
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-124
Failure in Passing a 1-Millimeter-Wide Balloon Through the Stent Strut: What to Do Next?
By Chih-Yang Lin, Feng Yu Kuo
Presenter
Chih-Yang Lin
Authors
Chih-Yang Lin1, Feng Yu Kuo1
Affiliation
Kaohsiung Veterans General Hospital, Taiwan1,
View Study Report
TCTAP C-124
Coronary - Complication Management
Failure in Passing a 1-Millimeter-Wide Balloon Through the Stent Strut: What to Do Next?
Chih-Yang Lin1, Feng Yu Kuo1
Kaohsiung Veterans General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 70-year-old man with dyslipidemia presented with intermittent exertional chest tightness and dyspnea for 6 months. He was an ex-smoker of 0.5 pack/day for 40 years and had quitted 10 years ago. The LDL level was poorly controlled (143 mg/dL). No cardiovascular disease were running in his family. He reported no other discomforts, such as cold sweating or radiating pain.
Relevant Test Results Prior to Catheterization
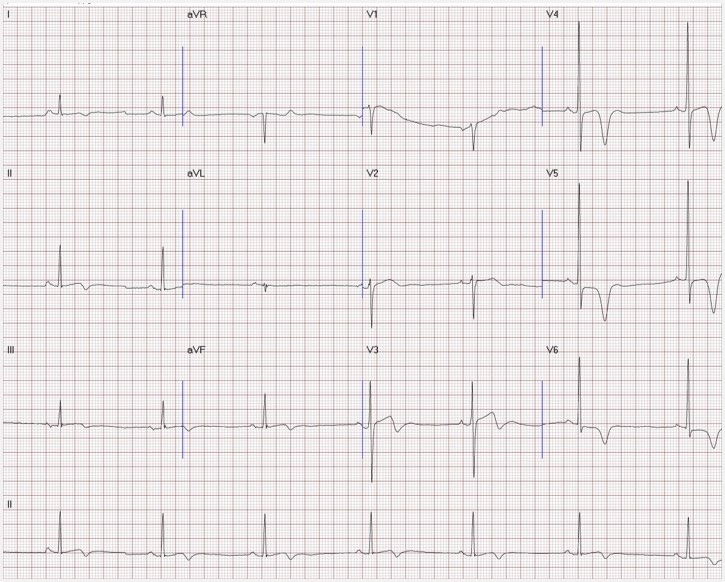
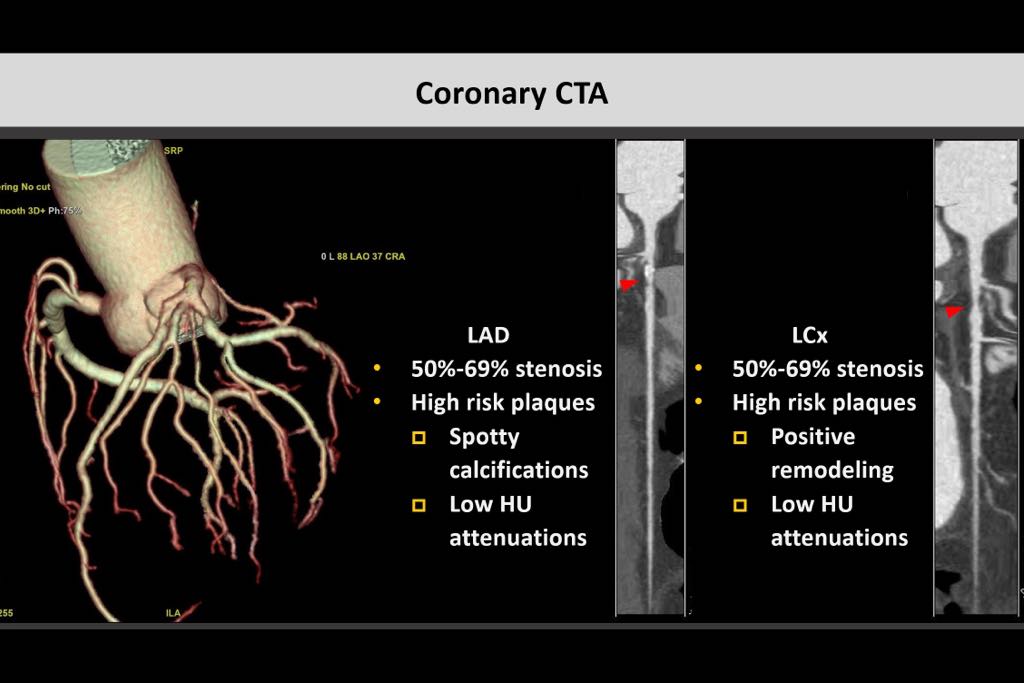
Electrocardiography showed sinus bradycardia with ventricular rate of 42 bpm and T wave inversion over V4-V6. Echocardiography reported preserved LV ejection fraction. Coronary CT angiography disclosed high risk plaque over proximal LAD with near 70% stenosis.
