
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-207
Constrictive Pericarditis Due to Actinomycosis With Short Course Therapy and Drainage of the Collections: A Case Report
By Suphaphit Horadal, Surapun Pongsuthana
Presenter
Suphaphit Horadal
Authors
Suphaphit Horadal1, Surapun Pongsuthana1
Affiliation
Rajavithi Hospital, Thailand1,
View Study Report
TCTAP C-207
Heart Failure - Vascular Heart Disease and Cardiomyopathies
Constrictive Pericarditis Due to Actinomycosis With Short Course Therapy and Drainage of the Collections: A Case Report
Suphaphit Horadal1, Surapun Pongsuthana1
Rajavithi Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 43-year-old Thai man, a construction worker with chronic smoking and social alcohol drinking, was admitted because of right-side heart failure. The previous history noted for right lung mass suspected malignancy with acute pericarditis. On examination, the oral cavity noted numerous dental carries. Cardiovascular examination revealed the Kussmaul sign and pericardial knock. While waiting for a biopsy, He developed a painful fluctuant mass of the anterior chest wall without a sinus tract.

Relevant Test Results Prior to Catheterization
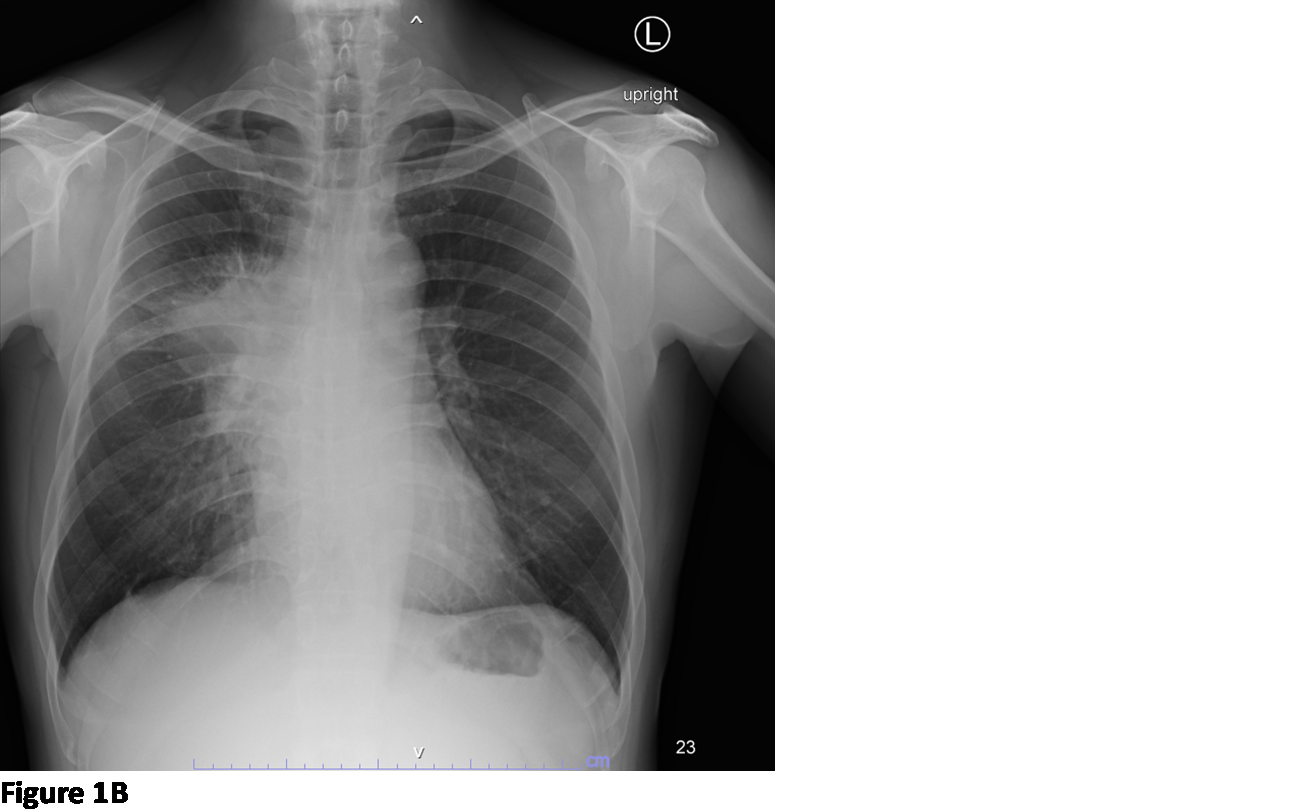
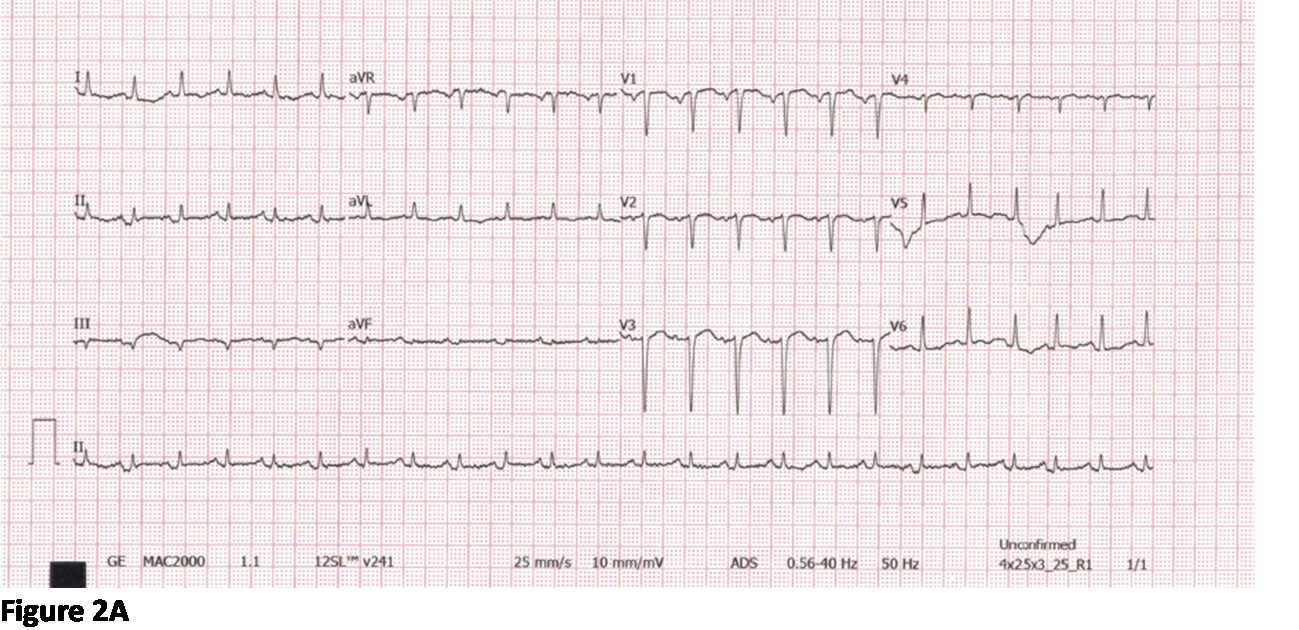
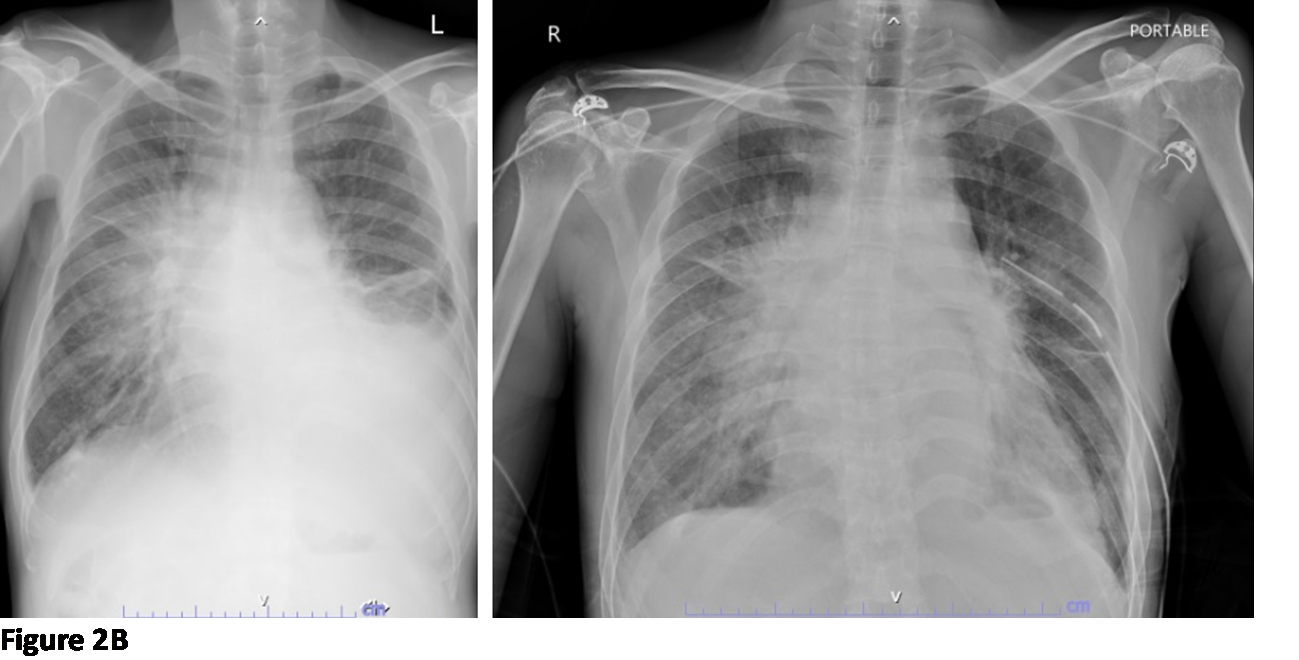
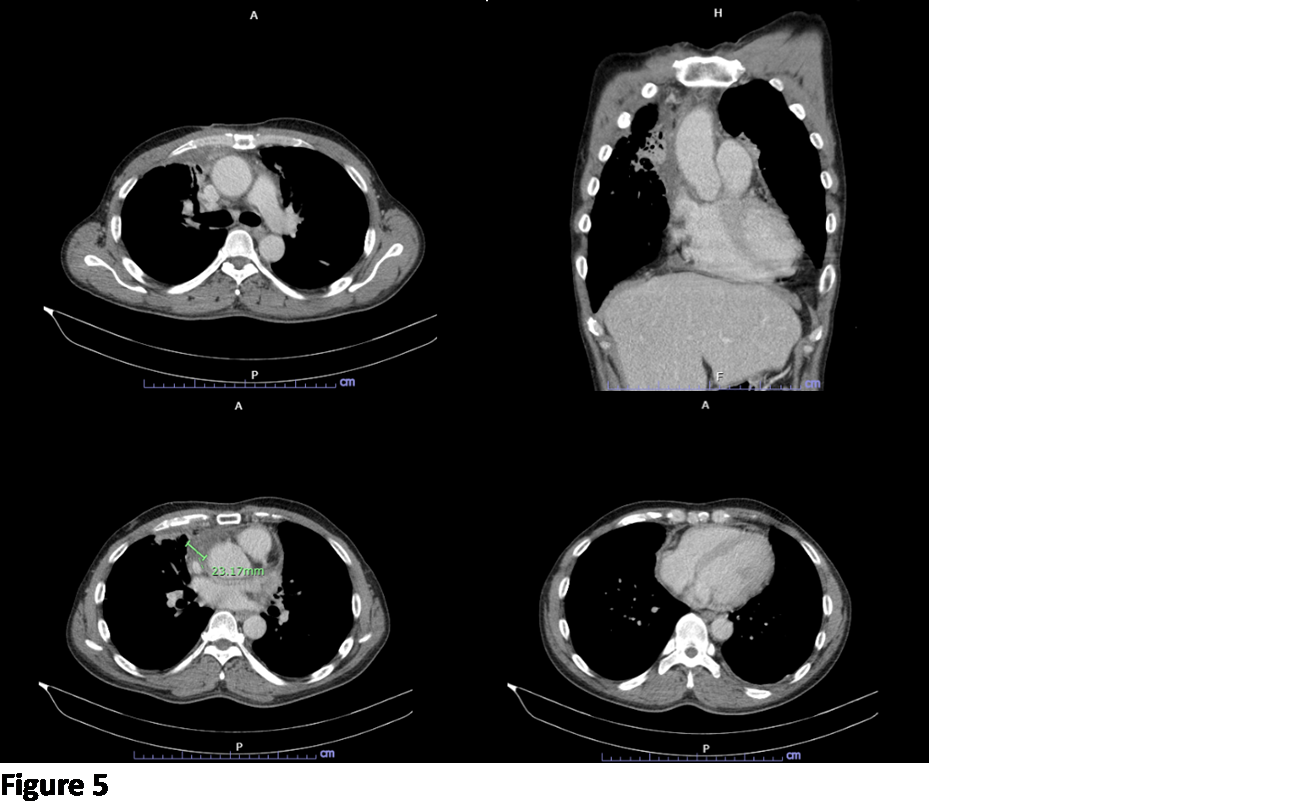
ECG demonstrated sinus tachycardia with no STT changes compatible with ECG staging of pericarditis. CXR showed an increased size of right lung mass with a moderate amount of left pleural effusion (pre and post-insertion of left thoracostomy tube). Blood investigation