
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-056
Success After Several Twists and Turns for RCA CTO
By Yen-Lien Chou
Presenter
Yen-Lien Chou
Authors
Yen-Lien Chou1
Affiliation
Tri-Service General Hospital, Taiwan1,
View Study Report
TCTAP C-056
Coronary - Complex PCI - CTO
Success After Several Twists and Turns for RCA CTO
Yen-Lien Chou1
Tri-Service General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
• 74-year-old man, smoker (0.5PPDfor 50 years)
• HCVD and Hyperlipidemia
• Chest pain&tightnessfor1 month andrelievedby sublingual NTG
• Besides,dyspnea on exertion (walking)was also identified
Relevant Test Results Prior to Catheterization
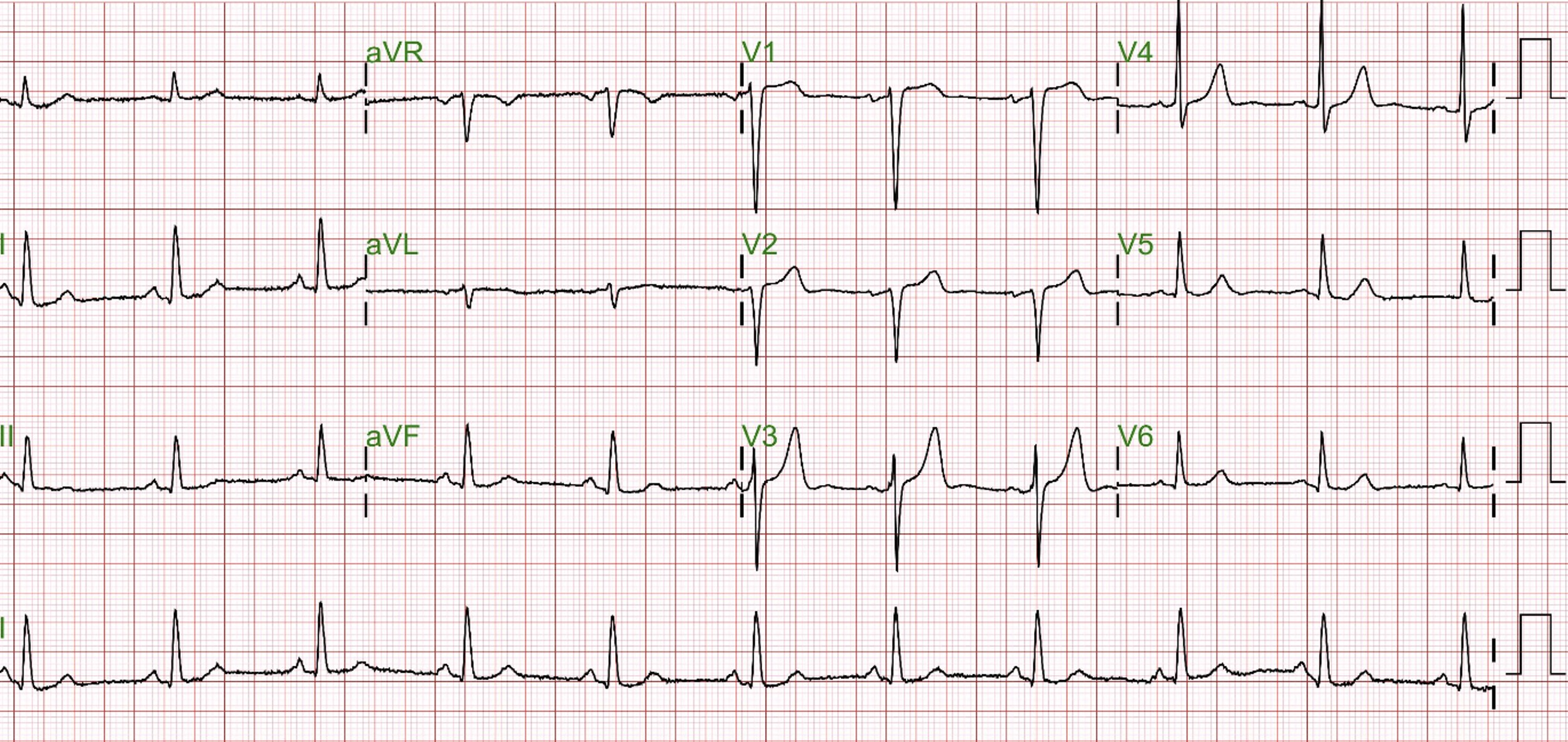
1120427 ECG: Sinus rhythm, Q wave over V1-V21120427 CXR: normal heart border and no active lung diseaseTl-201 myocardial perfusion scan: 20% of LAD and 50%of RCA territory in