Relevant Catheterization Findings

Interventional Management
Procedural Step
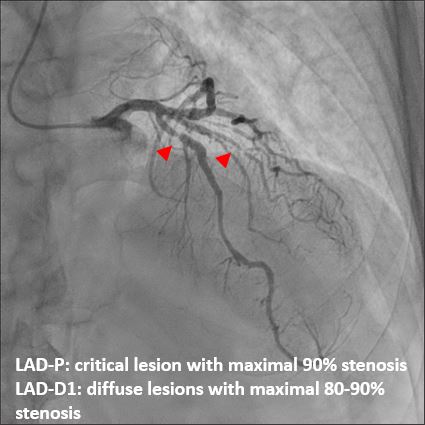
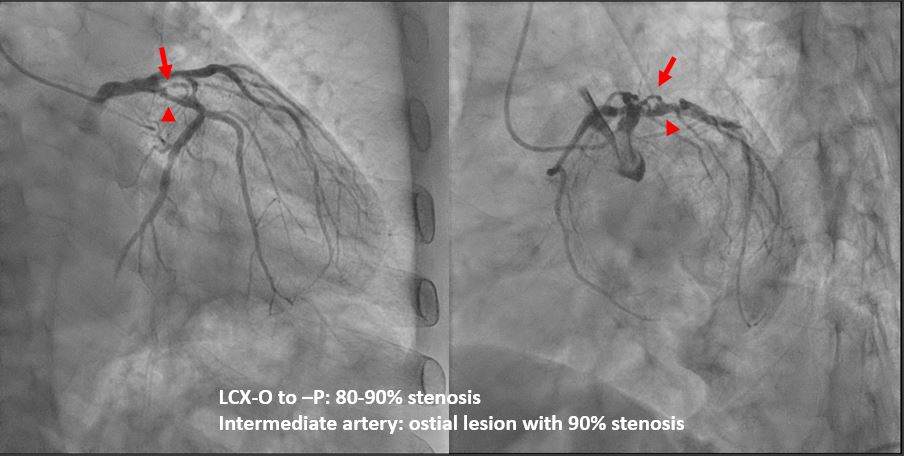
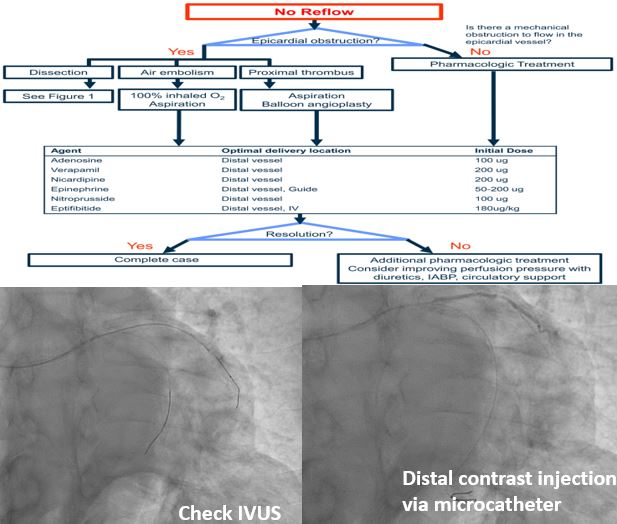
Wiring, pre-dilation, and then stenting of LAD-D1 with 2.25x34mm DES and LAD-P with 3.5x18mm DES were smooth. For LCX-P lesion, wiring of the LCX main branch with Runthrough was performed, which was followed by wiring of intermediate artery with Fielder FC for side branch protection. POBA of the ostial lesion of the intermediate artery with 1.25x10mm balloon was performed, following with pre-dilatation of LCX-P and then stenting with 3.5x14mm DES. Loss of intermediate artery ensued. Abrupt chest pain accompanying with cold sweating was complained. Blunt re-wiring with Fielder FC was attempted first and seemed successful. However, even 1.0mm balloon failed to pass the LCX-P stent strut. Re-wiring again with Sasuke microcatheter was successful. POBA of intermediate artery with 2.0mm balloon for near the whole side branch was performed but still TIMI 0-1 flow noted. IVUS showed no severe dissection, intramural hematoma, or mechanical thrombus. Distal contrast injection via microcatheter showed still delayed and near backward flow but without apparent distal emboli. True no-reflow (microvascular dysfunction) was impressed. Repeated low dose adenosine was injected into the distal coronary vascular bed via microcatheter for 8 times. There was no worsening of bradycardia. Final TIMI 2-3 flow was restored, along with resolution of the chest pain.


Case Summary
When facing with difficulty in equipment delivery or even entrapment, pulling back strongly or a hard push were not recommended. Take a closer look and figure out the mechanism behind the failure is crucial to a successful procedure. Besides, abrupt vessel closure is a troublesome and sometimes lethal situation. It is essential to make a quick differential between mechanical obstruction and true no-reflow to be able to act accordingly and promptly.