
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-132
Longitudinal Stent Deformation During Radial Approach : Retrieval Through Radial Access Was Not an Option
By Joel Herbet, Dafsah Arifa Juzar, Doni Firman, Amir Aziz Alkatiri, Arwin Saleh Mangkuanom, Nanda Iryuza
Presenter
Joel Herbet
Authors
Joel Herbet1, Dafsah Arifa Juzar1, Doni Firman1, Amir Aziz Alkatiri1, Arwin Saleh Mangkuanom1, Nanda Iryuza1
Affiliation
National Cardiovascular Center Harapan Kita, Indonesia1,
View Study Report
TCTAP C-132
Coronary - Complication Management
Longitudinal Stent Deformation During Radial Approach : Retrieval Through Radial Access Was Not an Option
Joel Herbet1, Dafsah Arifa Juzar1, Doni Firman1, Amir Aziz Alkatiri1, Arwin Saleh Mangkuanom1, Nanda Iryuza1
National Cardiovascular Center Harapan Kita, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
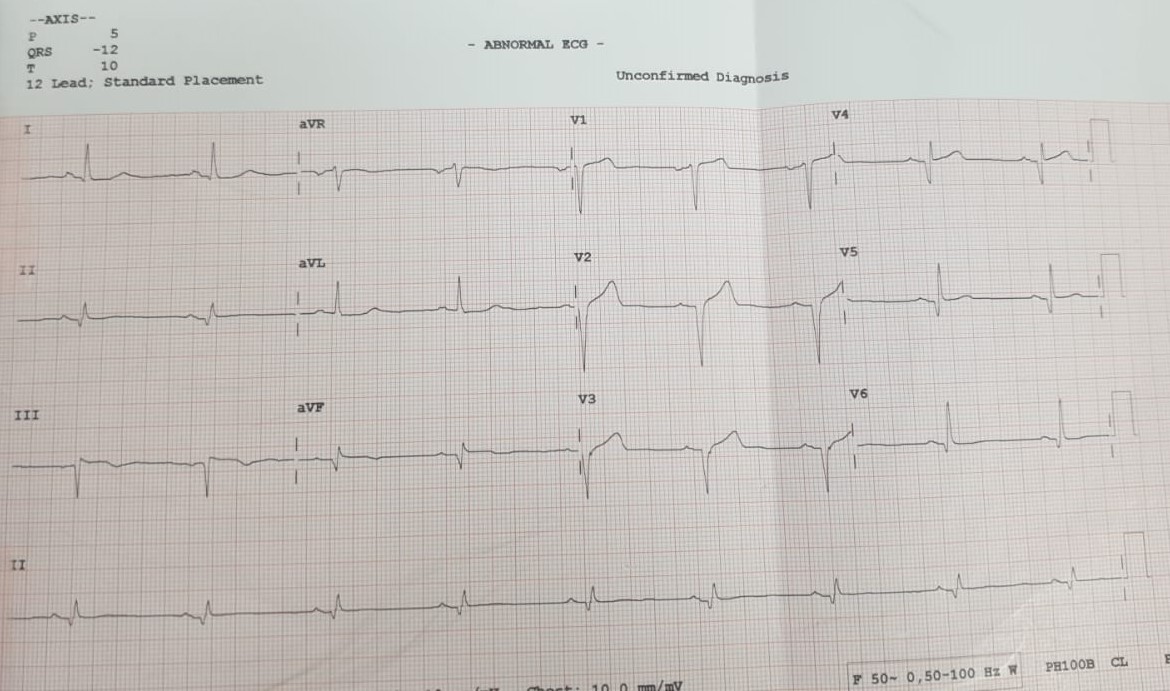
Mr. EPSA 45 years old, heavy smoker, presented to emergency room with chest pain that had persisted for 2 hours prior to admission. First chest pain was felt 3 days ago. He was diagnosed with inferior ST Elevation Myocardial Infarction (onset >48 hour). His vital signs upon arrival at the ER were a blood pressure of 110/75 mmHg and a heart rate of 56 bpm. There were no rales and his peripheral perfusions were normal.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