stress phaseEchocardiography: preserved LVSf with EF: 65%, mild AR, moderate MR, mild TR, and PAP: 30mmHgHDLC 52;LDLC 59;GLU 91;TCHO 126;TG 84;BUN 14;CREA 1.0;UA 8.1;AST 23;ALT 17;NA 141;KS 4.3;HBA1C 5.7;BNP 177.3

Relevant Catheterization Findings
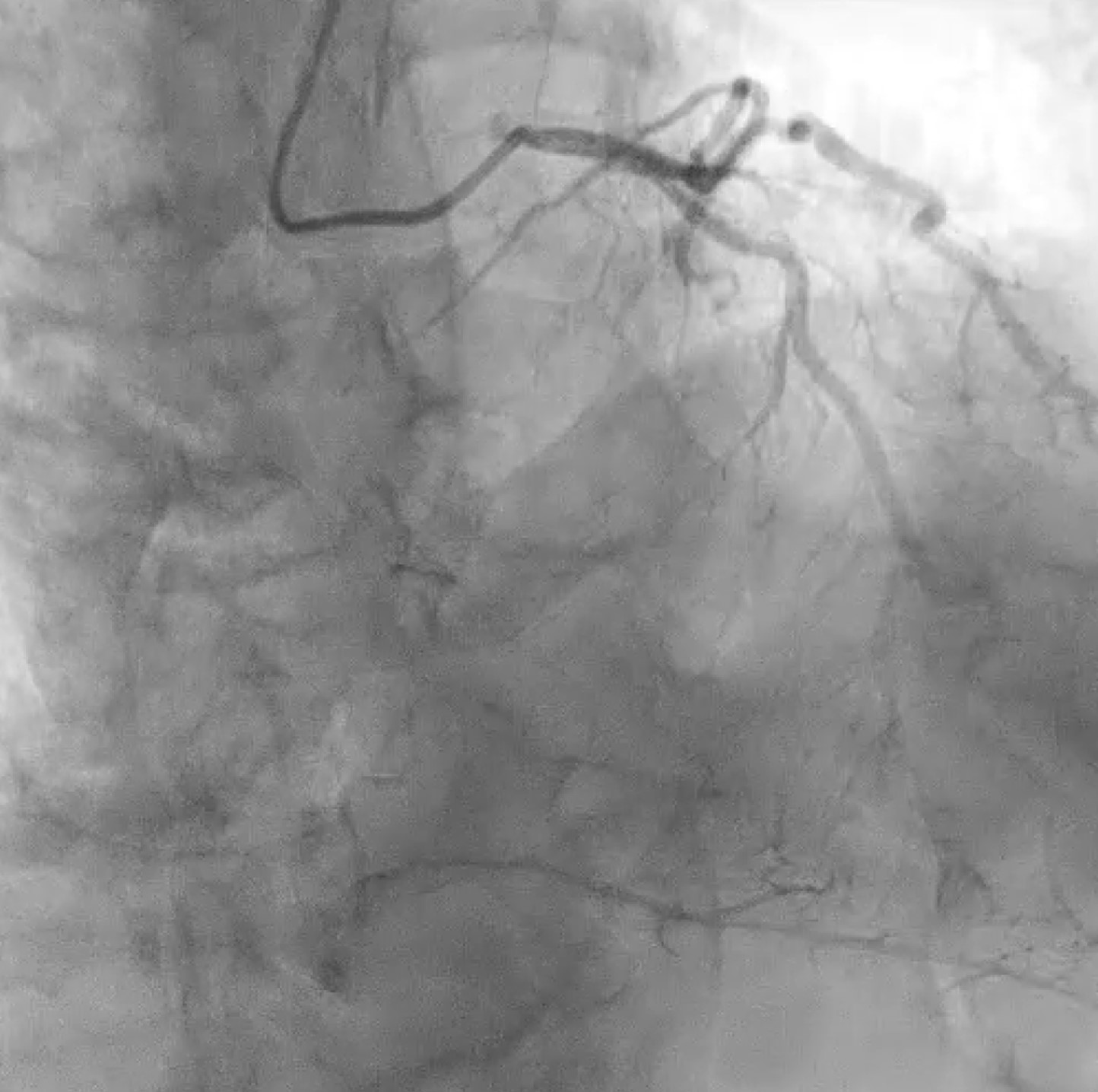
LMCA: Atherosclerosis- M/3 to D/3: Tubular eccentric 50% stenosis, Medina (1,1,1)LAD: Atherosclerosis- Ostium to P/3: Diffuse eccentric 50-70% stenosisLCx: Atherosclerosis- Ostium to P/3: Diffuse eccentric 50-90% stenosisRCA: Atherosclerosis and calcification- P/3: Chronic total occlusion - Ostium to D/3 of PDA: diffuse eccentric 50-80% stenosis with smal caliber- Ostium of D/3 of PL: diffuse eccentric 50-80% stenosis with - Receiving collateral flow from septal perforator to m to d-RCA


Interventional Management
Procedural Step
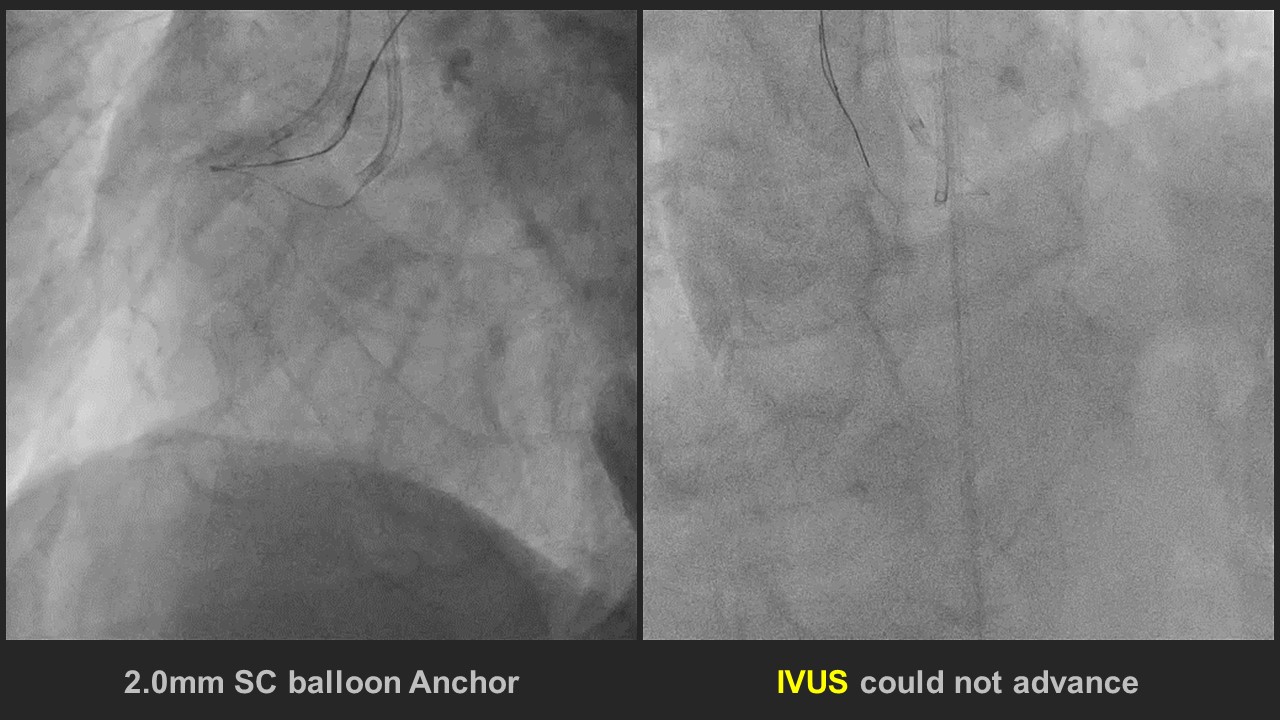
