
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-166
Unraveling the Bridge: How an Invasive Exercise Test Gives a New Perspective to Myocardial Bridging
By Wishnu Aditya Widodo, Teuku Muhammad Haykal Putra
Presenter
Wishnu Aditya Widodo
Authors
Wishnu Aditya Widodo1, Teuku Muhammad Haykal Putra1
Affiliation
Jakarta Heart Center, Indonesia1,
View Study Report
TCTAP C-166
Coronary - Imaging & Physiology - FFR
Unraveling the Bridge: How an Invasive Exercise Test Gives a New Perspective to Myocardial Bridging
Wishnu Aditya Widodo1, Teuku Muhammad Haykal Putra1
Jakarta Heart Center, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
This is a case of a 50-year-old male who was employed by an international oil and gas company. He had a history of unstable angina pectoris and had previously undergone elective PCI to the RCA. During a routine yearly medical checkup, a positive result emerged from a treadmill test, prompting the company to seek a cardiac consultation and inquire about the patient's eligibility for fieldwork.

Relevant Test Results Prior to Catheterization
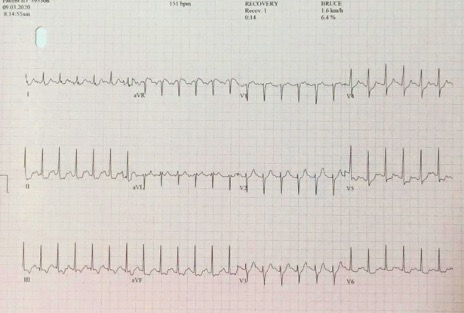
The treadmill test revealed a maximum exercise time of 09:31 minutes on the Bruce Protocol, reaching 89% of the target maximum heart rate. An ischemic response was evident, characterized by a 2 mm upsloping ST depression on lead II, III, aVF, v4-v6.
Relevant Catheterization Findings
Coronary angiography and invasive physiology study were done. The RCA stent remained patent, LAD myocardial bridging was notable, and there was borderline stenosis in LCx



Interventional Management
Procedural Step
LCx physiology evaluation yielded nonsignificant results with a Resting Fractional Reserve (RFR) value of 0.96. Subsequently, a pressure wire was inserted across the myocardial bridging segment in the LAD, and a small cycling device was affixed to the cathlab table. The patient cycled with the wire still on the coronary, achieving 80% of the maximum heart rate. Significant physiological changes were recorded, with the RFR value dropping from 0.80 to 0.62. This finding confirmed the substantial impact of physical exercise on the myocardial bridging segment.



Case Summary
We recognize various methods for assessing significant occlusion in invasive coronary physiology studies. The standard procedure, inducing maximum hyperemia with adenosine, may not offer the same insights in dynamic stenosis like myocardial bridging. Pharmacological provocation with inotropes, such as dobutamine, could be used but comes with caveats due to vasodilating effects. Here, we demonstrate simultaneously conducting a physical exercise test with an invasive physiology study, offering potential for more physiologic, relatable results to explain a positive treadmill test.