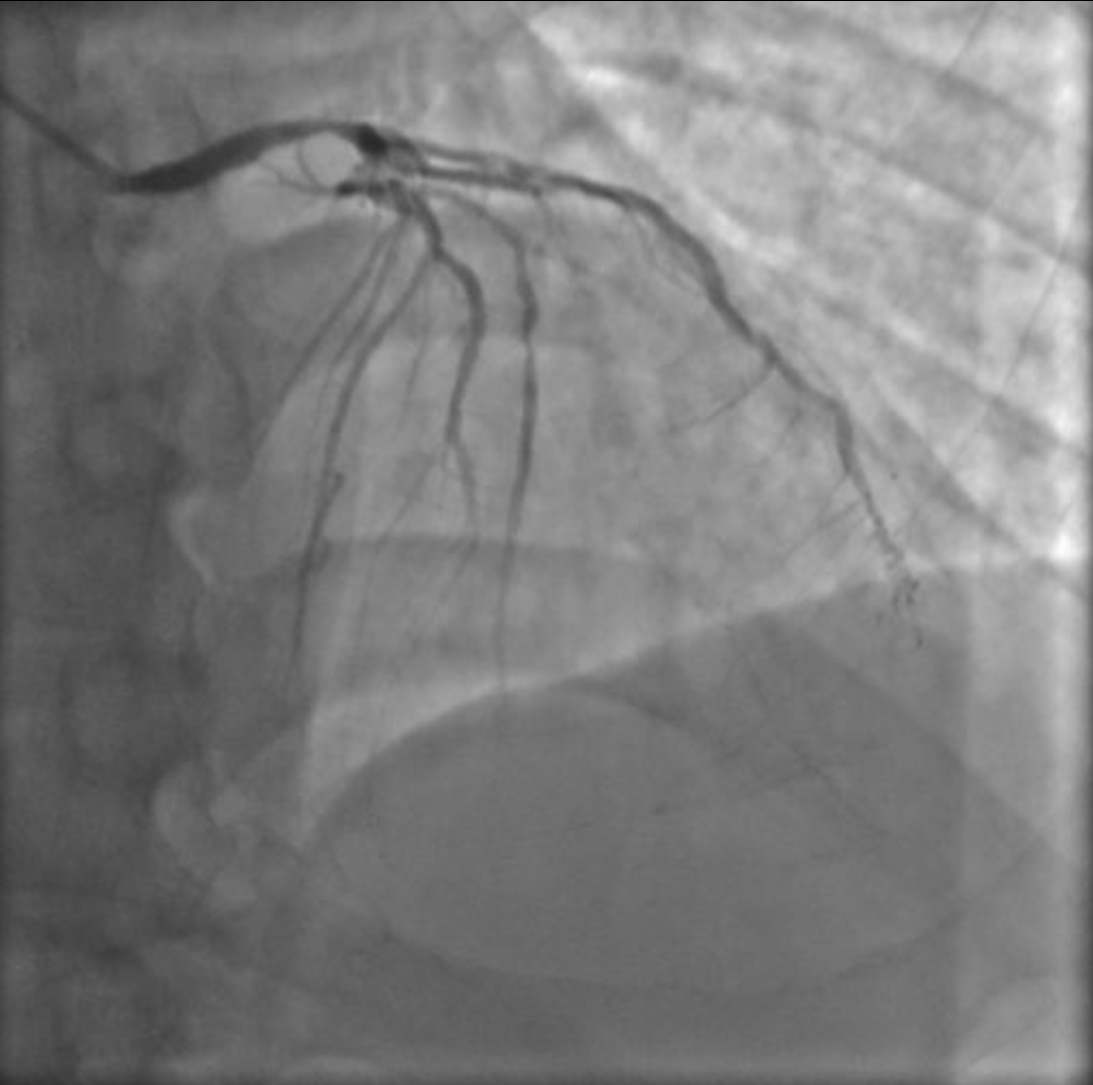
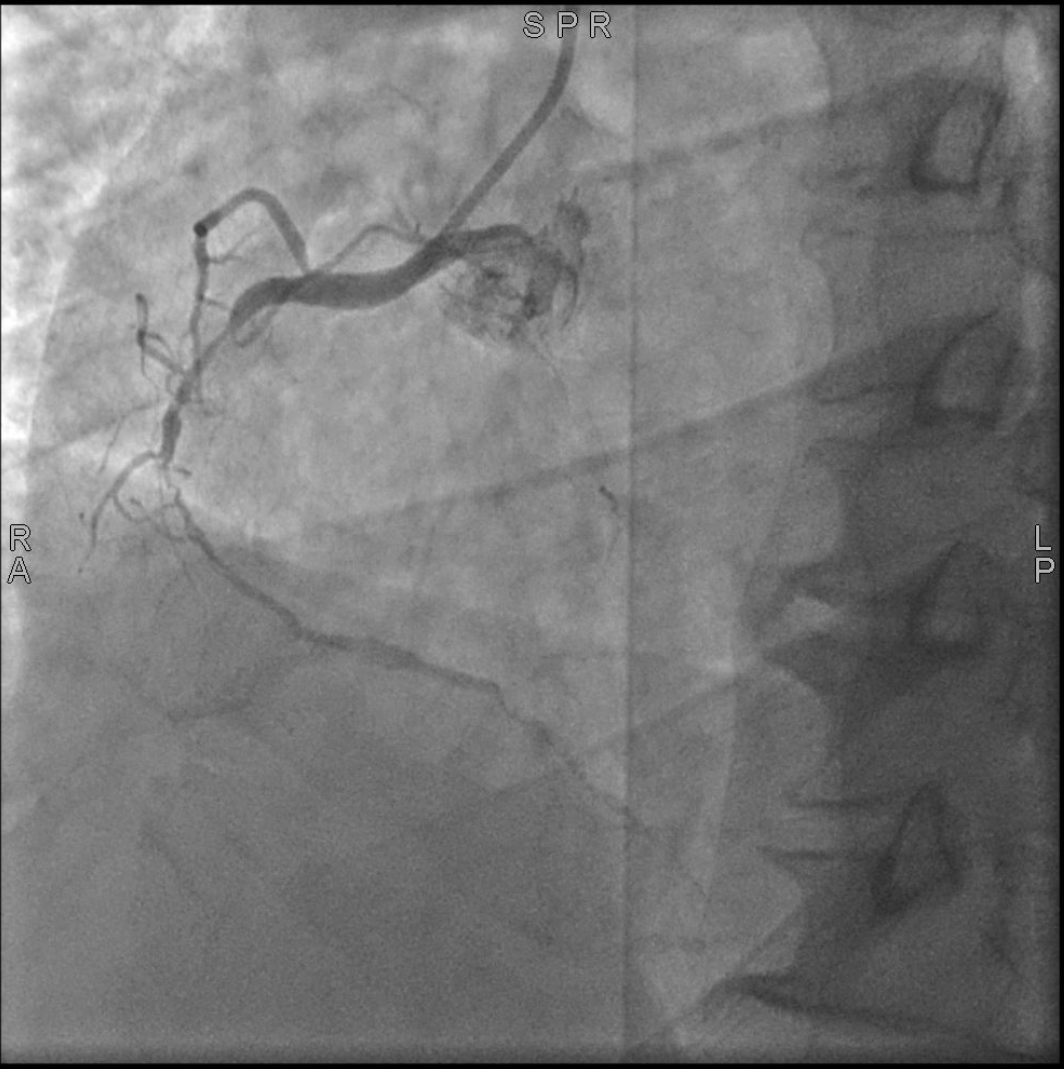
Using Optitorque 5Fr diagnostic catheter via 6Fr radial sheath :Left Main : Senosis 70% at distalLAD : Diffuse stenosis 80% at proximal to distalLCx : Total Occlusion at distal, flow at distal from RCA (Rentrop II)RCA : Dominan, diffuse stenosis from proximal to distal, total occlusion at distal PL, flow to distal from LAD (Rentrop III)

Interventional Management
Procedural Step
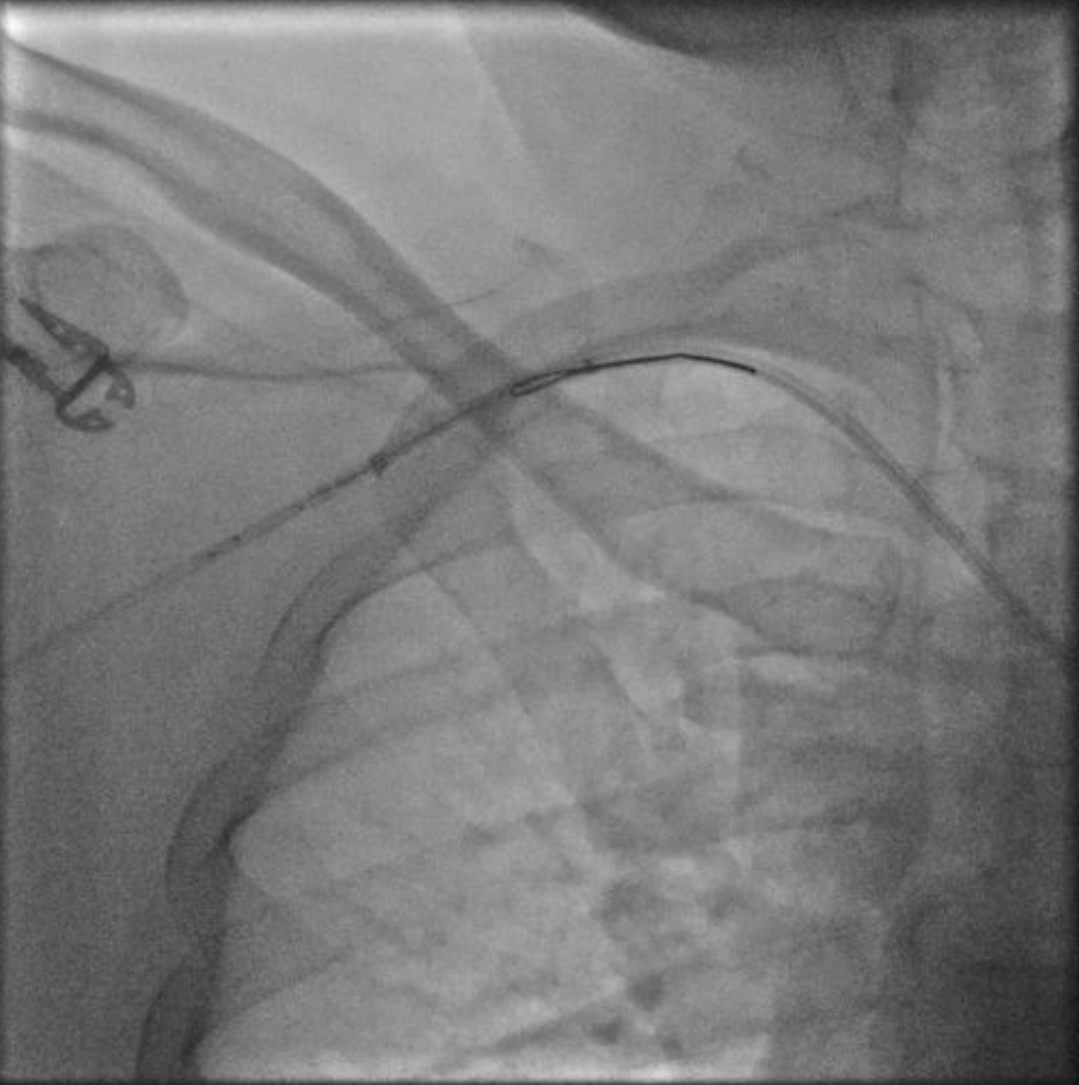


Case Summary
Longitudinal stent compression is one of the rare complications of PCI. In these primary PCI case, the stent compresses as it is retracted into the guide catheter because the guide tip reshapes from circular to various shapes when inserted too deeply to the wedge coronary artery lesion. We decided to perform femoral snaring because compressed stents can injure the brachial and radial arteries. In addition, the changing diameter of the stent due to compression will have difficult passing through the 6Fr radial sheath. Finally it can be overcome by using a loop wire technique from contralateral access and stent can be pulled out through the femoral artery.