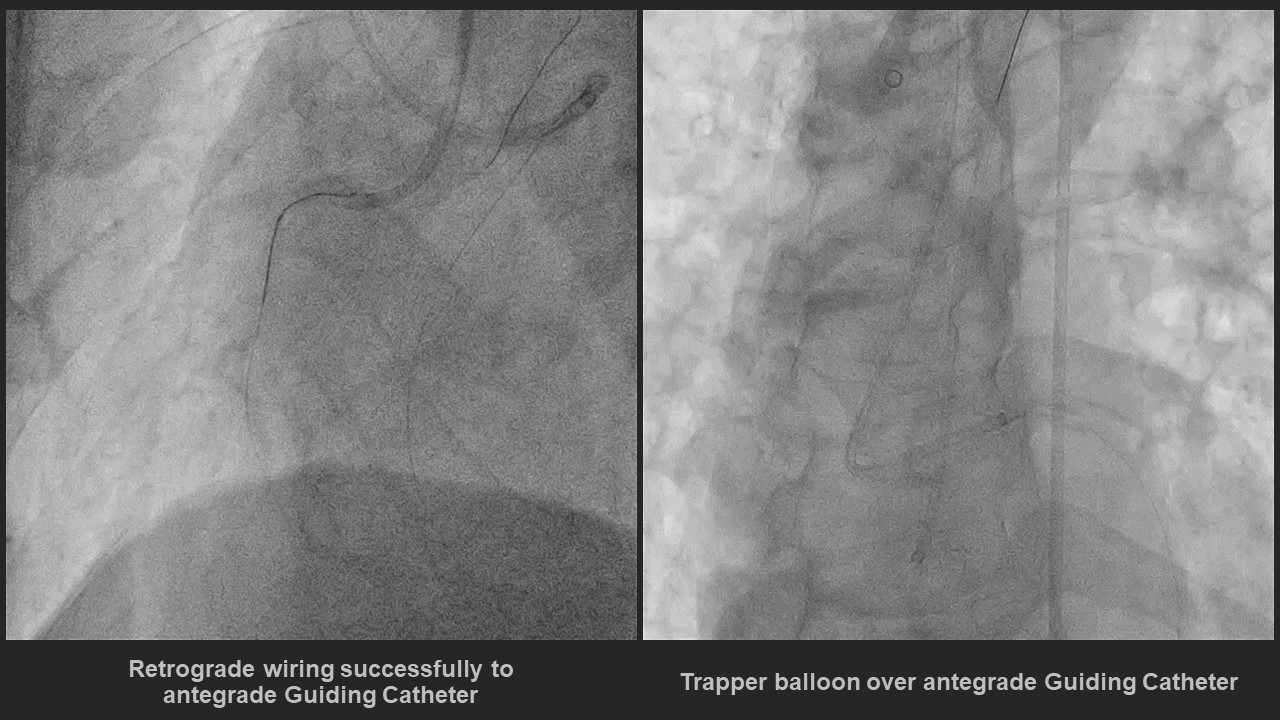
Ping pong guide technique with two guiding catheters placed at RCA ostiumSion wire introduce to RCA and advanced to RV branchSionblue wire advanced to RV branch and lesion at RV branch dilated by 1.5mm balloonAnchor balloon technique at RV branch and IVUS introduce to RCA and plan to place before CTO lesion but failedSASUKE a9nd Crusade R placed at CTO lesion and XTA and Gaia I wire attack the CTO lesion but failedEBU 4.0 7F S.H. engaged to LMSionblack wire in Caravel advanced to distal septal branch from LADBroken Sion wire retrogradely advanced to PDA and wiring to p-RCA, but the Caravel failed to cross the critical lesion at p-RCA.Retrograded Sion wire wiring to telescope which at RCA ostium Retrograded Sion Black wire in JR guiding catheter was trapping by trapper balloon and Finecross advanced to JR guiding catheterSion wire shift to RG3 wire for externalizationLesion from d-RCA to p-RCA evaluated by IVUSLesion dilated by NC balloon and Cutting balloonLesion stented by 2 DES from d-RCA to os-RCA and post-dilatation was done by NC balloonLesion at PDA and PL dilated by a 1.5mm SC balloonFinal IVUS doneFinal angiography showed no residual stenosis from os-RCA to d-RCA with TIMI 3 flow

Case Summary
1. Bending angle > 45 degrees was difficult to wire from antegrade or retrograde
2. IVUS-guided puncture during stumpless CTO could be performed by Ping-pong guide technique
3. Guide extension catheter could be another method for direct retrograde wire cross at ostium to the proximal lesion to avoid into the false lumen (extension to aorta)
4. Trapping balloon technique in the antegrade guiding catheter may facilitate retrograde microcatheter advance smoothly to the antegrade guiding catheter for externalization