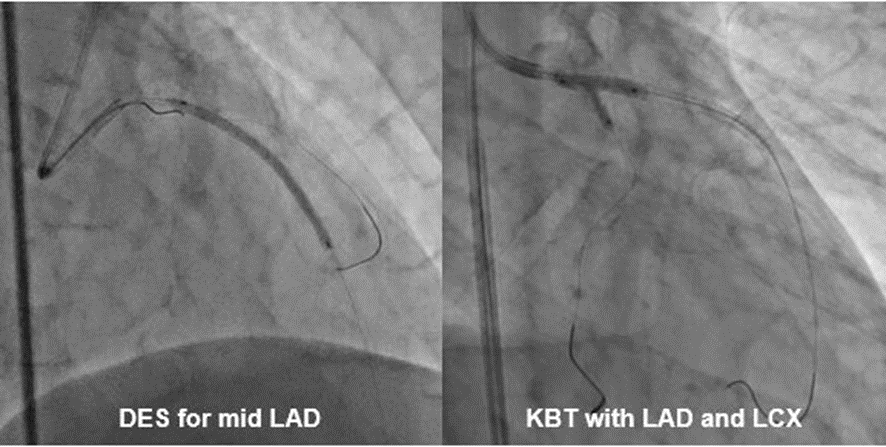
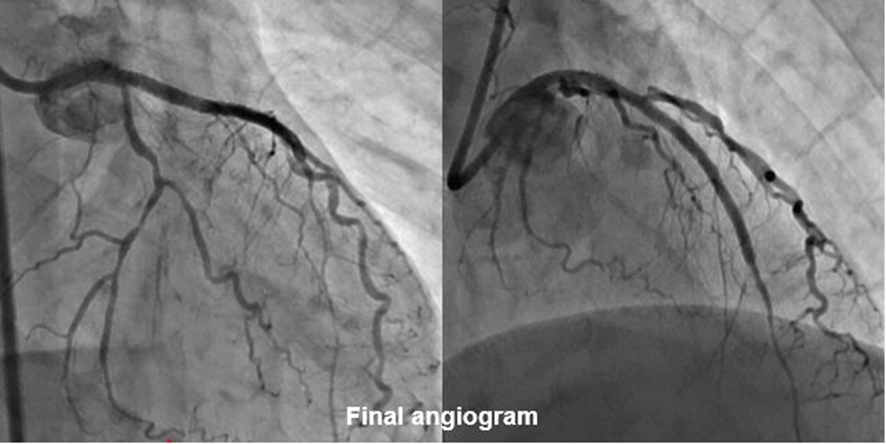
The strategy involved using an 8F guiding catheter and attempting antegrade wiring for the LAD-CTO, followed by a rescue retrograde approach procedure. We used IABP from the beginning due to severe stenosis at LMT. Initially, LAD and LCX were wired using a dual lumen catheter, and dilated LMT bifurcation with KBT. Next, the antegrade wiring with the XT-R failed to pass the mid LAD-CTO lesion, so we switched to Gaia Next 1 and successfully achieved antegrade wiring. The CTO was sequentially predilated with 2.5mm balloon, and 2.5mm DES stent was deployed at the CTO lesion. The proximal LCX was dilated with 2.5mm balloon, and 3.5mm DES stent was deployed at the LMT-LAD lesion. The LCX wire was recrossed, and final KBT was performed using 3.0mm balloon in the LMT-LAD and 2.5mm balloon in the proximal LCX. Finally, DCB was used at LCX ostium.
Case Summary
In this case, the DCA catheter became trapped in the implanted stent, resulting in the removal of both. A few months later, a coronary angiogram revealed a CTO at the same site, which was successfully treated using an antegrade approach. There was also severe stenosis at the LMT bifurcation, and the use of an IABP from the beginning allowed the procedure to be performed with stable circulatory dynamics. Finally, the treatment could be completed with a single stent over the LMT-LAD.