revealed mild leukocytosis, ESR 72 mm/hr, hs-CRP 13.95 mg/dL, procalcitonin 2.2 ng/mL. The serology tests including HIV and hepatitis B and C were unremarkable.
Relevant Catheterization Findings
Interventional Management
Procedural Step
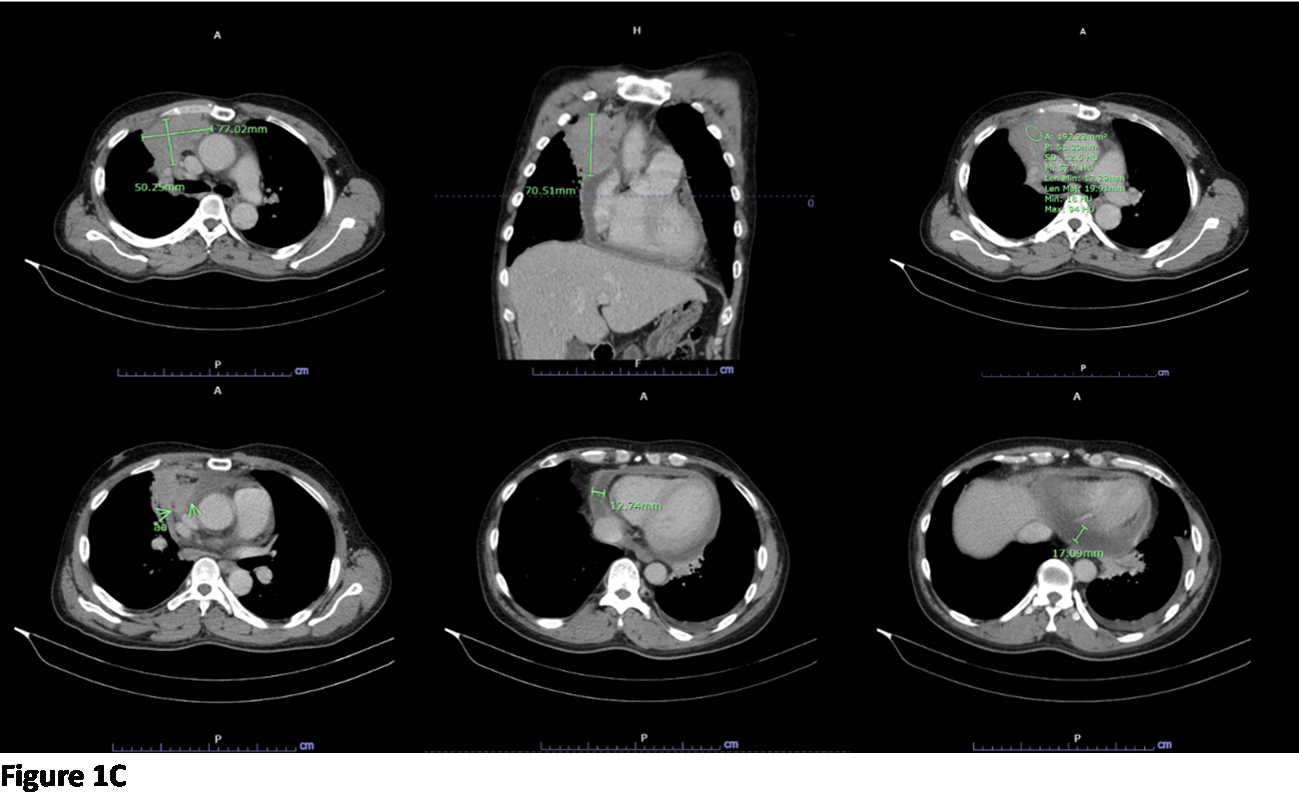
Transthoracic echocardiogram showing constrictive pericarditis, and extracardiac mass compression to left atrium. Thoracentesis was obtained for diagnosis and the left thoracostomy tube was inserted for further drainage of the collection for a total of 3 weeks and underwent successful talc pleurodesis. Pleural fluid examination revealed a yellow appearance with an exudative profile and cell counts showed red blood cells 3,700/mm3, and white blood cells 1,922/mm3, with 73% lymphocytes, and 23% neutrophils. Also, the definite diagnosis