
Lots of interesting abstracts and cases were submitted for TCTAP 2024. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-039
Pandora Box: Chronic Total Occlusion and Severe Calcified Lesion
By Mohd Ruslan Mustapa, Muhamad Ali SK Abdul Kader
Presenter
Mohd Ruslan Mustapa
Authors
Mohd Ruslan Mustapa1, Muhamad Ali SK Abdul Kader1
Affiliation
Sultan Idris Shah Serdang Hospital, Malaysia1,
View Study Report
TCTAP C-039
Coronary - Complex PCI - Calcified Lesion
Pandora Box: Chronic Total Occlusion and Severe Calcified Lesion
Mohd Ruslan Mustapa1, Muhamad Ali SK Abdul Kader1
Sultan Idris Shah Serdang Hospital, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
A 47 year old male with history of AF on Rivaroxaban presented for chronic coronary syndrome. His CCS score was 2 and occasional complaint of reduced effort tolerance upon exertion. He is an ex-smoker. His vital signs are stable, other systemic examination unremarkable. He was scheduled for routine coronary angiogram.


Relevant Test Results Prior to Catheterization
ECG revealed rate-controlled AF at 70bpm. Echo done showed EF 50% with no RWMA. Valves are normal with no pericardial effusion. Baseline investigations demonstrated haemoglobin 14.2g/dL, platelet 186,000 and creatinine 72mmol/L.
Relevant Catheterization Findings
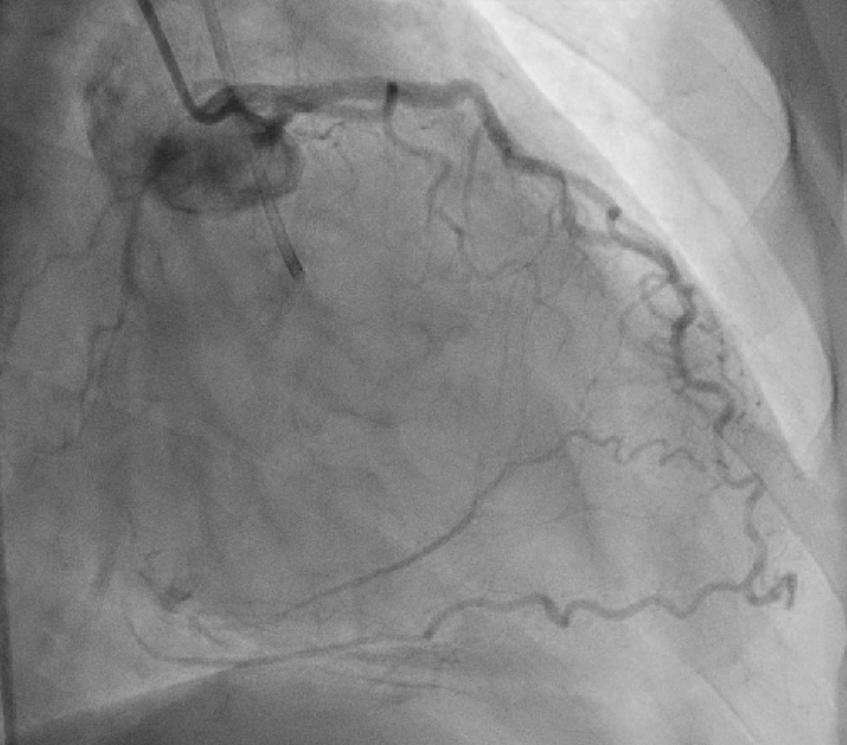
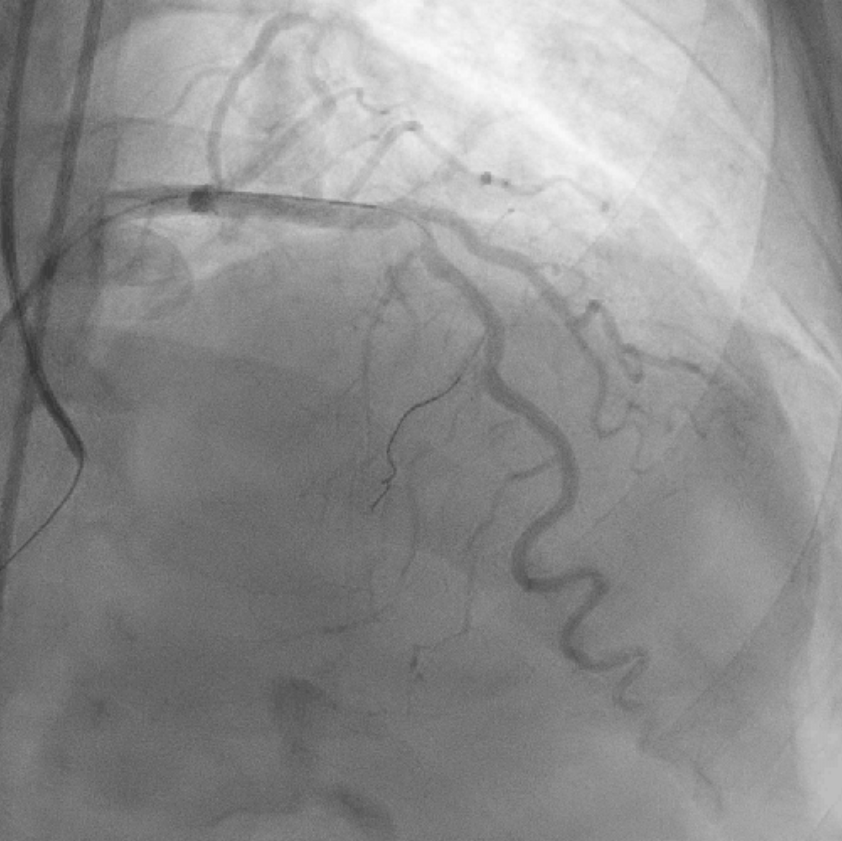
Diagnostic angiogram revealed normal LM. Mid LAD 80% stenosis and smooth LCx. RCA is dominant. Calcified, 90% stenosis proximal RCA and mid CTO with collaterals from the left system.
Interventional Management
Procedural Step
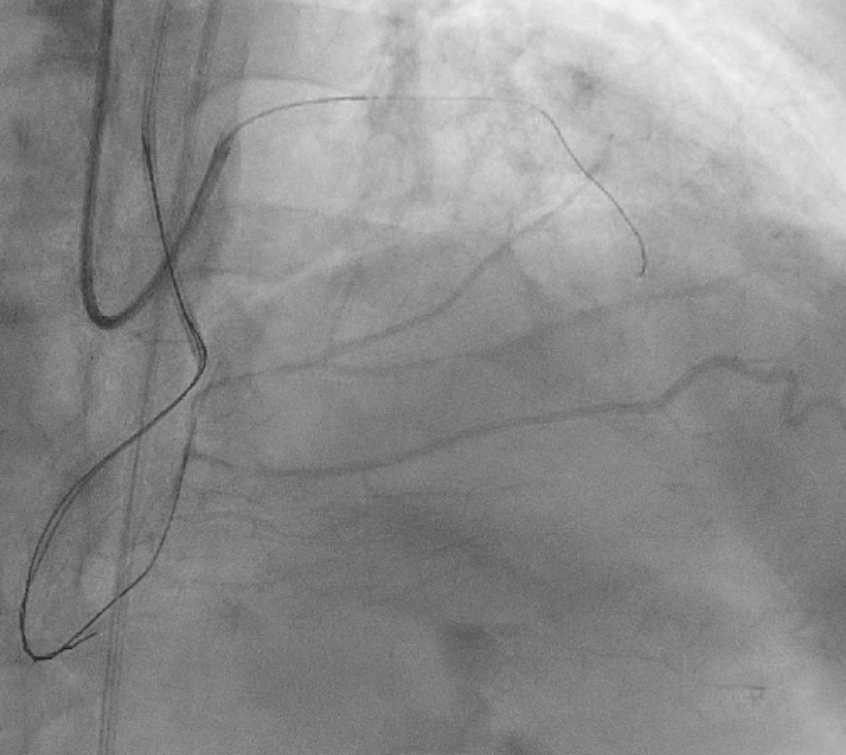
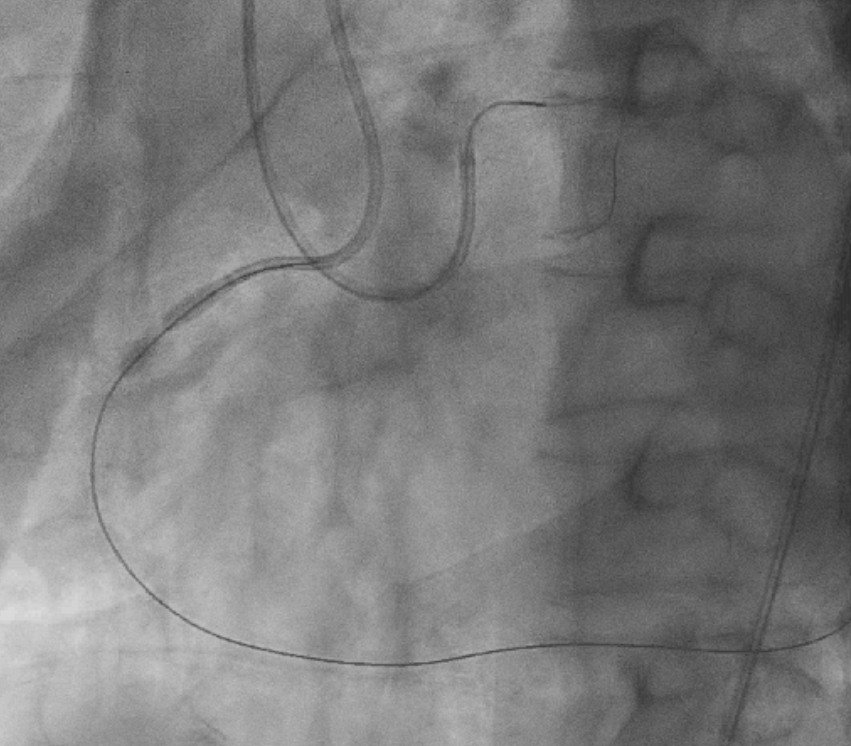
RRA and RFA access. 6Fr EBU 3.0 and 6Fr AL1.0 respectively. Plan for PCI RCA CTO with antegrade approach. Fielder XT-R in Finecross and then upgrade to Gaia Next2 but the wire keeps going into subintimal. Change for retrograde with Suoh 03 and Corsair Pro. All the septal attempted but failed to cross due to calcified tortuosity. Re-attempt the antegrade with Gaia 2nd and Conquest Pro12 parallel wire technique and crossed to distal PLV. Guidezilla used but can’t pass the proximal segment. Ryurei 1.0/5 used to predilate from distal to proximal. Sequential with Ryurei 2.5/12 but can’t open well at 20ATM and burst due to calcium nodule at proximal RCA. Next Ryurei 3.0/15 used but unable to pass through. Due to multiple dissection decided for IVL 3.5/12 and followed by Wolverine 3.0/10 which both can’t pass through. Sequentially predilate again with Ryurei 1.0/5 and 2.0/10 both at 20ATM. However proximal lesion still not open. Decided to Rotablator with 1.5burr at 180K RPM. At first attempt the burr trapped and removed en bloc. RCA re-engage and rotablation resume for another 3 runs. Lesion then prepared with Wolverine 3.0/10 and IVL 3.5/12 (7 cycles). PCI to PLV with Sequent Please Neo 2.5/40 at 16ATM for 60s, mid RCA with DES Supraflex Cruz 2.5/40, and prox RCA with 4.0/48. Postdilate mid RCA with Accuforce 3.5/15 and proximal with Sapphire NC4.5/15 at 16-24ATM respectively. Final results with TIMI 3 flow and non-limiting flow dissection at distal RCA.
Case Summary
Echocardiography inpatient showed preserved EF with no pericardial effusion. Patient was well post PCI and discharged after 2 days. His medications optimized to attend his risk factors. He was planned for stage LAD in 2 months.