of constrictive pericarditis was confirmed by heart catheterization. Intravenous piperacillin-tazobactam was initiated for about 2 weeks and then switched to cefazolin for 1 more week duration due to septic workup including pus, pleural fluid, and hemocultures were negative. His clinical was improved, also procalcitonin level was decreased, and deemed suitable for outpatient management with continuation of oral amoxicillin/clavulanic acid for 10 days. Finally, the pathological report of soft tissue from the anterior right chest wall biopsy showed the presence of Actinomyces spp. supported his diagnosis of pericardial actinomycosis, likely due to mediastinal infiltration from lung infection. Then he lost follow-up for 3 months but finally came to repeated thoracic CT that showed improvement of the disease. He reported no clinical of heart failure. He denied taking any medication or any hospitalization during his loss follow-up period.


Case Summary
Cardiac actinomycosis is rare, 80% have an infection of the pericardium, and usually arises from the contiguous spread. It has no preference for age, race, season, occupation, underlying disease, or immunocompromised status. Factors associated with pericardial actinomycosis include dental disease and alcohol abuse. The traditional treatment is high-dose penicillin for a prolonged period (6 months to 1 year). Compared with our patient has only received a short course of antibiotics with primality treatment was found to drain the collection. The disease might have been relapsed with not surprising but the improvement of the disease by CT imaging was impressive.